Article Text

Abstract
Objective: Occupational workload has been associated with an increased risk of osteoarthritis. The objective was to further examine the association between workload and occurrence of osteoarthritis and in particular to study whether heavy workload has similar importance as a causative factor for osteoarthritis of the hip and knee.
Methods: In a cohort study, the authors investigated the incidence of surgically treated osteoarthritis in the hip and knee among men employed in the Swedish construction industry (n = 204 741). Incident cases were found by linkage with the Swedish hospital discharge register between 1987 and 1998. Incidence rates adjusted for age and BMI were compared between different occupational groups.
Results: The incidence rates for osteoarthritis in hip and knee were positively correlated (r = 0.62; p = 0.01). There was a significantly increased risk of surgically treated osteoarthritis in the knee among floor layers, asphalt workers, sheet-metal workers, rock workers, plumbers, brick layers, wood workers and concrete workers. Even if there was a trend towards increased relative risks for osteoarthritis in the hip in floor layers, asphalt workers, wood workers and concrete workers they were not statistically significant. The relative risk for surgically treated osteoarthritis of the knee was 4.7 (95% CI 1.8 to 12.3) among floor layers, indicating an attributable fraction for work factors of 79%.
Conclusions: This study shows that some work-related factors seem to be risk factors for osteoarthritis both in the knee and hip. However, the risk factors seem to be of greater importance for osteoarthritis in the knee compared with the hip. This study indicates that at least 50% of the cases of severe osteoarthritis of the knee can be prevented through decreasing occupational risk factors in some occupational groups.
Statistics from Altmetric.com
Mechanical factors such as heavy load on the joint are important mechanisms behind primary osteoarthritis (OA) in the hip and knee. Obesity, overweight and heavy physical activity in sports have been found to be associated with increased risk for OA of the hip and knee in several studies.1–3 Some studies have found an increased risk in workers with heavy workloads, although some reviewers consider the evidence as moderate for an association between heavy load in work and OA in the hip and knee.4–12 The objective of this study was to further examine the association between workload and occurrence of OA and in particular study whether heavy workload has similar importance as a causative factor for OA of the hip and knee.
MATERIALS AND METHODS
The study base is a cohort of construction workers participating in a national health control programme. Swedish construction workers were invited to participate in health controls on a regular basis from late 1960 until 1992 in a nationwide occupational health centre programme (Bygghälsan) according to a collective agreement between the employers’ associations and the unions. The participation rate in the health controls has been estimated to at least 80% (Englund A, personal communication). The workers’ job title, smoking habits, body weight and height were registered at the examinations and there is a computerised register of results from health examinations that took place between 1971 and 1992. Those in the computerised register constitute the basis for this study, in total 389 132 persons. Health examinations were offered every 3–5 years and the job title from the first health examination was used in the analysis. Swedish construction workers usually stay in the same job; 74% of those participating in more than one examination reported the same job title in subsequent examinations.
The analyses were restricted to men because the database included too few women with surgically treated OA (n = 12 for hip and n = 2 for knee in manual jobs) to make analyses according to job title feasible. The analyses were further restricted to the ages of 15–67 years at the time of the health control as 67 years was the official retirement age in Sweden until 1976, and because few persons started to work before the age of 15 years. Furthermore, only men with a BMI (calculated as weight in kg/(height in m)2) of 17–35 kg/m2 were included. In the analyses we used the bodyweight and length measured at the time of the first health control. Linkages with official Swedish registers were used for information about whether a person was alive, deceased or had emigrated. A small percentage (0.15%) of workers were not found in any register and were excluded from the analyses. Thus, of the 389 132 persons there were in total 204 741 men included in the study, of whom 9136 were white-collar workers.
The occurrence of surgically treated OA of the knee and of the hip was collected from a linkage with the Swedish Hospital Discharge Register, which holds information on persons who have been hospitalised for at least one day. This register has nationwide information from 1 January 1987. We included data until 31 December 1998. To be classified as a case with OA the worker should have been treated surgically for primary OA in the hip or the knee. The register contains codes for diagnoses as well as for surgery performed. The patients can have several diagnosis and surgery codes at each admission. We excluded cases classified as traumatic or with OA secondary to other diseases such as rheumatoid arthritis. Also, cases treated for a secondary hip or knee replacement were excluded. Thus, in this study, to be classified as OA of the hip, a person with a diagnosis of OA (ICD 9: 715B; ICD 10: M16.0, M16.1) also had to had a hip replacement performed (register codes 1987–96: 8410, 8414; codes 1997–8: NFB29, NFB39, NFB49, NFB99). Correspondingly for the knee, besides a diagnosis of OA of the knee (ICD 9: 715B; ICD 10: M17.0, M17.1), a knee replacement was required (register codes 1987–96: 8423, 8424; codes 1997–8: NGB09, NGB19, NGB29, NGB39, NGB49, NGB99).
