Article Text

Abstract
Objective Colorectal cancer screening by means of faecal immunochemical tests (FITs) requires successive screening rounds for an optimal preventive effect. However, data on the influence of the length of the screening interval on participation and diagnostic yield are lacking. Repeated FIT screening was therefore performed in a population-based trial comparing various repeat intervals.
Design 7501 Dutch individuals aged 50–74 years were randomly selected and invited for two 1-sample FIT screening rounds (haemoglobin (Hb) concentration ≥50 ng/ml, corresponding to 10 μg Hb/g faeces) with intervals of 1 (group I), 2 (group II) or 3 years (group III).
Results In group I, participation was 64.7% in the first screening round and 63.2% in the second. The corresponding percentages for groups II and III were 61.0% vs 62.5% and 62.0% vs 64.0%. Triennial screening resulted in a higher participation rate in the second screening round compared with annual screening (p=0.04). The overall positivity rate in the second screening round was significantly lower compared with the first round (6.0% vs 8.4%; OR 0.69, 95% CI 0.58 to 0.82) and did not depend on interval length (p=0.23). Similarly, the overall detection rate of advanced neoplasia was significantly lower in the second round compared with the first screening round (1.9% vs 3.3%; OR 0.57, 95% CI 0.43 to 0.76) and also did not depend on interval length (p=0.62). The positive predictive value of the FIT did not significantly change over time (41% vs 33%; p=0.07).
Conclusion The total number of advanced neoplasia found at repeat FIT screening is not influenced by the interval length within a range of 1–3 years. Furthermore, there is a stable and acceptably high participation in the second screening round. This implies that screening intervals can be tailored to local resources.
- Colorectal cancer screening
- repeated faecal immunochemical testing
- interval length
- participation
- detection rate of advanced neoplasia
- cost-effectiveness
- decision analysis
- screening
- gastrointestinal cancer
- faecal incontinence
- Helicobacter pylori
- gastritis
Statistics from Altmetric.com
- Colorectal cancer screening
- repeated faecal immunochemical testing
- interval length
- participation
- detection rate of advanced neoplasia
- cost-effectiveness
- decision analysis
- screening
- gastrointestinal cancer
- faecal incontinence
- Helicobacter pylori
- gastritis
Significance of this study
What is already known about this subject?
-
Recent studies have indicated that faecal immunochemical testing (FIT) is superior to guaiac-based faecal occult blood test screening both with respect to participation and diagnostic yield.
-
Not all advanced neoplasia will be detected with a single FIT test owing to suboptimal sensitivity for such lesions.
-
Successive screening rounds are therefore necessary for an optimal preventive effect in the target population.
-
There are no data on the comparison of different intervals for repeat FIT screening and their impact on the participation and detection rate of advanced neoplasia.
What are the new findings?
-
The positivity rate and detection rate of advanced neoplasia were significantly lower in the second screening round than in the first round of screening.
-
There was no association between the interval length within a range of 1–3 years and the detection rate of advanced neoplasia at the second screening round.
-
Second round participation was stable and acceptably high with screening intervals of 1–3 years.
How might it impact on clinical practice in the foreseeable future?
-
These results can be used for optimal FIT screening strategy planning, with intervals tailored to local resources, in particular the available budget and colonoscopy capacity.
Introduction
Colorectal cancer (CRC) is a major health problem in the Western world which fulfils the conditions for population-based screening.1 There is considerable evidence that annual to biennial screening of asymptomatic individuals at average risk using a guaiac-based faecal occult blood test (gFOBT) can detect cancers at an early curable stage, which results in a reduction of 15–33% in CRC-related deaths.2–5 Based on these results, repeated FOBT screening has been advocated in international guidelines.6–8 Recent studies have indicated that faecal immunochemical testing (FIT) is superior to gFOBT screening, both with respect to participation and diagnostic yield.9–11 The introduction of FIT-based screening is therefore widely considered and implemented in the USA, Canada and many countries throughout Europe. Unfortunately, a single FIT is insufficient for the detection of all advanced neoplasia (ie, all patients with CRC or an advanced adenoma, usually defined as an adenoma of ≥10 mm, an adenoma with ≥25% villous histology or with high-grade dysplasia) due to a suboptimal sensitivity for such lesions.12 This necessitates successive screening rounds, which may result in a similar preventive effect as a screening strategy with an invasive highly sensitive test such as colonoscopy.13 However, there are no data on the comparison of different intervals for FIT screening and their impact on participation and detection of advanced neoplasia, two factors which both highly determine the efficacy of a screening programme.
