Article Text

Abstract
Objectives: To investigate the relation between typical ambient noise levels (highway, rail, road) and multiple mental health indices of school children considering psychosocial and biological risk factors as potential moderators.
Methods: With a two stage design strategy (representative sample and extreme sample) two cross sectional samples (n=1280; n=123) of primary school children (age 8–11) were studied. Individual exposure to noise at home was linked with two indices of mental health (self reporting by the child on a standard scale and rating by the teacher of classroom adjustment on a standard scale). Noise exposure was modelled firstly according to Austrian guidelines with the aid of a geographical information system and then calibrated and corrected against measurements from 31 locations. Information on potential confounders and risk factors was collected by mothers and controlled in regression modelling through a hierarchical forward stepping procedure. Interaction terms were also analysed to examine subgroups of children at risk—for example, low birth weight and preterm birth.
Results: Noise exposure was significantly associated in both samples with classroom adjustment ratings. Child self reported mental health was significantly linked to ambient noise only in children with a history of early biological risk (low birth weight and preterm birth).
Conclusions: Exposure to ambient noise was associated with small decrements in children's mental health and poorer classroom behaviour. The correlation between mental health and ambient noise is larger in children with early biological risk.
- traffic noise
- environmental
- mental health
- low birth weight
- Leq, noise exposure
- dB,A adjusted noise levels
- dB,A,Leq, equivalent sound pressure level
- dB,A,Ldn, equivalent sound pressure day-night level
Statistics from Altmetric.com
- Leq, noise exposure
- dB,A adjusted noise levels
- dB,A,Leq, equivalent sound pressure level
- dB,A,Ldn, equivalent sound pressure day-night level
The present study focuses on the relation between typical, everyday neighbourhood noise levels and children's mental health. Mental health in children is usually measured in one of three ways: psychiatric evaluation of anxiety, depression, conduct disorder, or psychoses; self reported questionnaire measures of clinical symptoms of anxiety, depression, and conduct disorders; or by either teacher or parent ratings of behavioural adjustment. Numerous studies in the child psychiatric and clinical literature indicate the reliability and validity of all three types of measurement for non-clinical populations, with psychiatric evaluation reserved for more serious, clinically relevant symptoms of serious disorders such as disassociation.1–4 In the present study we incorporated child self reported and teacher ratings of mental health. We judged that psychiatric evaluations were overly intrusive and unnecessary for the modest increases in the non-clinical range of mental health symptoms we expected to see in a sample of the general population.
There are several important gaps in the noise and mental health literature considered by the present study. Firstly, previous studies of noise and mental health all focused on major noise sources—such as airports or major highway traffic—and neglect typical neighbourhood noise as experienced by most of the population.5–8 Although it is obviously important to focus noise protection efforts on those most heavily impacted, we should not overlook the fact that nearly half of the World Health Organisation European region is exposed to daily community noise levels of between 55 and 65 adjusted noise levels (dB,A).9 This ambient noise level exceeds recommended criteria for residential areas, schools, and hospitals.10, 11
A second gap we considered is that nearly all studies of noise and mental health have focused exclusively on adults. Only one study has examined noise and mental health in children. Bullinger et al studied 326 8–11 year olds attending primary schools in high noise impact zones and comparison groups around the Munich-Riem airport.12 A third shortcoming in the noise and mental health literature that we considered is the problem of the small sample sizes. This has precluded the incorporation of sufficient multivariate controls for other relevant mental health factors (biological, psychosocial, and environmental risks) and therefore not provided researchers with the opportunity of examining mental health within a multivariate risk model.
A common analytical strategy in environmental epidemiology is to examine the relation between an environmental agent and health, while statistically controlling for other variables. The application of general linear models depends upon the assumption that the slopes of the regression plots for the predictor are parallel across each statistical control (the regression plots all have the same slope).13–15 When this assumption is violated, there is an interaction between the predictor variable (noise) and the control variable as they affect the outcome of interest (mental health). Therefore, it is important to first test whether any control variables interact with the environmental risk factor of interest. The presence of a statistical interaction is also important for theoretical and practical reasons.16, 17 Statistical interactions can help us better understand the nature of environment and health relations, pointing towards potential explanatory mechanisms and processes. From a policy perspective, interactions may uncover vulnerable population subgroups, hidden by weak or non-significant overall effects.
Thus the present study was designed to investigate whether a large representative sample of children living under typical neighbourhood noise levels in small, alpine towns and villages in Central Europe (Austria) would show any relation between a broad range of exposures to noise and two indices of mental health. The sample was sufficiently large so that we could examine multiple biological and social risk factors and as already explained, investigate statistical interactions. We also employed an innovative variant of a classic two stage study design.18 As well as obtaining a broad, representative sample of the population, we also oversampled a subset of children at the high and low ends of the range of exposure to noise in the community. We did this because extreme group analysis, whereas not ecologically representative, has a distinct advantage—they provide substantially greater statistical power.19, 20 This enables investigators in a new area to identify suspected environmental risk factors—such as noise for children—where there is a paucity of knowledge. Such research designs on extreme exposure can uncover early warning signs of a potential public health problem before they reach levels sufficient to be seen in the overall population. This research design also provides possibile internal replication. Do the conclusions from the highly exposed population generalise to the dose-response analysis in the general population?
