Article Text

Abstract
Introduction Infective endocarditis (IE) is among the most serious infectious diseases in the western world. Treatment requires lengthy hospitalisation, high-dosage antibiotic therapy and possible valve replacement surgery. Despite advances in treatment, the 1-year mortality remains at 20–40%. Studies indicate that patients experience persisting physical symptoms, diminished quality of life and difficulties returning to work up to a year postdischarge. No studies investigating the effects of rehabilitation have been published. We present the rationale and design of the CopenHeartIE trial, which investigates the effect of comprehensive cardiac rehabilitation versus usual care for patients treated for IE.
Methods and analysis We will conduct a randomised clinical trial to investigate the effects of comprehensive cardiac rehabilitation versus usual care on the physical and psychosocial functioning of patients treated for IE. The trial is a multicentre, parallel design trial with 1 : 1 individual randomisation to either the intervention or control group. The intervention consists of five psychoeducational consultations provided by specialised nurses and a 12-week exercise training programme. The primary outcome is mental health (MH) measured by the standardised Short Form 36 (SF-36). The secondary outcome is peak oxygen uptake measured by the bicycle ergospirometry test. Furthermore, a number of exploratory analyses will be performed. Based on sample size calculation, 150 patients treated for left-sided (native or prosthetic valve) or cardiac device endocarditis will be included in the trial. A qualitative and a survey-based complementary study will be undertaken, to investigate postdischarge experiences of the patients. A qualitative postintervention study will explore rehabilitation participation experiences.
Ethics and dissemination The study complies with the Declaration of Helsinki and was approved by the regional research ethics committee (no H-1-2011-129) and the Danish Data Protection Agency (no 2007-58-0015). Study findings will be disseminated widely through peer-reviewed publications and conference presentations.
Registration Clinicaltrials.gov identifier: NCT01512615.
- Infective Endocarditis
- RCT
- Mixed Method
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
The CopenHeartIE trial is a randomised clinical trial investigating the effects of comprehensive cardiac rehabilitation versus usual care for patients treated for infective endocarditis (IE).
-
The hypothesis is that comprehensive cardiac rehabilitation improves mental health (MH) and physical capacity.
-
Using a mixed method approach, a broad range of outcome measures is collected to evaluate the intervention.
Key messages
-
Infective endocarditis (IE) is a life-threatening disease. Patients experience severe deconditioning and diminished quality of life postdischarge.
-
Studies exploring the effects of rehabilitation of patients treated for IE have not been published.
-
This trial is the first to examine physical functioning (PF) and to test a comprehensive rehabilitation programme on a large population of patients treated for IE. CopenHeartIE will provide much-needed evidence and insight into the postdischarge status and rehabilitation needs of patients treated for IE.
Strengths and limitations of this study
-
The study has been designed to meet the criteria for high quality in non-pharmacological randomised clinical trials with central randomisation, multicentre participation, blinded assessment and analysis.
-
We are aware of the subjective nature of the mental-health component subscale (primary outcome). Accordingly, we will interpret the findings conservatively.
Background
Infective endocarditis (IE) is an infection of the heart valves and/or adjacent structures. The bacteria may invade and destroy the tissue, and vegetations can dislodge into circulation and cause harmful and potentially deadly complications. Despite improvements in diagnostic tools, novel antibiotics and changes in treatment regimens, the mortality of IE remains high.1–3 The incidence of IE in the developed countries is currently between 1.9 and 10.0 per 100 000 people/year,3 ,4 and is rising due to the increase in degenerative valvular disease in the elderly, increasing insertions of prosthetic valves and implantable cardiac devices, and exposure to invasive procedures and nosocomial bacteraemia.1 ,5–7 In Denmark, the incidence is at least 10 per 100 000 people/year, equivalent to approximately 500 patients/year.4 The treatment includes a lengthy hospitalisation with intravenous antibiotic therapy, extensive invasive and non-invasive diagnostic procedures and, in about 50% of the patients, valve replacement surgery.4 The in-hospital death rate of patients with IE is 10–25%, between 20% and 40% at 1-year postdischarge and up to 50% at 10 years postdischarge.3 ,8–11 The causes of postdischarge mortality are still poorly understood.