The aim of this study was therefore to compare the participation and diagnostic yield of repeated FIT testing with screening intervals of various lengths ranging from 1 to 3 years in a population-based CRC screening trial.
Methods
Study population
Details about the design of our ongoing population-based CRC screening programme have been described elsewhere.9 ,14 ,15 In short, demographic data of all individuals aged 50–74 years living in the southwest of The Netherlands were obtained from municipal population registers. Random samples were taken from the target population by a computer-generated algorithm (Tenalea, Amsterdam, The Netherlands). Selection was performed per household and occurred before invitation. Since there is no CRC screening programme in the Netherlands, the target population invited for this trial was screening-naïve when first approached. Exclusion criteria were asked for on the informed consent form that had to be completed by the subject being screened. Exclusion criteria were a history of CRC; inflammatory bowel disease; an estimated life expectancy of less than 5 years; a colonoscopy, sigmoidoscopy or double-contrast barium enema within the previous 3 years; and inability to give informed consent. Recruitment took place between November 2006 and December 2010.
Interventions
With each screening round one FIT (OC-Sensor Micro, Eiken Chemical Co, Tokyo, Japan) was sent by mail to collect a single sample of one bowel movement. The test was considered positive when the haemoglobin (Hb) concentration in the FIT sample was ≥50 ng/ml, which corresponds to 10 μg Hb/g faeces. Details about the study design have been described elsewhere.9 ,14–16 All study subjects were divided into three groups to undergo repeat FIT testing at various screening intervals. The groups were designated in relation to the interval length, expressed in years, between the consecutive FITs.
Study groups
Groups I–III: Repeat 1-sample FIT screening
Subjects assigned to groups I–III were offered repeat 1-sample FIT screening at intervals of 1, 2 or 3 years, respectively (figure 1). In order to complete the repeat FIT screening trial, we started with recruitment of subjects who were scheduled for a longer interval. Recruitment for groups II and III took place between November 2006 and December 2007. Individuals selected for group I received their first invitation between May and November 2008. In each group, invitees who fulfilled the exclusion criteria after the first invitation, those who tested positive during the first screening round, individuals who had become ≥75 years of age and those who had moved out of the region or had died were not approached for the second screening round.

