Article Text

Abstract
Objectives The aim of this study was to evaluate changes in the uptake of intrathecal baclofen (ITB) following commissioning of this therapy by the National Health Service (NHS) England in April 2013. The specific objectives of this study were: (i) to explore the gap between the need for and the actual provision of ITB services; and (ii) to compare England figures with other European countries with comparable data available.
Setting Data for ITB -related procedures were obtained from the Hospital Episode Statistics (HES) database from 2009/2010 to 2013/2014.
Participants Patients receiving ITB for the management of spasticity.
Results The available data for implantation of ITB from 2009/2010 to 2013/2014 for the treatment of spasticity due to varied aetiologies show that there has not been an increase in uptake of this therapy. The estimated need for this treatment based on the incidence and prevalence of conditions susceptible to ITB therapy is between 4.6 and 5.7 per million population. Our analysis of the data available from the HES database showed that the actual number of implants is around 3.0 per million population. The same period 2009–2014 has seen an increase in the delivery of other neuromodulation techniques including spinal cord stimulation, deep brain stimulation and sacral nerve stimulation.
Conclusions There is a considerable gap between the need for and provision of ITB figures nationally. Additionally, within the same area, we have observed important differences in the ITB service delivery between the various trusts. The reasons for this can be multifactorial, including individual experience and opinions, organisational structures, resource and financial limitations. Further research analysing the efficacy and cost-effectiveness of this treatment in the UK might inform the development of Technology Appraisal Guidance for ITB, potentially leading to an improvement in service provision.
- Spasticity
- Intrathecal baclofen
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study highlights a considerable gap in the number of intrathecal baclofen (ITB) pump implants performed and the estimated need for the service despite the National Health Service England's commissioning of ITB.
Important differences in the ITB service delivery across England have been identified and possible reasons are provided.
English ITB uptake data is compared with appropriate equivalent data from other European countries.
These findings are based on data extracted from the Hospital Episodes Statistics database which relies on hospital-coded data on procedures and indications.
Introduction
Spasticity is a significant health problem in a subgroup of patients with multiple sclerosis, spinal cord injury, cerebral palsy and traumatic brain injury. This ailment is characterised by a motor disorder with increased resistance to velocity-dependent passive stretch that can be generalised or confined to a particular group of muscles. Spasticity has been defined as “disordered sensorimotor control resulting from an upper motor neuron (UMN) lesion, presenting as intermittent or sustained involuntary activation of muscles.”1 This syndrome can affect daily activities including mobility and ability to transfer, and can lead to incontinence complicated by pressure sores, skin breakdown and infection. It can also cause pain, discomfort, contractures, sleep disturbances and, consequently, mood disorders.
Spasticity can be differentiated on the basis of aetiology as spinal (eg, multiple sclerosis, spinal cord injury, transverse myelitis) and central spasticity (stroke, cerebral palsy, acute brain injury). The aim of treatments for spasticity includes improving the range of motion, mobility, facilitating the manual handling of patients, preventing contractures and achieving self-care and independence.
There are various existing therapies for the management of spasticity including physical therapy, botulinum injections and muscle relaxants. The muscle relaxants in common use are baclofen, tizanidine and dantrolene. Among these, baclofen is the most commonly used.
Intrathecal drug delivery (ITDD) facilitates the direct administration of drugs at a site of action, which allows for the use of lower doses of the drugs, thereby reducing their side effects while achieving maximum therapeutic benefit. Intrathecal baclofen (ITB) therapy is an effective alternative for the management of spasticity in patients in whom other treatment options (pharmacological agents, non-pharmacological adjuvants) have failed to provide adequate relief of symptoms, or for patients who derive benefit from oral or systemic medications but for whom the side effects have become intolerable.
Since April 2013, there have been major changes in the way services are commissioned in the National Health Service (NHS). Primary Care Trusts, which used to commission most NHS services and controlled 80% of the NHS budget, have been replaced by Clinical Commissioning Groups (CCGs). CCGs can commission any service provider that meets NHS standards and costs by taking into account the National Institute for Health and Care Excellence (NICE) guidelines and the Care Quality Commission’s (CQC) data about service providers. NHS England, formerly the NHS Commissioning Board (NHS CB), oversees the operation and allocates resources to CCGs.2
In April 2013, the NHS CB published a document on clinical commissioning policy for ITB.3 It states that the aim of the therapy is to improve passive and/or active functioning and to prevent deformities resulting from fixed contractures. ITB therapy should not be used simply to reduce tone and improve the range of motion. The aim of this study is to explore the impact of NHS England's commissioning on the uptake of ITB for the management of spasticity.