Health and quality of life
The disease, its treatments and the potential complications can lead to massive deconditioning of the patients.12–15 The few existing studies on patient experiences after discharge, indicate that patients treated for IE have persisting physical and mental symptoms, such as fatigue in 47% of patients,14 physical weakness in up to 78% of patients14 ,15 and concentration problems and memory loss in up to 35% of patients.14 Patients also report diminished health-related quality of life,14 negatively affected perceived health12 ,13 and up to 55% experience anxiety and depression15 and 11% showed signs of post-traumatic stress disorder.14 Furthermore, 35% of previously employed patients had not returned to work after 12 months.14
Rehabilitation
Secondary prevention initiatives including cardiac rehabilitation, is widely recommended by the European Society of Cardiology (ESC).16 Although evidence of the efficacy is strong, cardiac rehabilitation is still poorly implemented and often only on selected populations, and thus the development of full comprehensive preventive programmes, according to the ESC, is warranted.17 Studies exploring the effects of rehabilitation of patients treated for IE are lacking. As there is no evidence of the efficacy, the provided rehabilitation is presumably often suboptimal or totally lacking. Lessons, however, might be learned from rehabilitation studies in patients with related cardiac conditions. The positive effects of cardiac rehabilitation have been well documented, particularly in patients with coronary heart disease (CHD) and heart failure (HF), where rehabilitation has been proven to reduce hospital re-admissions and mortality in a cost-effective way,18 ,19 as well as improve quality of life.20 More specifically, studies on the effect of exercise training have demonstrated an increase in exercise capacity of up to 38% in patients after valve replacement surgery21 and an increase in peak VO2 of 2.3±2.2 (SD) ml/kg/min in the intervention group compared with −0.3±2.1 (SD) ml/kg/min in the control group as well as a significant change in quality of life in older patients with HF.22 Traditional cardiac rehabilitation has focused on physical training and standardised programmes, but studies indicate that individualised content and supervised exercise components are key design characteristics for improving outcomes.23 In addition to exercise training, evidence support interventions including patient education, which in patients with CHD has been shown to improve health-related quality of life and decrease healthcare costs24 and psychological support, which has been shown to improve psychological symptoms in patients with CHD, such as depression and anxiety.25 Evidence on the efficacy of comprehensive interventions for patients treated for IE, however, is needed. Based on the effects of rehabilitation in other cardiac conditions, we hypothesise that patients treated for IE can benefit from participating in a rehabilitation programme, consisting of an individualised exercise training programme and a psychoeducational intervention. Therefore, we have designed the CopenHeartIE trial.
Study objectives
The aim of the trial is to test a comprehensive cardiac rehabilitation programme for patients treated for IE versus usual care. The programme consists of a psychoeducational component and an exercise-training component. The primary hypothesis is that comprehensive cardiac rehabilitation improves mental health (MH), measured by the mental component scale (MCS) of the Short Form 36 (SF-36) questionnaire, in patients treated for IE with six points (13%) in the intervention group compared with the control group after the completed intervention. The estimated 13% increase in primary outcome is based on a study on ICD recipients with a comparable complex rehabilitation intervention which found a similar increase (unpublished data from the COPE-ICD trial26). The secondary hypothesis is that physical capacity, measured as peak oxygen uptake (VO2 peak) by the bicycle ergospirometry test, will be 3 ml/kg/min (20%) higher in the intervention group compared with the control group after 12 weeks of exercise training. Since no data on physical capacity exists on patients treated for IE, this hypothesis is based on rehabilitation studies including patients after heart valve surgery.27 ,28 Exploratory analyses will test the hypotheses that comprehensive cardiac rehabilitation improves self-rated health, quality of life, nutritional status, sleep quality and body image and reduces anxiety, depression and fatigue after 6, 12 and 24 months. Furthermore, we intend to assess whether comprehensive cardiac rehabilitation can reduce healthcare utilisation, work cessation and mortality and increase cost effectiveness after 24 months.
Design
The CopenHeartIE trial is part of the overall CopenHeart project, which is designed to develop evidence-based knowledge on rehabilitation among patients with complex cardiac conditions.29 The CopenHeartIE trial is a multicentre, multidisciplinary, randomised clinical trial designed to examine the effects of a comprehensive cardiac rehabilitation programme compared with usual care for patients treated for IE. In addition to this, the CopenHeartIE trial includes two complementary studies, aimed at investigating the postdischarge experiences and rehabilitation needs of patients treated for IE, and a qualitative postintervention study to explore the meaning of the CopenHeartIE rehabilitation programme from the patient's perspective. Accordingly, the trial combines quantitative and qualitative research methods. The premise of mixed methods research is that the use of qualitative and quantitative approaches in combination provides a better understanding of the research problems than either approach alone, because different types of questions require different types of data and that mixed methods research provides strengths that offset the weaknesses of both qualitative and quantitative research.30 The methods are integrated by applying the mixed method embedded experimental design and include qualitative data to develop the intervention and to examine the process of the intervention and the results of the trial (see figure 1).30 ,31 The rationale for this approach is that the quantitative findings provide a general understanding of the research problem through statistical results, and qualitative findings refine and explain the results by exploring participants’ views in greater detail. Evaluation using qualitative research methods is increasingly promoted in evidence-based rehabilitation.32–35 Qualitative research alongside randomised controlled trials can contribute in several ways to the development and evaluation of complex healthcare interventions and may be particularly useful in evaluating interventions that involve social and behavioural processes that are difficult to explore or capture using quantitative methods alone.36 As patient participation is paramount to the efficacy of the rehabilitation,37 we find it highly valuable to include the patients’ perspective in the development and evaluation of the intervention. This paper presents the study protocol for the CopenHeartIE randomised clinical trial. The complementary studies are briefly described in a separate section.

The CopenHeartIE study. Mixed method—embedded experimental model.