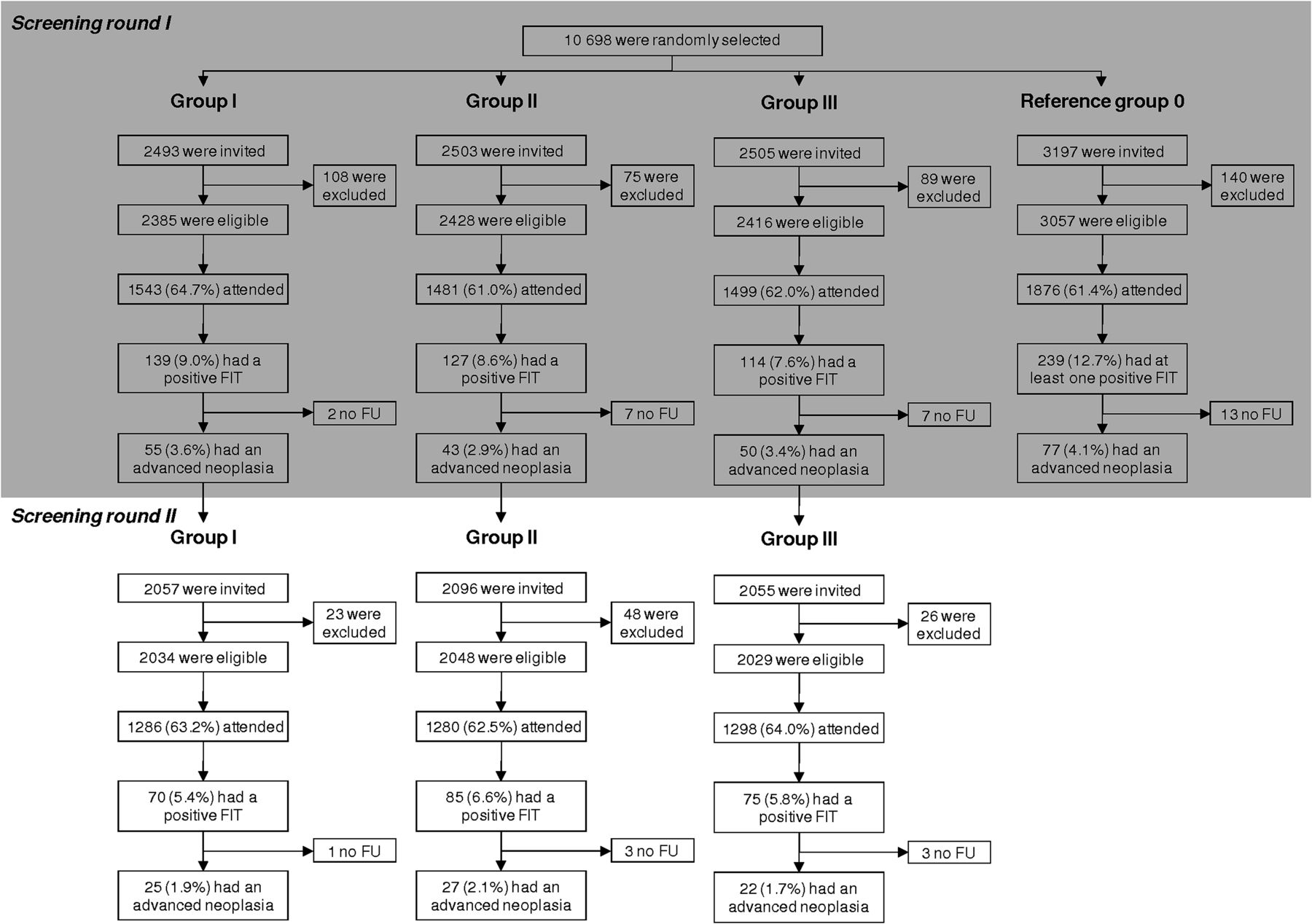{kind=link}
Trial profile. Groups I, II and III: Individuals were invited for a second 1-sample FIT screening round after 1, 2 and 3 years, respectively. Reference group 0: Individuals were invited for their first 2-sample FIT screening round. Screened individuals with a positive test result in the first screening round, subjects who fulfilled the exclusion criteria of the first round, individuals who had moved out of the region, had died, or reached >75 years were not invited for a second FIT-based screening round. Advanced neoplasia was defined as a colorectal cancer and an adenoma ≥10 mm, an adenoma with ≥25% villous histology or with high-grade dysplasia. FIT, faecal immunochemical test (OC-Sensor Micro), cut-off value 50 ng haemoglobin/ml; FU, follow-up after a positive test result (ie, colonoscopy).
Reference group 0: Once-only 2-sample FIT screening
Subjects assigned to reference group 0 were offered once-only 2-sample FIT screening (figure 1). All subjects who were randomly selected for this group simultaneously received two FIT kits. Explicit instructions were given to obtain a single stool sample per FIT and to use both FITs on two consecutive days while noting the sampling date on both test tubes. Recruitment took place between October 2008 and June 2009. The results of this once-only 2-sample FIT group have been published previously.15 Only those data relevant to the current comparison with repeat FIT testing with longer screening intervals are presented in this paper.