Methods
Data for ITB procedural activity during the years 2009/2010 to 2013/2014 were obtained from the Hospital Episode Statistics (HES) database4 using the QUANTIS system via NHiS.5 HES is a national statistical data warehouse for England for care provided by NHS hospitals. QUANTIS is a database of NHS and social care numerical data for the UK, and NHiS is a vendor that provides subscribed access to the QUANTIS database.
We examined OPCS-4 procedure codes A54.3 (implantation of ITDD device adjacent to spinal cord), A54.4 (attention to ITDD device adjacent to spinal cord), A54.5 (removal of ITDD device adjacent to spinal cord). OPCS code 54.4 does not allow for a clear differentiation between refills, catheter revision and pump replacements.
The relevant OPCS codes were filtered by indication to ensure that only spasticity due to spinal and supraspinal origin indication were included. This eliminated any inclusion of other indications for insertion of ITDD system such as malignant and non-malignant pain.
Insertion of ITDD system uptake is expressed per million population across each strategic health authority region in England.
We compared English ITB uptake data (code A54.3 only) with European countries where we were able to source the appropriate equivalent data, that is, France, Belgium, Germany and The Netherlands.
Results
The HES data analysis between the years 2009 and 2014 show the activity trend for procedure codes A54.3, A54.4 and A54.5 (table 1). This shows minimal fluctuation in the uptake for any of these procedures except for a small increase in A54.4. Continuing increases in procedure code A54.4 are to be expected, as there are more new implants per year than devices explanted, thereby resulting in an increasing number of pump refill procedures.
Total number of intrathecal pump procedures from 2009 to 2014
There is considerable variation in the rate of uptake of ITDD service between the various CCGs (figure 1). Additionally, within the same area, there have been important differences in the ITDD service delivery between the various trusts.

Number of intrathecal drug delivery implants per million population for 87 Clinical Commissioning Groups (CCGs) in 2013–2014. In total 117 CCGs performed between 1 and 5 implants per million; 7 CCGs did not perform any implants.
The variation in access to ITDD therapy during 2013/2014 is also noticeable across the different strategic area teams indicating inequality in access to this treatment (figure 2).
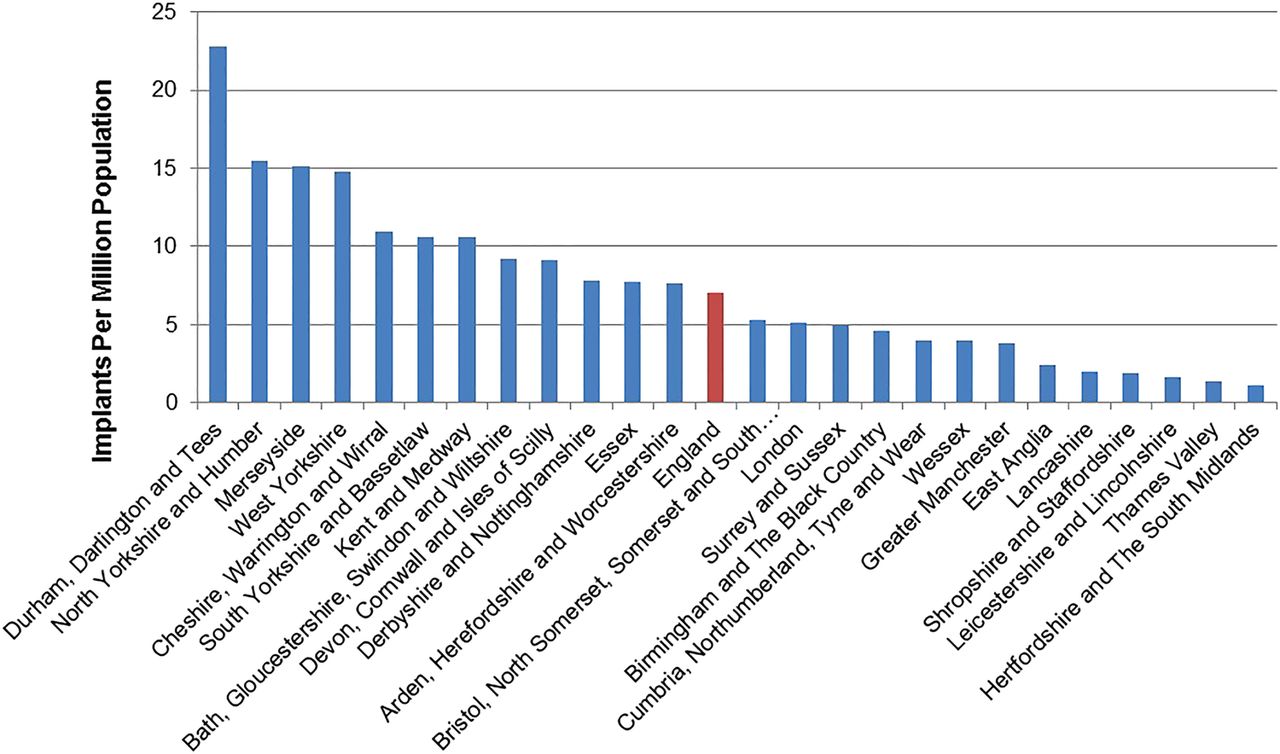
Number of intrathecal drug delivery implants per million population for each Area Team in 2013–2014. Where numbers were masked for patient confidentiality (between 1 and 5 procedures), 3 was used as an estimation in order that the rate per million could be calculated.
