Article Text

Abstract
Objectives The authors investigated self-perceived psychosomatic health in young people (10–24 years of age) in Sweden and analysed different samples during the years 2005 and 2007–2010 via a community website.
Design Repeated cross-sectional surveys: (1) single question on a single day in 2005. (2) One specific question delivered on each of eight separate days in 2005. (3) The same eight questions delivered to smaller groups on the same day in 2007 and then again to randomly selected subjects in 2010.
Setting Validated questionnaires launched on the internet by a recognised Swedish community site. Study participants were invited to answer questions about their health with full anonymity as they logged into their personal area.
Participants 10–24-year-old children, adolescents and young adults.
Primary and secondary outcome measures Self-reported psychosomatic health in terms of sex and age over time.
Results A large number of responses were obtained (up to 140 000). The response rate for the single item on stress was 41%. A high percentage of young subjects responded that they felt stressed very often/often; the numbers were higher for women (47%) than for men (29%). Older teenaged women had more psychosomatic complaints than did men of similar ages; in contrast, among 10–12-year-old children, the percentage of psychosomatic complaints was similar for men and women. When comparing results obtained in 2010 with those obtained in 2007, young people of both sexes had a slightly better self-perceived health status in 2007.
Conclusions During the period 2005–2010 a high percentage of young people, particularly females, 16–18 years of age, had psychosomatic complaints and considered themselves as being often or very often stressed. These complaints were more pronounced in the older age groups. When directing questions to a large community, internet-based surveys appear to be valuable tools.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Examining self-perceived health and stress in large cohorts of children, adolescents and young adults who are members of a large Swedish web-based community.
Examining whether psychosomatic health deteriorated in adolescents between 2007 and 2010.
Assessment of the usability of a large web-based community on the internet to investigate self-perceived psychosomatic health in Swedish youth.
Key messages
A high percentage of young subjects responded that they felt stressed very often/often, and the numbers were higher for women than for men.
Older teenaged women had more psychosomatic complaints than men did.
Both sexes reported a slightly worse self-perceived health status in 2010 than in 2007.
Novel internet-based community site surveys are feasible for assessing self-perceived health in the young.
Strengths and limitations of this study
The study examined a very large cohort of children, adolescents and young adults from throughout Sweden.
All subjects responded completely voluntarily.
There may be a selection bias, given that we do not know the psychosomatic health of individuals who were not logged onto the website.
Participation in the survey was completely anonymous; thus, we could not perform additional interviews to study the web questions' validity in this population.
Introduction
Children's life situations have changed dramatically over the past decades. Several conditions in today's modern information-based society have exposed children to seemingly increased levels of stress in multiple ways.1 ,2 Lupien et al3 noted that risk factors for the development of stress reactions depend primarily on an individual's genetic vulnerability, exposure to adverse life events, socioeconomic situation, disturbances in important relationships, problems with school and the timing of stressful events. Importantly, the development of stress reactions in young people is, to a great extent, gender dependent.4–6 Thus, it seems plausible that several factors, both psychological and physical, play important roles in the development of stress reactions which will have an impact on children's well-being and ill health, with salient implications for future health and disease.7
High frequencies of ill health, such as complaints about perceived stress and psychosomatic symptoms in children, adolescents and young adults, particularly older teenage girls, have recently been reported in Sweden and internationally.8–13 The aim of this study was to obtain information both at a given time point and as a analysis at different time points about perceived stress and psychosomatic symptoms in Swedish subjects aged 10–24 years. To achieve this purpose, we needed a strategy that would feasibly allow us to ascertain a large number of respondents. Donker et al14 used screening questionnaires for common mental disorders and recommended that such questionnaires be administered via the internet, which offers quick and easy access to a large number of users at a low cost. The screening must be brief, as subjects are more likely to undergo screening if it is short, quickly completed and easy to read.14
Our primary and main aim was to explore psychosomatic health problems among children and adolescents, focusing on sex and age differences, using a web-based protocol launched on a large internet community.
To our knowledge, this study is the first to use the internet to examine self-perceived health and stress in large cohorts of children, adolescents and young adults. Furthermore, as a secondary objective, we explored possible changes in the percentages of self-reported health complaints over a 3-year period from 2007 to 2010.
Methods
The present study used the internet to assess psychosomatic health in young people using well-established questions,4 ,10 ,11 with the beneficial result of having a high number of respondents in each age and sex category. Each subject could log into her or his own ‘LunarStorm corner' and voluntarily choose to complete the questions on the community site, which would make the subjects more likely to provide honest answers. Compared with the response rates obtained from telephone or mail questionnaires, the number of responders per day may seem somewhat low. We received responses from 100 000 to 150 000 individuals per day, which represents approximately 36% of the entire population of members (1.2 million).