Follow-up evaluation
Subjects with a positive FIT were scheduled for colonoscopy within 4 weeks. All colonoscopies were performed by experienced endoscopists. The maximum reach of the endoscope, adequacy of bowel preparation as well as the characteristics and location of any polyps were recorded. All removed polyps were evaluated by experienced gastrointestinal pathologists.17 ,18 Patients with a positive colonoscopy entered a surveillance programme, while patients with a negative colonoscopy were referred back to the screening programme but were considered not to require FIT screening for 10 years.6 ,19
Screen-detected and interval carcinomas
Except for individuals who moved out of The Netherlands, all recruited participants were followed for the development of CRC. Screen-detected cancers were defined as cancers identified at colonoscopy performed after a positive test result. Interval cancers were defined as CRCs diagnosed within the time period between two consecutive screening rounds. Interval cancers were identified through record linkage with the Dutch Comprehensive Cancer Centre (http://www.iknl.nl).
Power calculation
The primary outcome measurement was the participation rate for each screening strategy. The sample size was chosen based on a presumed 50–60% participation rate to yield an 80% power to determine second round participation rates for each group with a confidence interval (CI) of ±2.5%.
Statistical analysis
Differences in proportions between the screening interval groups were tested using the χ2 test. Differences in means between the various groups were tested using the Student t-test. The participation rate was calculated by dividing the number of participants by all eligible subjects (defined as all invitees minus the individuals who fulfilled the exclusion criteria). The positivity rate (PR) was defined as the proportion of participants having a positive test result, the positive predictive value (PPV) as the proportion of participants with a positive test result having advanced neoplasia, and the detection rate (DR) as the proportion of participants having an advanced neoplasia. Participants with more than one lesion were classified according to the most advanced lesion found.
A logistic regression model was fitted to the data to determine differences in second round participation between the three interval groups (ie, groups I, II and III). In a subgroup analysis we extended this model by adding (non-)participation in the first screening round as a separate parameter. In a subsequent multivariate logistic regression model the variables age, sex, and socio-economic status were added. A second logistic regression model was fitted to the data to determine differences in PR, PPV and DR between groups I, II and III. Because participants with a positive screening test followed by colonoscopy during the first round were not invited for the second screening round, participants could only have one positive FIT result. This allowed us to combine the test outcomes from both rounds in a simple logistic regression analysis without using multilevel techniques. A third logistic regression model was used to determine the differences in second round PR and DR (subdivided into (non)-participation in the first screening round) between the three interval groups. All p values were two-sided and considered significant if <0.05. Statistical analysis was performed with SPSS 15.0 for Windows. Finally, we performed an analysis in which the once-only 2-sample FIT group was considered to be a 1-sample group which was reinvited for a second screening round after an interval of zero years (ie, reference group 0). The 2-sample FIT data presented under the subheading ‘First sample/screening round I’ were obtained when the average of the PR and DR of the first and second performed test was taken as reference. The data presented as ‘Second sample/screening round II’ were obtained when the same data of both performed tests were used to determine the added value of a second test. Additionally, for these analyses only individuals who participated twice were considered appropriate. This comparison is presented in table 3.