METHODS
Subjects and procedures
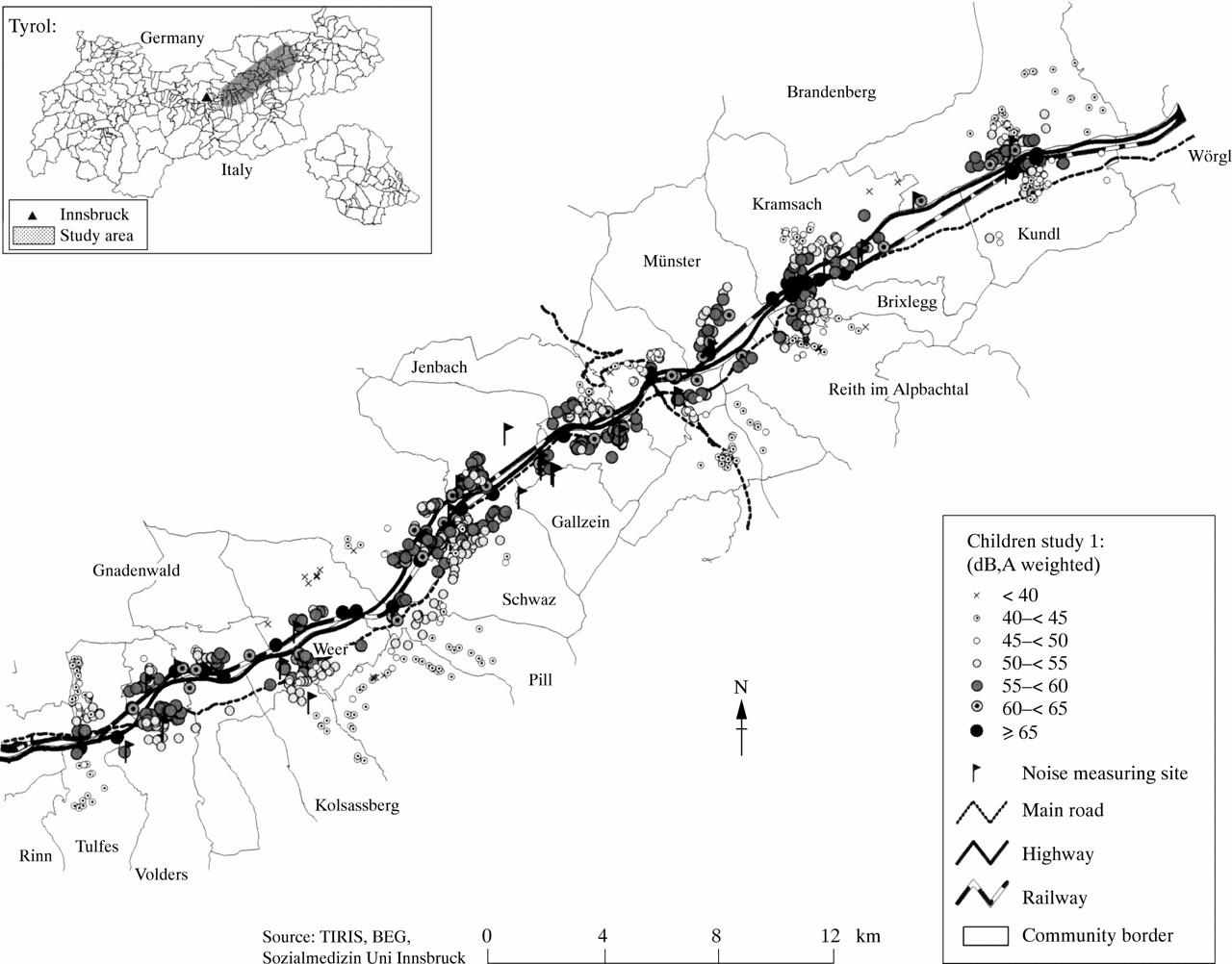
In June 1998 all school children in grades 3–4 (mean 9.44 years) were approached in a demarked area defined by the Austrian Government as an environmental health impact assessment. A total of 1280 children from 26 local schools participated (response 79.5%) after a letter was sent to their parents (population study). Children, their mothers, and their teachers were informed that this was a study of traffic, environment, and health required by law to supplement the environmental health impact assessment. The survey area (about 45 km long) is in the lower Inn Valley of Tyrol in Austria (fig 1. This mainly rural, alpine area consists of small towns and villages with a mix of industry, small business, and agricultural activities outside Innsbruck. A geographical information system was set up to enable multiple data linkages and to ease additional sampling.