Data were collected via internet-based questionnaires consisting of three parts: (1) a single question about ‘stress,’ launched on the internet on a single day in January 2005. (2) Eight questions about subjective health that were completed between 26 May and 28 June 2005. One question was delivered on each of eight separate days. (3) The same eight questions (comprising a composite measure of subjective health), delivered to smaller groups of randomly selected 15–20-year-olds on the same day in May 2007 and then again to a new age-matched group of randomly selected adolescents and young adults in May 2010. The subjects had complete freedom regarding whether to complete or abstain the questionnaire.
Apart from the single question about stress, the aforementioned eight questions were developed and tested for reliability and used by the Swedish National Board of Health and Welfare (http://www.socialstyrelsen.se) in studies of the psychological health and well-being of children and adolescents. The composite measure of subjective health4 comprised the following items: difficulty concentrating, difficulty sleeping, suffers from headaches, suffers from stomach-aches, feels tense, poor appetite, feels low and feels dizzy. The response categories for all of these items, which were delivered in question form, were ‘don't know’; ‘no, never’; ‘no, seldom’; ‘yes, sometimes’; ‘yes, often’ and ‘yes, always’. The outcomes from psychometric Rasch analysis of the psychosomatic problems (PSP) scale have been reported in previous papers.15 ,16 The analysis confirmed the appropriateness of considering somatic and psychological problems as interacting parts that constitute a higher-order unidimensional construct (psychosomatic health). The scale showed valid psychometric properties and met the measurement requirements of invariance and proper item categorisation. The Rasch model further revealed that from a general level of analysis, the eight items were invariant among students with good health and among those with bad health. Importantly, these eight questions also work invariantly across time; that is, there is no differential item functioning with respect to the year of investigation, which is a prerequisite for repeated analysis, as in the present study.
The item about stress was ‘How often/seldom do you feel stressed?’, and the response categories were ‘yes, very often’; ‘yes, often’; ‘yes, sometimes’; ‘no, seldom’; ‘no, very seldom’; ‘no, never’ and ‘don't know’.
Initially, we placed one question per day on LunarStorm's website, which was one of the first web communities to be established in Sweden. At the time of our investigations in 2005 and 2007, LunarStorm was the largest internet community in Sweden. It had 1.3 million active members and approximately 360 000 unique visitors per day who spent approximately 40 min per visit on the site (TNS Gallup/Red Measure, Nielsen/Net Ratings). Eighty-three per cent of 15–20-year-olds in Sweden were LunarStorm members, and 25 of 30 pupils in every secondary school class were members (Lunarworks AB/SCB). The gender distribution of members was 53% women.
Members saw the question after login, and only one answer per login was allowed and counted. We focused on children, adolescents and young adults from 10 to 24 years old. The percentage of LunarStorm members in each age class in Sweden ranged from 20% to 88%, with the highest values (>80%) for adolescents between 13 and 16 years of age (Statistics Sweden, http://www.scb.se). The reason why we placed one question per day instead of presenting the whole eight-item questionnaires at one single occasion was that the web community administrator had the experience that using such long composite questionnaires decreased the participation rate substantially. However, after receiving high response rates on the separate items, we decided to include the whole eight-item questionnaire at one specific time point.
The first set of eight questions was released on the internet on a single day in 2007 to a group of 15–20-year-old subjects who were randomly selected by the community websites using statistical methods. Children and younger adolescents were not included as they were in the protocol that presented one question per day. We chose to focus on 15–20-year-olds because of their higher response rate. Because questions released on separate days would attract a very large number of responders, we were able to divide the subjects into gender groups and into various age groups (online table 1). In yet another internet-based protocol using the same eight questions described above to determine self-perceived health trends, the subjects were randomly selected in both May 2007 and in May 2010 to respond to the questions. These groups comprised approximately 1500 subjects aged 15–20 years (online table 2).
Ethical approval was obtained from the chairman of the review board. According to the ethical guidelines, posting questionnaires on the internet does not require ethical approval from a committee. However, we choose to discuss these issues thoroughly with the chairman and received full approval.