Study population and eligibility criteria
Consecutive patients treated for left-sided (native or prosthetic valve) or cardiac device endocarditis at the tertiary referral heart centres in Copenhagen, Denmark (Rigshospitalet and Gentofte Hospital) will be screened for inclusion and approached for study participation. The patients aged 18 years or older, having completed treatment for IE based on the Duke Criteria,38 speaking and understanding Danish and providing written informed consent will be considered eligible for participation. The patients unable to understand study instructions, with a cardiac ischaemic event within the past 6 months, who are pregnant or breastfeeding, with reduced ability to follow the planned programme due to, for example, substance abuse problems or other somatic illness, with considerable illness in the musculoskeletal system or with physical disability which complicates exercise training or patients whose physician advise against participation, will be excluded.
Study procedure, randomisation and follow-up
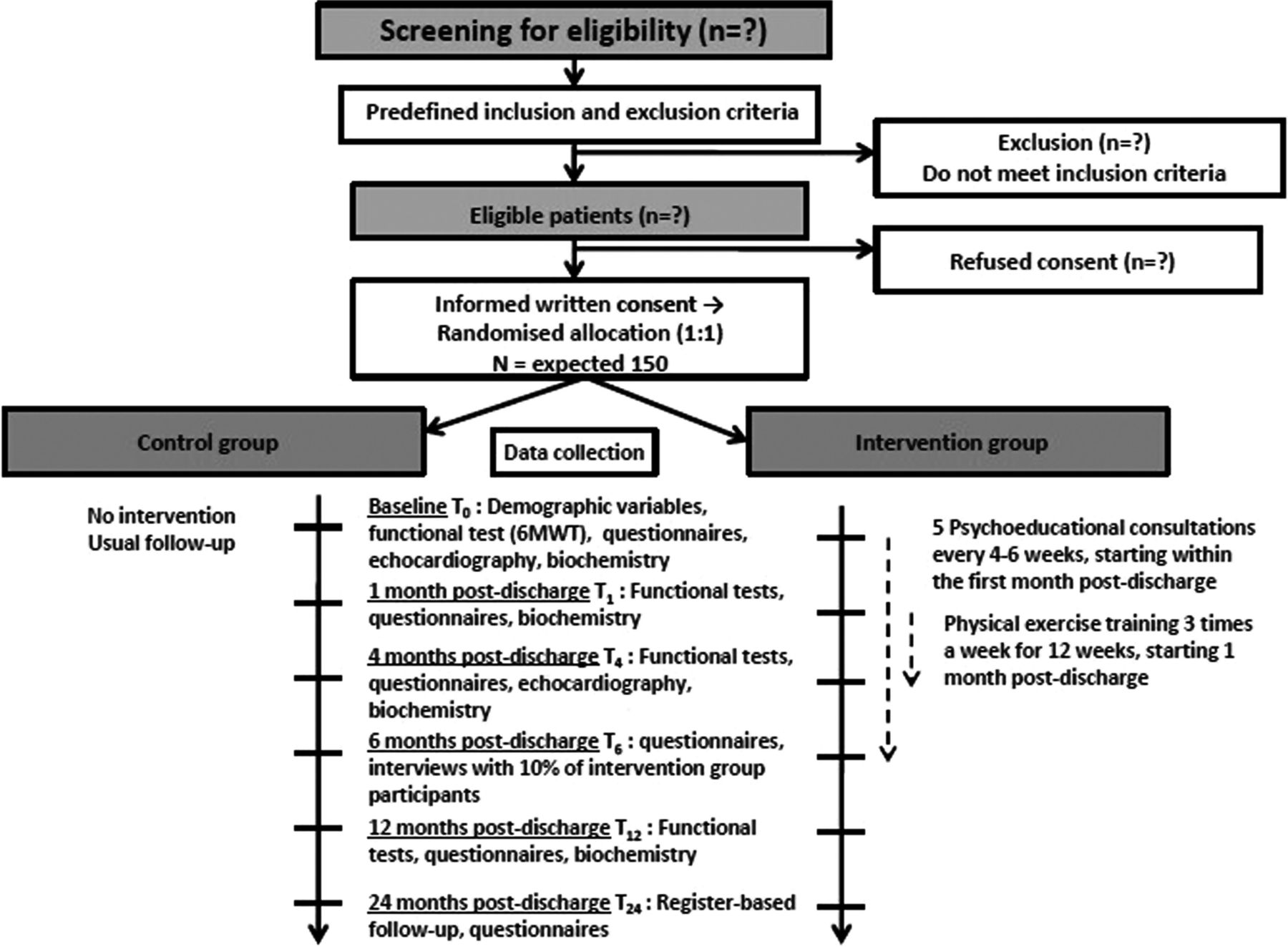
Patients eligible for participation will be approached by a nurse or a physician from the research group during the expected last week of their treatment for IE. A brief oral introduction is initially given together with written information describing the study and implications for the patient in detail. The patient is given ample time to read the information and if necessary involve a relative in the decision making. The enrolling nurse or physician will return within 2–3 days or at a planned time to answer any questions the patient or their relative might have. The patient should subsequently be able to provide informed consent or reject participation. When the informed consent form is signed attained, baseline data will be collected including the baseline questionnaire package, demographic variables and clinical characteristics. After baseline data collection, central randomisation is conducted by telephoning the trial coordinating centre, Copenhagen Trial Unit (http://www.ctu.dk/), for randomised allocation. The allocation sequence will be computer-generated with varying block sizes, blinded to investigators, randomising patients 1 : 1 to either the experimental intervention versus usual care. Thus, neither investigators nor patients or relatives can influence to which group the patients are allocated. The patients will be stratified according to sex and the treating heart centre. For both groups, the follow-up assessment will take place at 1 month (T1), 4 months (T4), 6 months (T6) and 12 months (T12) postdischarge and a register-based follow-up assessment will be conducted at 24 months (T24; see figure 2). In the event of complications arising after study enrolment, cases will be handled individually (see Intervention deviation section).