Results
Participation rate
During the first screening round of groups I–III, a total of 7501 asymptomatic subjects of average risk were invited (table 1), of which 272 (3.6%) were excluded from analyses after the invitation had been sent (223 individuals met one of the exclusion criteria, 41 had moved away and 8 had died) (figure 1). Of the remaining subjects, 4523 responded to the first round invitation. The participation rate was 64.7% (95% CI 62.8% to 66.6%) in group I, 61.0% (95% CI 59.0% to 62.9%) in group II and 62.0% (95% CI 60.1% to 64.0%) in group III. A total of 1021 individuals (13.6%) were not reinvited for the second screening round (380 subjects had tested positive during the first screening, 342 individuals had become ≥75 years of age, 88 individuals had died and the remaining 211 subjects had moved out of the region). Therefore, 6208 individuals were approached for the second screening round of which 97 (1.6%) invitees fulfilled the exclusion criteria (figure 1). In group I the participation rate in the second round slightly decreased to 63.2% (95% CI 61.1% to 65.3%). For the biennial and triennial screening groups, participation increased towards 62.5% (95% CI 60.4% to 64.6%) and 64.0% (95% CI 61.9% to 66.0%), respectively. In a multivariate analysis in which we corrected for participation in the first screening round, the interval length was associated with second round participation (p=0.04). Higher second round participation was achieved with biennial screening (odds ratio (OR) 1.18, 95% CI 0.98 to 1.43) and triennial screening (OR 1.26, 95% CI 1.04 to 1.52) compared with annual screening.
Baseline characteristics (first screening round)
Of first round participants, 89.8% (1166/1299; 95% CI 88.0% to 91.3%) also attended the second screening round after an interval of 1 year, 90.9% (1123/1235; 95% CI 89.2% to 92.4%) after an interval of 2 years and 91.3% (1138/1247; 95% CI 89.6% to 92.7%) participated again after a triennial screening interval (table 2). The same calculations were made for the non-participants of the first screening round: the proportion of eligible previous non-participants attending the second screening round was 16.3% (120/735; 95% CI 13.8% to 19.2%), 19.3% (157/813; 95% CI 16.7% to 22.2%) and 20.5% (160/782; 95% CI 17.8% to 23.4%) for groups I, II and III, respectively. No interaction was found between the parameters ‘first round participation’ and ‘interval length’ (p=0.86), indicating that the difference in second round participation for participants and non-participants in the first screening round (expressed in ORs) was the same in the three interval groups.
Overview of participation and FIT performance characteristics per screening round
Finally, a separate analysis was made of the cumulative participation rate after two 1-sample FIT screening rounds. In the group with an interval of 1 year, 69.7% (1663/2385; 95% CI 67.9% to 71.5%) of all eligible subjects participated at least once, compared with 67.5% (1638/2428; 95% CI 65.6% to 69.3%) in the biennial screening group and 68.7% (1659/2416; 95% CI 66.8% to 70.5%) in the triennial screening group. The interval length was not associated with the cumulative participation rate after two successive screening rounds (p=0.24).
Proportion of positive tests
At a Hb concentration ≥50 ng/ml, a total of 380/4523 (8.4%, 95% CI 7.6% to 9.2%) first round participants tested positive.
In the second screening round a total of 230/3864 (6.0%, 95% CI 5.2% to 6.7%) screened individuals tested positive. In a multivariate model, the overall PR was significantly lower in the second round than in the first screening round (OR 0.69; 95% CI 0.58 to 0.82). Among subjects who had tested negative during the first screening, the PRs in the second screening round were not significantly different between the three interval groups, being 5.1% (95% CI 4.0% to 6.6%) for group I, 6.8% (95% CI 5.4% to 8.4%) for group II and 5.6% (95% CI 4.4% to 7.1%) for group III (p=0.23, table 2).
Follow-up and test performance characteristics
Of the 380 subjects screened in groups I–III who tested positive during the first screening round (table 2), 364 (96%) underwent a successful colonoscopy. The remaining 16 subjects either refused a colonoscopy or their comorbidity was too severe to benefit from an invasive endoscopic procedure. Colonoscopy resulted in the detection of advanced lesions in 148 patients (PPV 41%; 95% CI 35.7% to 45.8%), consisting of 126 advanced adenomas and 22 CRCs of which 17 (77%) were classified as early stage (14 stage I, 3 stage II) and five (23%) as advanced (stage III). In the second screening round, 223 (97%) of the 230 positive subjects screened underwent colonoscopy and advanced lesions were found in 74 patients (PPV 33%; 95% CI 27.3% to 39.6%), consisting of 67 advanced adenomas and seven CRCs of which six were early stage (5 stage I, 1 stage II) and one was stage III. The difference in PPV between the first and second round of FIT screening was not statistically significant (p=0.07).