We have previously used this cohort to study the association between whole body vibration, body weight, smoking and age and OA.3 13
The observation period was from the year after the health examination or 1 January 1987, whichever came last, until 31 December 1998 or death, emigration or the occurrence of surgically treated hip or knee OA, whichever came first. For each calendar year the number of person-years was calculated according to the person-year method, stratifying for BMI (17–19, 20–24, 25–29, 30–35) and age class (10-year age classes).14 Only those aged 40–79 years were included in the analysis, as a replacement is very rare before the age of 40 (n = 0 for hip and knee in this study).
Attributable risk was calculated as (RR-1)/RR. Ninety five per cent confidence intervals for the incidence rates were calculated assuming a Poisson distribution. Mantel-Haenszel statistics were used to estimate relative risk with 95% CIs, stratifying for age and BMI, using white-collar workers as a control group.15
The study was approved by the Umeå University Committee of Ethics (DNR 99–140).
RESULTS
In total there were 1260 cases of surgically treated OA of the hip and 420 cases of surgically treated OA of the knee among the male workers (table 1).
In some occupational groups there were few cases and the further analyses were restricted to groups with five cases or more. The crude and adjusted incidence rates are presented in table 2.
At the group level, there was a positive association between surgically treated OA in the hip and knee (fig 1). If white-collar workers were excluded from the analysis there was still an association (Pearson’s coefficient of correlation including white-collar workers r = 0.62; p = 0.01; excluding white-collar workers r = 0.58, p = 0.03).
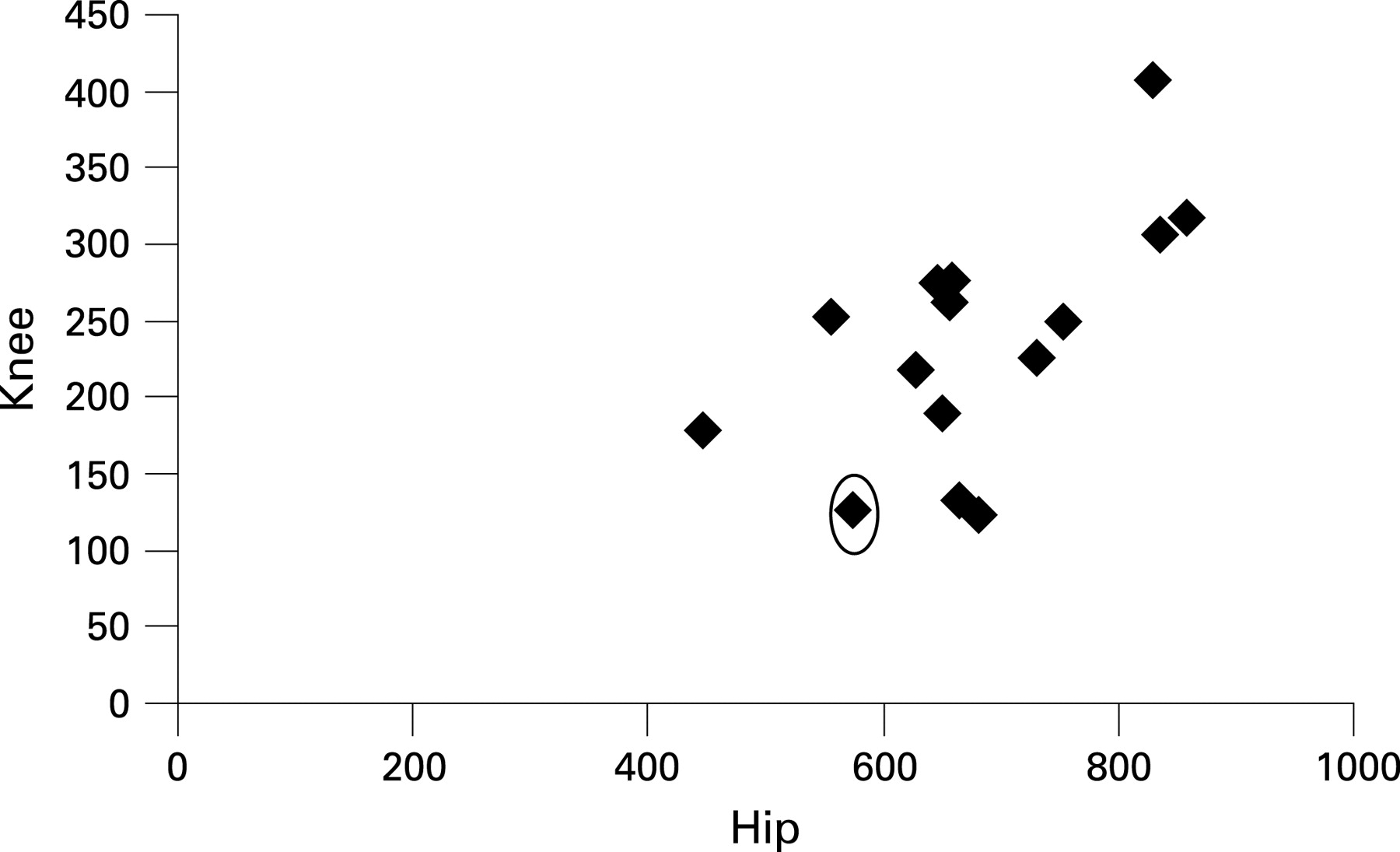
{kind=link}
The incidence rates varied between the occupational groups and were generally higher for surgically treated OA of the hip (table 2). Most manual workers had an increased risk compared with office workers for surgically treated OA of the knee and hip, but the relative risks were higher for OA of the knee (table 3). Only risks for OA of the knee reached statistical significance. The highest relative risk was found among floor layers (RR = 4.7), but several occupational groups had relative risks above 2. The attributable risk for floor layers was 79%, indicating that almost four of five cases of surgically treated OA of the knee are “caused” by factors in the working environment in this group. A relative risk above 2 indicates an attributable risk of at least 