{kind=link}
{kind=link}
Patient flow.
The patients answer questionnaires independently of the researchers, and before randomisation. All questionnaires are distributed electronically, thus data management is handled independently from the researchers who interpret data. All data entry is doubled and stored electronically in a coded database, and in an independent spread sheet, only accessible for the CopenHeart group.
Personal information about potential and enrolled patients will be collected electronically and shared in a database only accessible to those within the project group responsible for patient recruitment, to protect confidentiality before, during and after the trial.
Experimental intervention group
Patients in the intervention group will follow the integrated rehabilitation programme, consisting of a psychoeducational component and an exercise training component as well as usual care (see below). The intervention has been developed and tested in two clinical trials; the DANREHAB trial including patients with ischaemic heart disease and HF,39 and the COPE-ICD trial including patients with an implantable cardioverter defibrillator.26 The blood work and clinical control described for the control group (see below) are incorporated in the follow-up of the intervention group.
Psychoeducational component
The aim of the psychoeducational intervention is to provide emotional support and improve coping skills and illness appraisal in order for the patient to respond appropriately to physical and psychological symptoms. Education and information about the disease prepare the patient for expected symptoms and sensations. Dialogue and shared reflection facilitate strategies for coping with symptoms and experiences associated with the condition, for example, anxiety and fear. Cardiac care nurses with specific training will perform the psychoeducational intervention. Some of the most commonly reported concerns of patients treated for IE, such as fatigue, gastrointestinal function and concerns about work life are outlined in an inspiration guide for the nurses to address when and if relevant (see table 1). Information given will also be based on national guidelines and standard treatment of patients with IE, and on the findings of the qualitative study on postdischarge experiences described in the complementary studies section of this paper. The consultations focus on managing life after IE by establishing a joint approach to disease management and coping strategies, using a holistic view. The psychoeducational intervention is inspired by RR Parse's Human Becoming Practice Methodologies Three Dimensions.40 These are interpreted as (1) discuss and give meaning to the past, present and future, (2) explore and discuss events and possibilities and (3) move along with envisioned possibilities. According to this theory, there are three ways of changing health: creative imaging, that is to see, hear and feel what a situation might be like if lived in a different way, affirming personal patterns and value priorities and shedding light on paradoxes, that is, looking at the incongruence in a situation and changing the view held of something. The nurse is truly present in the process through discussions, silent immersion and reflection. The human becoming practise methodology was chosen to apply a holistic patient approach, focusing on the coping and transformation process of the individual person. Furthermore, the method is extensively used in the outpatient heart clinics at the heart centre at Rigshospitalet, such as for patients with inherited heart diseases and adults with congenital heart disease and finally documented in the COPE-ICD trial.26 ,41 The consultations take place in a quiet setting at the outpatient clinic and will last for approximately 1 h. The nurse is able to facilitate contact with or seek advice from a physician if needed. The first consultation will be approximately 1 week after discharge, and then once every 4–6 weeks, with a total of five consultations. Consultations can be done by telephone, according to the patient's wishes. The primary investigator will attend the consultations regularly to ensure protocol compliance.
Inspiration guide for nursing consultations/psychoeducational intervention
Physical exercise training component
The main objective of the exercise training is to improve the patient's physical capacity and facilitate lifestyle/behavioural changes, which will subsequently result in physical and psychological health benefits for the patient. However, the exercise training programme is also targeted at relieving the fear and uncertainty that the patient may feel in relation to physical activity. The intervention is based on the European guidelines for physical training in cardiac rehabilitation16 and complies with the recommendations on physical activity of the Danish National Board of Health.42 The intervention consists of three components (1) individual planning of the exercise training, (2) 12 weeks of high-intensity exercise training and (3) continuous moderate daily physical exercise.
Individually planned physical exercise by a specialised cardiac rehabilitation physiotherapist
Integrating detailed information regarding the specific type of IE, comorbidities, hospitalisation, activities of daily living (ADL) and level of physical activity prior to IE, the physiotherapist conducts a patient consultation of up to 30 min. The consultation is based on the initial testing of the patient, including the cardiopulmonary exercise testing, described in the outcome measures section, a 6 min walk test and a ‘sit to stand’ test. For all patients an individual training diary is prepared, and all patients are instructed in the use of a HR monitor integrated into Polar watches, provided by Rigshospitalet. The HR monitor and diary is essential to ensure CopenHeart training protocol compliance and are returned for data collection at the end of the exercise training intervention.