Overall, 148 of 4523 participants in the first screening round were diagnosed with an advanced neoplasia, corresponding with a DR of 3.3% (95% CI 2.8% to 3.8%), without significant differences between the three groups (p=0.60, table 2). In the second screening round the overall DR of advanced colonic lesions fell to 1.9% (95% CI 1.5% to 2.4%), significantly lower than in the first round (OR 0.57; 95% CI 0.43 to 0.76). In addition, significantly fewer CRCs were found during the second screening round (0.18%; OR 0.37; 95% CI 0.16 to 0.86) than in the first round (0.49%). Among first round participants, the overall DR with a second FIT was 1.8% (95% CI 1.4% to 2.3%; table 3, Second sample/screening round II), without significant differences between the three groups being 1.6% (95 CI 1.0% to 2.5%) in group I, 2.1% (95% CI 1.4% to 3.1%) in group II and 1.6% (95% CI 1.0% to 2.5%) in group III (p=0.62, table 2). In contrast, among non-participants in the first screening round, the second round DR was 3.2% (95% CI 1.9% to 5.3%) which, as expected, is similar to the rate of 3.3% among the participants in the first screening round and significantly higher than the second round DR among those who had participated in the first screening round (p=0.02).
Overview of positivity rate and detection rate per screening round for either 1-sample FIT screening (ie, groups I-III) or 2-sample FIT screening (ie, reference group 0)
Looking at the once-only 2-sample FIT group, the DR of advanced neoplasia of a single test was 3.3% (95% CI 2.6% to 4.2%) (table 3, First-sample/screening round I). The additional second FIT sample enabled detection of 16 additional advanced neoplasia in 1876 participants, corresponding with an additional DR of 0.9% (95% CI 0.5% to 1.4%) (table 3, Second sample/screening round II) and thus an overall DR of 4.1% (95% CI 3.3% to 5.1%).
Interval carcinomas
After record linkage with the Dutch Comprehensive Cancer Centre, 32 CRCs were found in the total study population. Twenty-nine CRCs (90.6%) were screen-detected tumours (table 2), of which 22 (76%) were detected during first round screening and seven (24%) during second round screening. The other three (9.4%) were interval cancers. Two of those were detected in the 4143 first round participants with a negative test: one stage III tumour (FIT result at baseline, 24 ng Hb/ml) was detected 9 months after baseline screening and one stage II cancer (7 ng Hb/ml) was discovered 2 years and 5 months after stool sampling. The third and last CRC was diagnosed at stage I in one of 117 subjects with a positive first round test (960 ng Hb/ml) but negative follow-up colonoscopy. The tumour was located 50 cm from the anal verge. Reassessment of the original colonoscopy report and pictures revealed no explanation for this lesion being missed.
These results imply that, in the first screening round, 0% (0/4) of all CRCs diagnosed in group I were interval cancers. The corresponding percentages for interval cancers were 9.1% (1/11) for the biennial screening group and 20.0% (2/10) for the triennial screening group.