NHS England records from 2009 to 2014 suggest that while there has been an increase in the uptake of other neuromodulation modalities, it would appear that ITB has not attracted as great an interest among clinicians (figure 3).

{kind=link}
{kind=link}
{kind=link}
Total neuromodulation implant procedures from 2009 to 2014. DBS, deep brain stimulation; ITB, intrathecal baclofen; NHS, National Health Service; SCS, spinal cord stimulation; SNS, sacral nerve stimulation.
The total number of intrathecal pumps implanted in England for the year 2013/2014 was 394 for spasticity and chronic pain (table 2). According to HES data, the number of intrathecal pumps implanted in the years 2013/2014 for spasticity were 194 (3.08 per million).
Total number of intrathecal drug delivery implants for spasticity and other indications
Table 3 shows that the estimated incidence of ITB suitable cases annually is around 4.6–5.7 per million population. There is a considerable gap between the recommended figures and the actual implanted figures nationally. Even with the assumption that the other indications were all ITB pumps (276 pumps for 2013/2014), still it would be 4.38 per million population, less than the minimum recommended figures.
Estimated incidence and prevalence of conditions potentially suitable for intrathecal baclofen (ITB)
ITDD implants performed for spasticity in European countries where data were available indicated the following number of implants per million: Belgium—16.3, France—1.72, The Netherlands—3.1 and Germany—13.12.7
Discussion
Baclofen is a γ-aminobutyric acid (GABA) agonist primarily used to treat spasticity. Spasticity results from an imbalance of supraspinal inhibitory and excitatory inputs, producing a state of net disinhibition of the spinal reflexes. Baclofen acts by resetting this imbalance via GABA B (GABAB) receptors. The GABAB receptor is distributed in the central nervous system in high density in the dorsal horn of the spinal cord, the thalamic nuclei, the cerebellum, the interpeduncular nucleus and the cerebral cortex. Baclofen is well absorbed orally, but because of its hydrophilic nature, it crosses the blood–brain barrier poorly. It is equally distributed between spinal and supratentorial compartments leading to side effects such as nausea, drowsiness, sedation and fatigue. ITB facilitates direct infusion of the drug at the site of action at a fraction of the oral dose, thereby minimising the risks of adverse effects.
ITB for spasticity was first described in 1985.8 Since then, there have been numerous published studies demonstrating its efficacy in the treatment of spasticity, spasm-related pain and improved quality of life in patients with spasticity of spinal and supraspinal origins.9–14
Ordia et al9 conducted a prospective case series of 131 patients treated with ITB for spasticity of spinal origin. Significant reductions in the Ashworth and spasm scores at a mean follow-up of 73 months (range of 2–137 months) were reported. Improvements in gait and balance, reduction detrusor hyper-reflexia, reduced need for urinary catheterisation and improved speech in patients with oropharyngeal muscle involvement were also observed. There were 24 catheter-related complications and 34 drug-related occurrences.
A prospective multicentre ITB case series with a 3-year follow-up in 64 patients with spasticity of spinal origin identified a decrease in the Ashworth scale greater than two points and a reduction in spasm score.10 These results were sustained at 3 years. Greater improvements were observed in patients under 25 and/or with complete spinal cord injury. Although observed, improvements in functional outcome were not quantified. Drug-related or catheter-related complications occurred in 19/64 (30%) patients.