Intensive exercise training programme
The initial training sessions take place in a physiotherapist-supervised setting at the primary investigating hospital, Rigshospitalet, to ensure the quality, intensity and safety of training. Training is started 4 weeks postdischarge to ensure optimum postsurgery healing after heart valve surgery or cardiac device implantation. Using wireless electrodes integrated into t-shirts (Corus-Fit, CardioCardio and Corus Exercise Assistant, CEA, vs 2.0.16, Finland) potential cardiac arrhythmias, electrocardiographic abnormalities such as ST-depression, ST-elevation, Q-wave or T-wave altering, atrial fibrillation and ventricular arrhythmias and training intensity level are monitored. After 1–3 exercise training sessions at Rigshospitalet, the patient continues the programme at a local CopenHeart certified training facility supervised by physiotherapists or as supervised home-based training. Supervised home-based exercise training has shown similar results as hospital-based exercise training,43 and has been confirmed in a Danish setting.44
The physical exercise training continues for 12 weeks, comprising 3 sessions weekly of 60 min, with a total of 36 sessions. The training protocol consists of aerobic and anaerobic exercise to accommodate endurance and muscle strength.
An exercise training session consists of 10 min warm up, 20 min of bicycling, 20 min of resistance training and 10 min stretching and cool-down period. Using the results from the cardiopulmonary exercise test performed prior to the initial training session, in combination with the Borg scale measuring subjective exhaustion, the aerobic exercise is performed with a gradually increasing intensity throughout the exercise intervention period, corresponding to 13–17 at the Borg Scale and 50–80% of the maximum HR. The anaerobic resistance training is initiated at 30–40% of one repetition maximum (RM) for the upper body, and 40–50% of one RM for the lower body, with an increasing work load during the training sessions. To achieve cardiovascular adjustment and reduce the risk of malignant cardiac arrhythmias and ischaemia, the training session is initiated and terminated with a warm-up and a cool-down period to gradually increase and decrease training intensity and HR. This cardiovascular adjustment has been proven to reduce the risk of ischaemia and arrhythmia in relation to exercise training.45 ,46 Training is predominantly performed in the upright position to reduce left ventricle preload (diastolic volume) and the risk of ischaemia and arrhythmias due to HF.46
Sustained moderate daily physical exercise
Participants are instructed to perform moderate physical exercise at least 30 min/day during the intervention period, for example, bicycling, walking, gardening, jogging or recreational sports. Daily moderate physical exercise is encouraged to be continued throughout life.
Intervention deviations
Both components of the intervention will be supervised regularly by the primary investigator to ensure protocol compliance. Modification of the allocated intervention due to surgery complications, rehospitalisation or emerging comorbidities (eg, pneumonia, pericardial exudation and musculoskeletal problems) will be individually assessed, and the time of the primary outcome assessment at 4 months (described in section below) will be corrected in accordance with changes in the intervention.
Usual care control group
Patients in the control group will follow standard follow-up for patients treated for IE, with one to two visits within the first month postdischarge, including blood work and clinical assessment. Haemoglobin level, infection variables, kidney function and, on indication, liver status is assessed, and blood cultures are drawn on suspicion of IE relapse. Blood pressure, pulse and temperature parameters are obtained. If results give cause for concern, the patient will see a specialist physician during the follow-up visit. A transthoracic echocardiogram will be performed within the first year postdischarge, typically between 1 and 6 months postdischarge and again at 12 months, depending on whether the individual patient has had heart valve surgery and on the status of the native or replaced valve. These patients will be contacted at 1, 4, 6, 12 and 24 months for outcome assessment, including functional test, questionnaires and clinical data collection (see figure 2).
Outcomes and data collection
Numerous data will be collected to evaluate the effect and meaning of the intervention. The primary and the secondary outcome reflect the primary modifiable factors of the intervention. Since almost no evidence exists, a number of explorative outcomes will also be collected.
Primary outcome
MH will be measured by the Mental Component Subscale (MCS) of the Medical Outcome Study Short Form 36 (SF-36) questionnaire47 after 1 month (T1), 4 months (T4), 6 months (T6), 12 months (T12) and 24 months (T24). The SF-36 questionnaire is a measure of self-rated health. It is a validated multipurpose health survey comprised of 36 items that address the following eight dimensions: physical functioning (PF), role physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role emotional (RE) and MH. The first four scales (PF, RP, BP and GH) are then combined into a physical component scale and the latter four (VT, SF, RE and MH) into an MSC.47 The instrument was chosen for its ability to detect changes in self-rated health within domains that could potentially be influenced by the CopenHeartIE intervention. MH was chosen as the primary outcome as other studies have shown that MH is affected in patients with IE compared to healthy controls13 ,14 and the rehabilitation intervention focuses on this modifiable factor.