Statistical analyses
The Mann–Whitney U test and the Kruskal–Wallis and χ2 tests were used. Each of the possible responses to each of the eight questions in the Likert format was assigned a number (‘no, never=1’; ‘no, seldom=2’; ‘yes, sometimes=3’; ‘yes, often=4’ and ‘yes, always=5’), which was multiplied by the response frequency and then averaged. The same procedure was performed with the item about stress, and the response categories were ‘yes, very often=6’; ‘yes, often=5’; ‘yes, sometimes=4’; ‘no, seldom=3’; ‘no, very seldom=2’; ‘no, never=1’; the answer ‘don't know’ was not included in the statistical calculations. Statistical significance was considered when p<0.05.
Results
Consistently more girls answered the questions, and there was an age-group-related decline in the severity of self-perceived health; however, girls still reported higher frequencies of psychological ill health during the whole investigated age span. The peak of problems experienced occurred in adolescents aged 16–18 years, and females perceived the most problems.
Item about stress
The single question about stress received 148 395 responses (85 330 girls) from 10- to 24-year-olds. The vast majority of this population was between 10 and 24 years old. When analysing the total population, we found that 30% of the women and 19% of the men considered themselves stressed very often (figure 1). Similarly, the response ‘yes, often’ was provided more often by women: 17% versus 10% in men (p<0.0001). When the 10–24-year-old population was divided into age subgroups, we found that 16–18-year-old males and females reported the highest degree of stress (very often): 22% for men and 37% for women (figure 2, p<0.0001). The lowest number of subjects responding ‘yes, often’ to stress was in the 10–12-year-old group. Consistently, females were significantly more likely to report higher levels of stress (‘very often’ and ‘often’) than males from 10 to 24 years of age. The percentage of males responding ‘yes, very often’ to the stress question remained relatively constant at 20% from 13 to 24 years of age, while the percentage of females responding ‘yes, very often’ increased until they reached 16–18 years old and levelled off for those who were 19–24 years old. However, this older female group still showed statistically significantly higher values for self-perceived stress than males of the same age (figure 2). Men of all ages chose the alternative response ‘no, never’ to the question about stress statistically more frequently than women (figure 2).
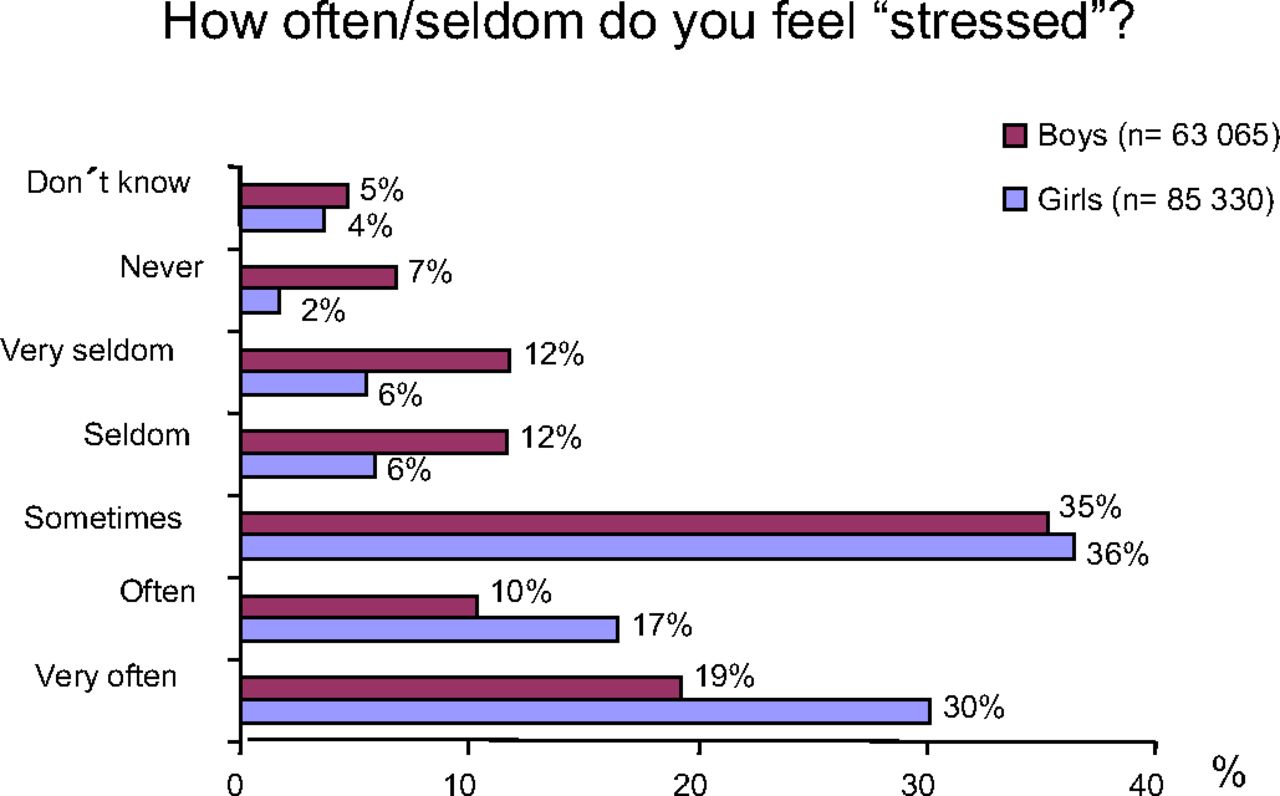
Bars depict the percentage of ‘never’ to ‘very often’ responses to the question ‘How often/seldom do you feel stressed?’ for 10–24-year-old females and males. The total number of respondents was 148 395. For the statistics, see the text.