Discussion
The effectiveness of FIT-based screening in decreasing CRC-related mortality has not been studied in large long-term prospective randomised controlled trials. Although such trials would be highly valuable, they may never be conducted. CRC screening programmes using FITs are therefore based on evidence from prospective randomised controlled trials showing that annual or biennial gFOBT screening led to a reduction of 15–33% in CRC mortality2–5 combined with observations from other randomised trials that FIT screening compared with gFOBT is associated with higher participation and diagnostic yield.9 ,11 This forms the basis for the assumption that repeat FIT screening will eventually have a larger impact on CRC-related mortality than gFOBT screening. This is further supported by modelling results.13 ,20 The effectiveness of a FIT-based screening programme is, however, highly dependent on adherence to repeat testing. This trial demonstrates that participation increases slightly with second round screening when performed at biennial or triennial intervals. This increased participation was seen in both first round participants and first round non-participants, in particular in the triennial screening group. This underlines the importance of reinviting previous non-participants to increase the effectiveness of screening. Unfortunately, this is not routinely applied in CRC screening programmes.21 Optimising participation rates must be a priority in any screening programme and requires scrutiny of health promotion campaigns, invitation techniques, the test kit and involvement of general practitioners.14 ,22–24
Besides pursuing high participation in repeat screening, the detection rate of advanced neoplasia is of similar importance for the effectiveness of screening. Repeated screening rounds enable a larger proportion of the population to be covered and help to detect more subjects with advanced lesions, both because of the gradual progression and the intermittent bleeding pattern of advanced neoplasia.15 As a consequence, CRC screening requires successive screening rounds for an optimal preventive effect. This trial first demonstrates that repeat FIT screening enables a greater population coverage and a higher detection rate of advanced neoplasia, even when compared with single round 2-sample FIT screening.15 The cumulative coverage of the target population was 67.5–69.7% in the repeat 1-sample FIT screening groups compared with 61.4% in the once-only 2-sample FIT group, and the cumulative DR of advanced neoplasia ranged from 5.3% to 5.7% in the repeat 1-sample FIT screening groups compared with 4.1% in the once-only 2-sample FIT group. Second, our study demonstrates that second round FIT screening yields fewer advanced neoplasia compared with baseline screening. This finding confirms that FIT screening has a considerable yield of advanced neoplasia already with single round screening.10 ,25 Third, this study shows that there is no association between the interval length within a range of 1–3 years and the DR of advanced neoplasia at the second screening round. This finding was, to some extent, against our assumption that a longer screening interval would result in more newly bleeding advanced neoplasia at the second screening round. Our current findings support the concept of slow progression of sporadic colorectal neoplasia. Finally, these findings could also suggest that non-bleeding advanced neoplasia persist in a non-bleeding state for a long time. This issue needs further research.
We performed additional analyses for the positivity rate and detection rate, including only participants who attended both screening rounds (table 3). Since the DRs in the three interval groups did not differ, corresponding data were pooled (ie, groups I–III) and compared with 2-sample FIT screening where the second test was performed after a virtual interval of zero years. The pooled data showed that 1.8 advanced neoplasia per 100 participants were detected during the second screening in groups I-III compared with 0.9 after an interval of zero years (ie, the second test of the once-only 2-sample FIT screening on two consecutive days). These figures imply that 50% of advanced neoplasia detected at second round screening could have been detected at baseline but were not bleeding (consistently) enough at that time to be detected by one FIT. Moreover, the fact that the second round DRs did not differ between groups I–III suggests that even a triennial screening interval might be too short to detect genuine newly developed or at least newly bleeding advanced neoplasia. This is consistent with the long so-called ‘polyp dwell time’—that is, the average time for transformation from a small adenoma to an invasive CRC—which is estimated to be on average at least 10 years.1 In this respect, it is important to note that the sensitivity of FIT for the detection of low concentrations of blood in stool samples, in particular at a low cut-off value which was used in this trial, leads to a considerably higher detection rate of advanced neoplasia than screening with gFOBT. For instance, in our previous randomised comparative trial, gFOBT and FIT screening led to the detection of six and 20 subjects, respectively, with an advanced neoplasia per 1000 subjects invited for screening.10 The majority of these subjects had advanced adenomas, not cancer. This shows that adenomas can bleed before becoming an invasive cancer, and single FIT sampling at a low cut-off detects part of these lesions. Therefore, while current international CRC screening guidelines recommend that FOBT screening should apply fixed 1-year intervals with a single test,6–8 our data suggest that FIT screening may progress to faecal sampling with longer intervals. This strategy may be further improved by using two FIT samples in every screening round, with optimisation of the number of days or bowel movements between FIT sampling.15 If this is true, such a multiple sample strategy with longer screening intervals could become more advantageous than a 1-sample FIT strategy with a shorter interval.