50%, Thus, our data indicate that more than every second case of surgically treated OA of the knee in asphalt workers, brick layers, plumbers, sheet-metal workers and wood workers in the construction industry is related to occupational factors. The attributable risks for surgically treated OA of the hip were on the other hand much lower as the highest relative risks are around 1.5, although not statistically significant. A relative risk around 1.5 indicates that every third case is caused by the work environment.
DISCUSSION
The results of this study support the previous view that occupational factors such as workload are of importance for OA of the hip and knee. The study indicates that these factors are of greater importance for OA of the knee, where occupational factors in some jobs seem to cause more than every second case. This means a potential for prevention of OA of the knee by improving the working environment. However, prevention needs knowledge of causative factors and not just occupational titles.
An advantage of this study is the prospective cohort design decreasing the risk of some bias. Some previous investigations are case-reference studies6 7 10 16–18 or cross-sectional studies19 and a recall bias and selection bias may cause associations with factors that increase pain but may be unrelated to the pathogenic mechanisms. A heavy job means that even modest joint pain may cause problems at work and the worker to seek medical consultation and possibly a change of job, while those with less demanding jobs do not see a doctor even if they experience similar pain. Therefore, studies based on patients treated for pain from OA or radiography taken in clinical practice may be biased. Furthermore, the information about diagnosis was collected from a national register and occupation from a health control at least one year before surgery excluding recall bias. Flugsrud et al used a similar design to ours for studying hip replacement.11 They studied a cohort of persons from the general population previously screened for cardiovascular risk (n = 50 034), followed the outcome through an arthroplasty register and found increased risk for replacement associated with physical workload reported at the examination. Construction workers were in their classification included in the two highest categories of physical activity. A Danish prospective study interviewed subjects at two occasions five years apart and found that hip pain was associated with physically demanding work and whole body vibration.20 Their cohort was a sample from the general population (n = 3714).