{kind=link}
{kind=link}
Bars demonstrate the percentage of ‘never’ and ‘very often’ responses to the question ‘How often/seldom do you feel stressed?’ divided by sex and age. The numbers in the graph represent the number of responding individuals. The statistics are reported in the text.
Eight questions presented via the internet on separate days to 10–24-year-olds
Given that these questions were placed one at a time, the response frequency varied between 12 000 and 45 000 subjects, who were mainly in the 10–12-year-old and 13–18-year-old age groups, respectively; the response frequencies for all eight questions were similar (online table 1). When all the possible responses to all eight questions were considered, we found that men of all age groups scored higher in terms of self-perceived health compared with women (p<0.0001). The only exceptions in which there were no differences between males and females occurred in the 10–12-year-old group regarding difficulty concentrating (p=0.11) and in the 19–24-year-old group regarding difficulty sleeping (p=0.16).
An analysis of the four age groups' responses to all the questions (except for the question regarding poor appetite) revealed that the older the subjects, the poorer their self-perceived health (p<0.0001). Both women and men demonstrated poorer self-perceived health the older they were (p<0.0001 for both, except for p=0.04 for poor appetite in women). However, men reported fewer headaches (p=0.02) and better appetite (p=0.003) with increasing age. When we adjusted for the differences in sex, we found poorer self-perceived health with increasing age (p<0.0001), with the exception of poor appetite (p=0.52), which received opposite overall responses for men and women, as described above. Similarly, when we adjusted for differences in age, we found better self-perceived health in men than in women (p<0.0001).
Eight questions regarding self-perceived health presented together on the internet in 2007 and 2010
Men reported better self-perceived health than women for all eight questions in the 2007 questionnaire (p<0.0001). The results were similar in 2010, with men reporting better self-perceived health than women regarding headache, stomach-ache, feeling tense, poor appetite, feeling low and feeling dizzy (p<0.0001) as well as difficulty sleeping (p=0.002). The difference between men and women regarding difficulty concentrating was not statistically significant (p=0.06). There were subtle differences between the overall responses to the 2007 and 2010 questionnaires. Men demonstrated better self-perceived health in 2007 versus 2010 regarding feeling low, poor appetite, feeling tense, and difficulty sleeping and concentrating (online table 2). Women presented a similar pattern of better self-perceived health, with the exception of poor appetite (no change). The items stomach-ache, headache and feeling dizzy remained unchanged from 2007 to 2010 for both sexes (online table 2).
Discussion
We found marked differences between the sexes regarding psychosomatic symptoms, with females reporting higher degrees of stress compared with males across the large age span between 10 and 24 years of age. These symptoms appeared to be most pronounced between 16 and 18 years of age and then declined, supporting and extending the results of Hagquist.4 Similar findings using the same eight questionnaire items were reported previously4 ,10; however, these findings came from smaller regional studies that administered the questionnaires in person (by distributing them in schools). The present study used the internet to assess psychosomatic health in young people using well-established questions,4 ,10 ,11 with a high number of respondents in each age and sex category. The fact that each subject could voluntarily and anonymously choose to complete the questions on the community site could have made the subjects more prone to provide honest answers.