To our knowledge, this is the first study to evaluate the second round participation and diagnostic yield of a FIT-based CRC screening trial comparing different interval lengths between successive screening rounds. Moreover, comparatively little is known about the outcome measures of the first versus subsequent screening rounds in CRC screening. Most available studies were conducted with the gFOBT, which has been used for more than 40 years.26–30 Additionally, the majority of FIT-related data published so far have not been tabulated by screening round and therefore do not allow analysis of participation and diagnostic yield per screening round.31–35 One exception is an Italian study in which all individuals were invited for biennial 1-sample FIT screening.36 Our main results concerning second round participation and diagnostic yield are in line with these Italian results. However, when the same Hb concentration threshold was used (ie, 100 ng/ml), we observed a lower first round PR and a higher DR of CRC. Potential explanations for the lower number of detected cancers in the Italian study included the younger population (aged 50–69 years vs 50–74 years) and the lower proportion of positive subjects screened undergoing follow-up colonoscopy (86% vs 96% respectively). It is difficult to explain differences in PR since the brand name of the used FIT kit was not provided, neither were additional baseline characteristics of the target population given.
This study has some limitations. First, the invitations for the first screening round were not sent at the same time. Since the recruitment of all groups took place in the same screening-naïve population, more awareness about CRC and CRC screening could have been obtained over time. This implies that the participation rate of group I at first screening and group III at second screening could have been affected the most by this potential bias as these were invited later in time. This increased awareness about CRC screening would then explain the higher first round participation seen in the annual FIT screening group compared with groups II and III, although this contrasts with the lower second round participation in this same group. Second, this trial was powered on participation and therefore lacks power to detect small differences in second round PRs and DRs between the different interval length groups. Additionally, although no significant differences were found in the total number and stage of advanced neoplasia between the three interval groups, this has to be confirmed with further studies.
In conclusion, this comparative population-based CRC screening trial demonstrates that the association, if any, between longer screening intervals and larger numbers of advanced neoplasia detected at repeat FIT screening is limited. Furthermore, this trial shows a stable and acceptably high participation in the second screening round within a range of 1–3 years. This implies that screening intervals can be tailored to local resources.
Acknowledgments
The authors would like to thank the members of the advisory board (A Cats, J W W Coebergh, R A M Damhuis, E H Eddes and J van Krieken), H 't Mannetje for retrieval of demographic data of all potential participants in the target population, E van der Donk (Tenalea) for the random selection of invitees, all general practitioners in the region, gastroenterologists and surgeons of the Erasmus University Medical Centre, IJsselland Hospital, St Franciscus Gasthuis Hospital, Vlietland Hospital, Haven Hospital, Ikazia Hospital, Medical Centre Rijnmond-South and Albert Schweitzer Hospital, residents, secretaries, nurses and all participants of the trial.
References
Footnotes
-
Funding This trial was funded by the Dutch Cancer Society (EMCR 2006-3673), the Dutch Ministry of Health, Health Care Prevention Program-Implementation (ZonMw 63300022 and ZonMw 120720011), Olympus Medical Systems Europe GmbH, Hamburg, Germany, the Jacoba Foundation and Eiken Chemical Co, Tokyo, Japan. The funding sources had no influence on study design, data collection, monitoring, analysis and interpretation of results or the decision to submit the manuscript for publication.
-
Competing interests None.
-
Ethics approval The study was approved by the Dutch Ministry of Health (PG/ZP 2.727.071 and PG/ZP 2.823.158). The study letters and information brochures were approved by the Institutional Review Board at the Erasmus University Medical Centre (MEC-2005-264 and MEC-2008-029).
-
Provenance and peer review Not commissioned; externally peer reviewed.