An observational study with a follow-up ranging from 12 months to 10 years observed significant improvements in the Ashworth score, spasm score and functional outcome in 18 patients with spasticity of supraspinal origin.11 The efficacy of ITB therapy in children suffering from spasticity has also been observed.12 ,15–17
Economic evaluations have suggested ITB to be a cost-effective alternative when compared with other treatment modalities.13 ,14 ,18 Including ITB as a first-option strategy in the management of function of severely impaired patients with disabling spasticity resulted in a higher success rate (78.7% vs 59.3%) when compared with a range of alternative strategies, such as sequential combinations of physical treatment, oral or focal treatment, or surgery or nursing using a mathematical simulation model.13 In addition, the ITB therapy model revealed a lower medical cost (€59 391 vs €88 272) over a 2-year time horizon, and an overall favourable cost-effectiveness ratio (€75 204/success vs €148 822/success) when compared with conventional medical management without ITB. In another study, de Lissovoy et al14 used mathematical modelling and computer simulation to estimate the incremental cost per quality-adjusted life-year (QALY) for identical cohorts of children treated with ITB or alternative therapy over a 5-year time horizon. The incremental cost-effectiveness ratio was calculated to be $42 000 per QALY (approximately £26 588), a figure considered as cost-effective, considering the willingness-to-pay threshold in the UK of between £20 000 and £30 000 per QALY. A systematic review evaluating the effect of continuous ITB infusion on function and quality of life in patients with severe spasticity concluded that ITB has a cost per QALY in the region of £6900–£12 800.18
This study suggests that despite the available evidence on effectiveness and cost-effectiveness, and although NHS England has issued a policy statement on ITB, there are still many patients who have not been able to access this therapy. We believe this to be related to the complexity of the set-up required to deliver the therapy and the need for interaction between a number of specialties, including neurosurgery, pain medicine, neurorehabilitation and spinal injuries, all of which may not be present on the same hospital site. The creation of specialist centres will and should overcome this problem in the future, although estimating the duration for the impact of specialised centres is difficult at this point. In comparison with other Western European countries, the UK is one of the lowest providers of ITB therapy. However, the data are available for other European countries for only 1 year, and therefore we cannot comment on trends. There is also a considerable variation in provision of services among various CCGs. The number of implants performed in the North of England commissioning region was 148 compared with 62 and 70 in the Midlands and South of England commissioning regions during the years 2012/2013. The number of implants cannot be explained based on population factors; the population figures are much higher for the South (27,830,219) than the North (15,845,124) and Midlands (12,694,544). We can only speculate that the differences may relate to several factors including a number of high-volume implanting centres based in the North of England. In addition, the variations in commissioning between CCGs may be explained by the individual ITB commissioning policies of the CCG precursors (the Primary Care Trusts) with more permissive Primary Care Trust policies towards implant of ITB pumps in the North than in the South or Midlands. It has previously been observed that commissioning policies varied vastly between Primary Care Trusts in respect to SCS commissioning.19 The Right Care20 is one of the national work streams in the DH Quality Innovation Productivity and Prevention programme which identifies unwarranted variation in NHS treatments based on geographical areas. One of the Right Care objectives for 2011–2012 is to minimise this unwarranted variation and maximise value. Value can be increased by improving quality, optimising resource utilisation and ensuring that patients receive appropriate interventions. Direction of commissioning towards specialised centres may lead to an improvement in uptake.
There may be several reasons for this inequality in or lack of service provision. The care of patients suffering from spasticity due to various causes is shared between specialties and requires service coordination and management. There is a continuing shortfall of resources and funding of rehabilitation services with ever increasing demand on these services as well as lack of coordinated service provision between a number of specialties. Finally, there may be an element of reluctance to adopt a new technology, particularly if the latter is invasive involving a permanent implantation. This reluctance may be due to perception of harm and perceived high level of complications despite published articles supporting the safety and efficacy of this treatment.21 With lack of resources, there are ever increasing challenges in setting up a new service and the increasing scrutiny of cost-effectiveness.
Conclusion
Our study shows that there is a considerable gap in the number of ITB pump implants performed and the estimated need for the service. We also lag behind our European counterparts in provision of the treatment, which can potentially relieve the symptoms and improve the quality of life in patients suffering from these conditions. There is a need to establish a service commitment to these patients by improving our multidisciplinary approach, education of those who provide care for these patients, and laying down referral pathways to the ITB service. The clinical commissioning policy for ITB therapy published recently can provide a pathway to improve uptake of this service.
Acknowledgments
The authors are grateful to Sophie Barnett, Medtronic UK, for extracting the relevant Hospital Episode Statistics data.
References
Footnotes
Contributors All authors had an integral role in producing this manuscript and have made substantial contributions to the analysis of data (RCN, AV); interpretation of data (RCN, RVD, AV, SE); drafting (RCN, RVD); revision of the article (AV, SE); and approval of the final version of the manuscript (RCN, RVD, AV, SE).
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SE has done consulting for Medtronic UK. AV is an employee of Medtronic UK.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.