Secondary outcome
Physical capacity will be measured by peak VO2 using cardiopulmonary exercise testing (Ergo-Spiro CS-200, Schiller, Switzerland) by investigators blinded to the intervention group. The test will be performed according to current guidelines for ergospirometry testing,48–50 using an ergometer bicycle with spirometry, monitoring heart rhythm, blood pressure, ECG and measuring gas exchange during workload and in the following recovery period. Average test duration is 10–15 min including pretestand post-test phase without work load. Before each session, calibration will be performed to address changes in room temperature, humidity and air O2 content. A standardised ramp protocol will be used with an initial work load of 25 or 50 W, increasing gradually by 12.5 W/min until peak exhaustion. Peak exhaustion is evaluated by a respiratory exchange ratio (RER)≥1.10 or subjective exhaustion of the patient. To encourage patients equally, independent of the tester, a standardised guide has been developed. During the test, clinical manifestations, ECG abnormalities (ST depression, ST elevation, q-wave and t-wave changes, supraventricular or ventricular arrhythmias), blood pressure response and several physiological parameters will be observed and documented. The test will be performed by either a cardiac care nurse or a physician. For safety reasons, preset criteria for initiation and/or termination of the test have been defined. The test will be performed prior to the exercise training programme (T1), after 12 weeks of exercise training (T4) and at 12 months follow-up (T12). Physical capacity was chosen as the secondary outcome measure, as studies indicate that patients treated for IE are physically deconditioned after long-term illness and hospitalisation.14
Exploratory outcomes
A more extensive evaluation of the physical and psychological status of the patients over time will be performed, exploring demographic, clinical, paraclinical and imaging variables, as well as additional physical capacity tests and additional questionnaires exploring, for example, fatigue, sleep quality and anxiety and depression (see table 2).
CopenHeartIE—exploratory quantities subjected to post hoc analysis
Data collected from official national registers regarding mortality, hospitalisation, emergency room visits, outpatient visits, medication, employment status and payment of welfare benefits (sick leave payment and early retirement pension) will be collected at 24 months to assess the long-term effects of the intervention. The Danish official national registers are well functioning with a small percentage of lost data.64 Consequently, the method is well suited as an outcome measure in small patient populations. Data will be collected from the Danish National Patient Register,65 the Danish National Health Service Register,66 the Danish National Prescription Registry,67 the Danish National Causes of Death Register68 and registers on transfer payments and labour market affiliation.69 ,70
Economic evaluation
An economic evaluation will be conducted alongside the trial to assess the cost utility of comprehensive cardiac rehabilitation compared with usual care in the study population. The economic evaluation will compare the costs to QALYs (quality-adjusted life years) and take a societal perspective as recommended nationally. QALYs and costs will be assessed at the end of the intervention, 6 months from randomisation and later after 24 months from randomisation using register-based follow-up.
QALYs will be estimated using the self-completed EQ-5D instrument, which is a standardised instrument assessing five dimensions of self-reported health status (mobility, self-care, usual activities, pain/discomfort and anxiety/depression).71 ,72 The estimated calculations will be evaluated using Danish preference weights.73 Information on costs will only include costs that are expected to differ between the intervention and usual care group.59 Included costs in the evaluation are health costs associated with the rehabilitation programme, other healthcare costs (healthcare utilisation apart from rehabilitation), patient costs and costs of productivity losses. Information on costs will be collected by a mixture of activity-based costing, surveys, patient diaries and by the use of registers.
Results from the analysis will be reported as an incremental cost-effectiveness analysis (ICER). Sensitivity analysis will be conducted to express uncertainty in the estimates.74 The reporting of ICER is presented using Bayesian methods, including bootstrapping and presented as cost-effectiveness acceptability curves.75
Sample size, power calculations and interim analysis
We will perform a randomised trial with a continuous response variable from independent control and intervention group participants with one control per intervention group participant. A previous study on an IE population found that the MSC was normally distributed with a SD of 13.13 If the true difference between the intervention and control group means is six points, we will need to include 75 participants in each study group (a total of 150 participants) to be able to reject the null hypothesis, stating that the mean in the intervention and the control groups are the same with a power of 80%. The type I error probability associated with this test of this null hypothesis is 5%.
For the secondary outcome, VO2, we will be able to reject the null hypothesis that the population means of the experimental and control groups are equal with a probability (power) of 75.4%, assuming the VO2 is normally distributed with an SD of 6.9,27 ,28 and the true difference in the experimental and control means is 3 ml/kg/min.
A data monitoring and safety committee will be informed, every 9 months, of all serious adverse events occurring in the two study groups. An interim analysis meeting will be held by the data monitoring and safety committee to review data relating to intervention efficacy, participant safety and quality of trial conduct. The committee will evaluate data on the primary and secondary outcome measures; MH (SF-36)/peak VO2 (efficacy) and all serious adverse events (safety/tolerability). After the interim analysis meeting, the committee will make a recommendation to the steering committee whether to continue, hold or terminate the trial. This recommendation will be based primarily on safety and efficacy considerations and will be guided by statistical monitoring guidelines defined by the trial safety charter.
Statistical analysis
Data will be pseudoanonymised and analysed, blinded by a trial-independent statistician using intention-to-treat analyses and a mixed model with repeated measures (MMRM) for continuous outcome measures.76 Using MMRM ensures that missing data values (in the case of the primary and secondary outcome) will not create bias as long as the missing values are random. Two-sided tests will be performed. The level of significance is set at 5%. Dealing with multiplicity, gate keeping will be used to adjust the observed p values for primary and secondary outcomes.77 Both original and adjusted p values will be reported.