Some previous studies have found an increased risk of OA of the hip in construction workers. The reason for the non-significant findings in our study may be lack of contrast and misclassification of exposure. All comparisons in this study were within the group of construction workers, and those we considered “low” exposed may be more exposed to heavy physical work than some other groups in society. Even white-collar workers may have had construction jobs during their early career. Some other studies compare risk in the general population, where the gradient between low and high physical workload probably is much higher than in our study.6 10 11 17 A job title in the construction industry may contain variable exposure between time periods and individuals. Such misclassification is mainly non-random causing underestimation of the risks. Thus, our risk estimates for hip OA should be regarded as possibly underestimated and not be used to argue against an association between heavy physical workload and OA in the hip.
Floor layers had the highest risk of OA in the knee. Floor layers may lift heavy rolls of carpet, however we think that kneeling and creeping on the knees is the largest difference in their job compared with other jobs in this study. Previous studies have sometimes focused on squatting; however, workers such as electricians and painters also squat but seem to have a lower risk of OA of the knee. It could also partly be a difference in dose—kneeling may be more prevalent among floor layers. Jensen studied work tasks in floor layers and carpenters and found that floor layers had much more knee-straining work activities.21 In a Finnish study floor layers had at least one knee on the floor 42% of the time, while it was rare in painters (no figure given). Squatting occurred in 3% in both groups.22 A US study found that floor layers more often reported kneeling (score 5.5) than bricklayers (score 2.9).23
Kneeling may also be a cause for increased risk in other jobs, such as concrete workers. A Finnish study compared workloads on the knee of concrete reinforcement workers and painters.24 They observed workers in six sites and found that standing with bent knees was more common among concrete workers (3% vs 0%) while squatting was more common among painters (9% vs 3%).
Other studies have indicated that frequent squatting and kneeling are important causes of OA in the knee but those studies have also indicated heavy lifting as important mechanism.7 12 In an English case-referent study repeated kneeling or squatting and climbing a ladder were significantly associated with knee OA, with about double the risk in men.17 Repeated heavy lifting (>25 kg) was associated with a similar risk in men, but the confidence interval was rather wide (OR 1.7; 95% CI 0.8–3.0). Heavy workload may be an important factor in the increased risk of OA in the knee among rock workers, concrete workers, brick layers and wood workers. Electricians, who rarely have heavy burdens, have a low risk compared with other groups which supports the idea that heavy lifting is also a causal mechanism. The increased risk of OA in the knee among asphalt workers is harder to explain. We have not been able to find any other study of OA among asphalt workers. Climbing and jumping up and down is improbable as a cause as machine operators have no increased risk. Kneeling or creeping is rather infrequent for most asphalt workers and heavy lifting is also rare. Furthermore, they seem to have an increased risk of OA in the hip. Swedish asphalt workers are seasonal workers as it is too cold for paving in the winter. Thus, Swedish asphalt workers often have other jobs in the winter. A possible explanation is that these workers have heavy physical jobs during the winter.
Climbing or jumping on stairs has been suggested as a risk factor for OA in the hip and knee,7 17 but our results do not support that hypothesis. Painters and electricians are occupational groups with high exposure to stair climbing, but their risks seem to be lower than the risk in most other jobs in this cohort. Whole body vibration—for example, from heavy vehicles—has also been suggested as a risk factor, but a previous analysis on this cohort did not support such a hypothesis.13
The attributable risk depends on exposure and comparison group. A risk estimate for a group of workers will depend on their average exposure as it depends on the relative risk. In populations it also depends on exposure prevalence.15 The attributable risk has its advantage in estimating the potential for preventive measures, but comparisons between studies must emphasise differences in population and exposure.
This study shows that there are differences in the risk of OA in the hip and knee between different occupational groups within the construction industry. There is no detailed information about exposure in the different jobs and workload can differ within jobs, so it is difficult to recommend certain measures based on data from this study alone. However, data from other studies in combination with our data indicate that preventive measures in the construction working environment—for example, reducing kneeling and heavy lifting—may prevent more than every second severe case of knee OA in some occupational groups.
Main message
In some jobs occupational factors can contribute to more than 50% of cases of severe osteoarthritis of the knee.
Policy implication
Reducing occupational kneeling and heavy lifting may decrease the risk of severe osteoarthritis.
Acknowledgments
We thank Fritjof Nilsson and Leif Nilsson, who supported the data handling and analysis. This work was supported by the Swedish Council for Working Life and Social Research.
REFERENCES
Footnotes
-
Competing interests: None declared.