As shown in the present study and what has been noted previously4 ,11 is that women are more likely than men in the same age group to report feeling stressed across both childhood, adolescence and as young adults. Notably, while females seem to increase their reporting of stress and psychosomatic symptoms from childhood to young adults, similar variables are remarkably constant from 13 to 24 years of age in males. These salient sex differences may be explained by the fact that there are real differences in stress levels and psychosomatic symptoms between the sexes or that girls are more self-aware and reflecting and therefore more able to assess their psychological health or that it is more culturally acceptable for girls to report psychosomatic symptoms or a combination of the factors above. Boys might be more inclined to express themselves more physically, like being more active in sports or pursue other forms of acting out behaviour.10
For several, but not all, of the questions, self-perceived health was better in 2007 than in 2010 for both men and women perhaps reflecting the financial crisis that emerged in 2008. Although the changes between 2007 and 2010 were quite small, and the time elapsed was perhaps too short, we did note similar differences between men' and women' responses in 2005, 2007 and 2010. Self-perceived health was undoubtedly worse for women than for men, irrespective of age; this finding is supported by earlier studies5 ,6 and the results of Osika et al,12 who used Beck Youth Inventory questionnaires.
Our data, together with the results of previous studies,4 ,8 ,12 ,13 ,17 point unequivocally to impaired self-reported psychological and psychosomatic health in the young, and the prevailing situation and trend do not seem to be improving. The psychosomatic health of young women is of particular concern, given the increase in complaints that appears to have occurred over the past 20 years, as indicated by surveys in Sweden.4 However, the figures regarding alcohol problems, criminality and suicide are much higher for males than for females in the 16–24-year-old group.10
Given that the majority of the subjects in the present study were school-aged, the school environment is an important factor to consider. Previous reports established links between the school environment and the psychological and psychosomatic symptoms of school children.9 ,18 In fact, Hjern et al13 demonstrated an association between school stressors, such as harassment by peers, schoolwork pressure and being treated poorly by teachers, as well as psychosomatic pain and psychological problems, reflected as sadness, irritability, and feeling unsafe and nervous. In the light of our demonstrated sex differences also during school age, one may surmise that factors related to school environment might affect girls and boys differently.
Methodological considerations and limitations
The eight-item scale we used was validated in several studies as an appropriate means of estimating the subjective health complaints of children and adolescents. The instrument was also examined with the Rasch model, for which invariance is essential.16 ,19 There are few data available regarding internet-based surveys of psychological health among young people; thus, there are few validation analyses. Donker et al14 validated a brief web-based screening questionnaire for common mental disorders with follow-up phone interviews, using a ‘gold standard’ interview guide to assess the presence of DSM-IV disorders in the previous 6 months. Their questionnaire screened for common mental disorders. However, the subjects in the present study could not be identified; thus, such a validation was not possible.
A study by Mangunkusumu et al20 demonstrated good agreement between responses to questionnaires that were handed out manually and those administered via the internet. Notably, the internet approach received more favourable evaluations, even though it also took place in a school milieu. A major advantage of the present study was that the subjects could choose whether to answer the questions while in a familiar private and comfortable environment. Furthermore, such administrative factors as data transcription, the risk of excluded values and ‘odd’ answers and the concern that other people might read the answers can be overcome by computer- and internet-based surveys. Thus, internet surveys assessing psychological health and well-being issues appear to be quite suitable for use with young people.
Approximately 350 000 people logged in on a given day, raising the possibility of selection bias. Because the subjects were anonymous, we could not investigate selection effects. However, a recent study using the internet for health-related topics was independent of gender, age and diagnostic group in a group of patients with psychosomatic disorders.21 Although the design of that study was not entirely comparable with the present study, it is an indication of that there was limited selection bias in our study. Additionally, the response rate obtained at LunarStorm was very high for such a generalised internet-based survey.
Conclusions
A relatively high percentage of young people, particularly females 16–18 years of age, had psychosomatic complaints that did not seem to improve between 2007 and 2010. A considerable worsening of these complaints occurred from the age of 12 onwards in both sexes. Internet-based survey assessment appears a valuable tool for examining self-perceived health in young people over a broad range of ages.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
Footnotes
To cite: Friberg P, Hagquist C, Osika W. Self-perceived psychosomatic health in Swedish children, adolescents and young adults: an internet-based survey over time. BMJ Open 2012;2:e000681. doi:10.1136/bmjopen-2011-000681
Contributors PF had the main responsibility for designing, analysing data and shared the main responsibility for drafting the manuscript with WO. WO also took active part in designing questions regarding psychosocial health and reviewing data analysis. CH took active part in designing questions regarding psychosocial health, reviewing data analysis and made important commentaries on the text. Authors approve the present version to be published.
Funding This study was funded by Sahlgrenska Hospital, Stress Research Institute Stockholm University, Kempe-Carlgrenska Foundation, Public Health Committee of West Sweden.
Competing interests None.
Ethics approval Ethical approval was obtained from the chairman of the review board. According to the ethical guidelines, posting questionnaires on the internet does not require ethical approval from a committee. However, we choose to discuss these issues thoroughly with the chairman and received full approval.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional data available.