For the primary and secondary outcomes, we will conduct sensitivity analysis to assess the potential impact of non-random missing values. For each intervention group (A and B) some quantities (imputing quantities) will be computed to be used to impute missing values in a group (A or B) as explained below. A comparison between groups A and B where missing values in group A are imputed using imputing quantities obtained from group A and missing values from group B are imputed using imputing quantities obtained from group B is referred to as a best-case analysis. If missing values in group A are imputed using imputing quantities obtained from group B and vice versa the comparison is called a worst-case analysis. The imputed quantities for the primary outcome would be the group mean at T1 (X1-bar), the group mean at T4 (X4-bar), the group mean at T6 (X6-bar), the mean difference between the value measured at T4 and that measured at T1 (delta 1), and the mean difference between the value measured at T6 and that measured at T4 (delta-2). Table 3 explains how the quantities will be used to impute missing values in a group (either the same group or the other intervention group).
Statistical appendix
If the SE of a parameter estimate calculated using imputed data is smaller than that of the corresponding parameter calculated using complete case data it will be replaced by the latter SE when the p value is calculated.
Long-term register-based outcomes will be analysed by two different models: non-negative count outcomes (eg, number of contacts to the hospital or number of visits to general practitioners) will be analysed by a Poisson model or a zero-inflated Poisson model if the number of zeros are large, and time-to-event data (eg, cause-specific mortality and leaving the labour market) will be analysed with survival methods (Kaplan-Meier estimator and Cox regression model). Especially for socio-economic outcomes, competing risk due to mortality will be considered if a large proportion of patients die during follow-up.
Explorative data will be analysed using appropriate statistical methods according to type of data (see table 2). SPSS V.19.0 and SAS V.9.3 will be used.
Complementary studies
Qualitative study on postdischarge experiences
The postdischarge experiences of patients treated for IE will be explored through semistructured qualitative interviews, which take a phenomenological−hermeneutic approach. The data derived from this study will be used to address relevant issues designing the rehabilitation intervention. The patients treated for IE, 3–6 months postdischarge will be identified through hospital admission lists. A sample sufficient to achieve data saturation will be included. The study aims to answer the following thematic research questions: What are the experiences of returning home after treatment for IE? What are the new experiences, if any, in daily living? Which health problems, if any, have patients experienced? What are the concerns, if any, for the future? The data analysis is inspired by Ricoeur's theory of interpretation and consists of three levels: naive reading, structured analysis and critical interpretation and discussion. Qualified interviewees will be chosen, ensuring a representative sample in relation to sex, age and surgery/non-surgery.
Survey-based study
The postdischarge status of the patients treated for IE will be explored through a national survey. The standardised questionnaires SF-36,47 ,78–81 Hospital Anxiety and Depression Scale (HADS),54 Multidimensional Fatigue Inventory (MFI-20),61 ,82 EuroQoL—EQ-5D,59 ,83 Heart-Related Quality of Life (HeartQoL R),58 International Physical Activity Questionnaire (IPAQ)60 ,84 and a questionnaire developed by the Danish Heart Foundation on the extent and quality of rehabilitation offered will be sent out to patients who have undergone treatment for IE, 6–12 months postdischarge. The instruments are all validated and have good reliability and responsiveness.54 ,58 ,60 ,61 ,83 ,85 The data will provide knowledge on patients’ self-rated health, quality of life, fatigue, anxiety and depression, body image and extent and quality of the rehabilitation currently received. The patients will be identified through the National Patient Register65 and questionnaires will be sent out to 210 of them. We aim to achieve a response rate of 70%, using repeat mailing strategies and/or telephone reminders to maximise response if necessary.86 This should result in an estimated 150 questionnaire respondents. Data will be anonymised and analysed by relevant descriptive statistical methods.
Qualitative study on rehabilitation participation experiences
After the intervention, an interview study, including 10% of the intervention population or until data saturation has been reached, will be conducted, to explore the experiences and processes behind the potential effect of the intervention. The study aims to answer the following thematic research questions: What are the experiences of participating in the integrated rehabilitation programme? Which components of the programme are meaningful? In what way? Participant selection and applied methods in this study are consistent with that of the qualitative study on postdischarge experiences.
Ethics
The trial has been approved by the Regional Research Ethics Committee (no H-1-2011-129) and the Danish Data Protection Agency (no 2007-58-0015). All eligible patients will be informed about the trial verbally and in writing, and the patients are included after written informed consent is obtained. All data will be handled confidentially and patients are ensured anonymity. The study complies with the latest Declaration of Helsinki and is registered at ClinicalTrials.gov (NCT01512615). An independent safety committee comprised of an international group of experts is monitoring the trial; ensuring good clinical practise standards are being upheld. No serious risks are anticipated to receiving rehabilitation. No risks have previously been reported in relation to psycho-educational consultations. The physical exercise training and the cardiopulmonary exercise testing will be supervised by competent healthcare professionals and will be in accordance with current guidelines on safety when testing and training cardiac patients.87 ,88 Efforts will be made to avoid arrhythmias during workload testing and exercise training by protocol with a cool-down period, which positively affects serious complications. Staff members will be trained according to guidelines to handle cardiac arrest or other disease-specific or device-specific emergencies. All serious and moderate adverse events will be registered and reported according to the protocol.
Not providing rehabilitation to the control group can be ethically justified, as current national and international guidelines give no specific recommendations on cardiac rehabilitation for patients treated for IE. The scope and quality of rehabilitation offered to this population is unknown, but suspicions are, that often no or suboptimal rehabilitation is provided. The survey-based complementary study, described previously in this paper, will hopefully provide more insight. In screening patients for participation, the enrolling nurse or physician will exclude patients with a compelling rehabilitation need, for instance after a cerebral embolic event. Furthermore, patients are informed of the study design before giving their consent, and are free to decline participation.
Discussion
This randomised clinical trial is the first to examine PF by cardiopulmonary exercise testing and to test a comprehensive rehabilitation programme on a large heterogeneous population of patients treated for IE. CopenHeartIE will provide much-needed evidence and insight on the postdischarge status and rehabilitation needs of patients treated for IE for healthcare professionals and policymakers to make qualified, evidence-based decisions in everyday clinical practise and as a foundation for national and international guidelines. With increased physical and psychological well-being of patients, lower morbidity and healthcare utilisation expected in case of a positive outcome, patients and society are anticipated to benefit greatly. Whether it produces neutral, negative or positive results, the CopenHeartIE trial will have implications for clinical practise in follow-up care of patients treated for IE in the western world.
The patients may decline participation due to an unwillingness to return to hospital after a lengthy illness and hospitalisation. We will attempt to avoid this problem by informing patients of the potential benefits of participation, for example, the security we provide by following them closely after postdischarge and the value to science of their participation for future patients. Furthermore, it is documented that a substantial number of patients in rehabilitation studies control group perform self-initiated physical exercise training, possibly motivated by the study information during the recruitment process.39 Hence, we will abstain from giving extensive information about the training programme, or elaborate on the health benefits of physical training before knowing to which group the patient is randomised.
The study has been designed to meet the criteria for high quality in non-pharmacological randomised clinical trials89 with central randomisation, multicentre participation, blinded assessment of the exercise outcome, blinded analysis by study independent statisticians and furthermore, detailed information on the intervention received and usual care will be collected, including information on self-initiated exercise training during the trial period. For the primary outcome, the mental-health component subscale, we are aware of the subjective nature of the data collected. Accordingly, we will interpret the findings conservatively.
Safety aspects and Data Monitoring Safety Committee
In supervised exercise training and testing of other cardiac patient groups than patients after IE, the risk of adverse effects is low (eg, ischaemic heart disease, chronic HF); however, no current national safety instructions exist. Patient safety is given highest priority, and exercise training after heart valve surgery is considered safe based on results from exercise testing and training with HF patients.87 ,88 Any serious adverse events will be registered as part of the data collection.
The Data Monitoring Safety Committee (DMSC) works independently from the funder and has no competing interests, and consists of two clinicians and a statistician. The committee is responsible for safeguarding the interests of trial participants, assessing the safety and efficacy of the interventions during the trial, and for monitoring the overall conduct of the clinical trial. The steering committee and the DMSC communicate regularly and at least every 9 months the overall number of all serious adverse events is reported.
Dissemination plan
The results of the trial and complementary studies will be published in relevant international peer-reviewed journals. Authorship will be determined according to the guidelines of the International Committee of Medical Journal Editors. Owing to the comprehensiveness of the outcome measures the results will be presented in more than one scientific paper as relevant. Economic and long-term follow-up will be reported as data become accessible.
Trajectory
Inclusion was initiated in December 2011 and is expected to be completed at the end of 2013. Results from two of the complementary studies are expected during 2012, and from the clinical trial in 2014. To achieve adequate participant enrolment, patients are recruited from two independent heart centres, and another heart centre, already in partnership of the trial, will be invited for inclusion if the enrolment rate declines. The inclusion rate is carefully monitored weekly. The patients in doubt are contacted several times during hospitalisation, and if necessary after hospital discharge by phone.
Acknowledgments
The team responsible for the rehabilitation intervention and study administration is: Pernille Preisler, Anna-Louise Boehm-Baggesen, Helena Tjalk-Sørensen, Lars Tang, Signe Gils, Helle Tauby, Katrine Haase and Line Ellemann-Jensen.
References
Footnotes
-
Contributors SKB, ADZ, TBR, HB, CG and JLH, in collaboration with PM and TMN, designed the study and developed the protocol. PW and LCT specifically designed the statistical analysis plan. TBR, SKB, ADZ, SSR and KLS drafted the manuscript. SKB, ADZ, HB, CG, JLH, PW, LCT, PM, TMN, SSR and KLS all revised the manuscript critically. All authors have given their final approval of the version to be published.
-
Funding The trial is partly funded by Gentofte Hospital, Rigshospitalet, and the Danish Council for Strategic Research. The funder has no influence on the study design, the execution of the trial or the interpretation of data.
-
Competing interests None.
-
Ethics approval Regional Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.