Children study 1. Sample distribution across study area by noise exposure levels: from a representative sample of a population study.
After the geographical information system link of calculated noise exposure (equivalent sound pressure level, dB,A,Leq) with the child's home address two new samples of children in grade 4 were drawn in September 1998 from the extremes of the available exposure information (< 50 dB,A,Ldn v > 60 dB,A,Ldn (day-night levels)). Sixty three children inhabited low and 60 resided in moderate and higher noise exposure locations (fig 2). Participation rates in the extreme analysis was lower (64%) because the data were not collected at school and required more time. However, as table 1 shows, the two samples did not differ significantly on various social, lifestyle, and biological factors.
Main characteristics of both study samples

Children study 2. Sample distribution across study area by noise exposure levels: study sampling on extreme exposure (<50 bD,A,Ldn; >60 bD,A,Ldn).
Background information
Sociodemographic data and biological risk information were collected from each child's mother to assess standard risk factors and to check for possible statistical interactions. Prenatal and perinatal data were assessed from doctor's entries in the “mother-child-passports”—every pregnant mother in Austria receives one of these. Biological risk (0 or 1) was defined as low birth weight less than 2500 g or preterm birth less than 37 weeks gestation. Other biological variables recorded were maternal age, parity, and birth order. Further biological, social, and environmental data were collected with a self administered, standardised questionnaire from the mother. Mother's education was scaled along a five point continuum from 9 years of school to graduate work. Family size, single parenthood, house type (1=single family detached, 2=terraced house, 3=multiple dwelling units), duration of residence (years), and months of breast feeding, were recorded.
Exposure assessment
Residential noise exposure is usually assessed by an index that describes the average noise exposure (dB,A) over a specified time period (Leq, day or night or 24 hours). In this study noise exposure (Leq) was assessed first by modelling (Soundplan) the three major sources (highway, rail, local main road) according to Austrian guidelines (ÖAL Nr 28+30, ÖNORM S 5011). The dichotomous sampling for the pilot study was based on this information. Afterwards a calibration study (31 measuring points) was conducted (day and night measurements) and linear corrections were applied to the modelled data when the difference to the measured data exceeded 2 dB. Based on both data sources approximate day-night levels (dB,A,Ldn) were calculated for each child's home to enable comparison with available dose-response data. This calibrated noise exposure information (combined levels from all sources) was used in all the dose-response analyses. The noise range in the field study was between 31 and 81 dB,A,Ldn (95% within 40–65 dB,A,Ldn). The range in the pilot study was 31 to 72 dB,A,Ldn (95% within: 34–50 dB,A,Ldn) in the low exposure group, 52–71 dB,A,Ldn in the high exposure group.
Psychological health
A 22 item scale was formed from two subscales of the KINDL,21 a valid and reliable index of children's quality of life and four items on a sleep disturbance scale. Analyses of the intercorrelations of the three scales showed the potential to combine the scales, which yielded one internally consistent index of psychological health (Cronbach's α=0.87). Children reported from 0=never to 4=very often, how often they experienced various symptoms indicative of anxiety and depression appropriate for a non-clinical population (I feel lonely; I have trouble falling asleep at night; everything I start turns out right). The psychological health scale was administered to children in their classroom by two graduate students who were blind to the child's exposure to ambient noise.
Classroom adjustment
Each child's teacher was asked to rate the child on a standard index of behaviour.22 This 11 item, dichotomous (yes or no) scale was reliable (Cronbach's α=0.80). Sample items included. In general is this child functioning as well as other children his or her own age? Is this child easily distracted during his or her work? The teacher was blind to each child's level of ambient noise exposure.
Statistical procedures
Exposure and survey data were linked through the geographical information system, and statistical analysis was conducted with SPSS 8.0 and S+4.5 including F Harrells' HMISC and DESIGN libraries. Multiple linear regression techniques were used and 95% confidence intervals (95% CIs) were calculated based on normal approximation. Based on existing knowledge, a hierarchical forward stepping procedure was applied.23 We entered first a minimum set of standard risk factors (sex, maternal education, density, house type, biological risk) and noise exposure. Then further testing for the effects of other variables followed (breast feeding, lone parent, birth order, duration of residence). The most consistent and parsimonious set of variables across the four analyses was chosen to test for three prespecified interactions with noise exposure (biological risk, sex, education). No higher order interactions were uncovered. Finally, sensitivity analyses were conducted to test the stability of the estimates.24
RESULTS
Psychological health
Table 2 describes the results for child self reported psychological health. In the population study there are significant main effects due to education, house type, household density, and a borderline effect for sex. While higher education is associated with better psychological health, all the other variables (household crowding, apartment block housing versus single detached housing, male sex) show a negative impact. The main finding of interest, however, is the significant interaction of early biological risk and ambient noise exposure on psychological health. Figure 3 shows the effect of noise exposure (adjusted for maternal education, sex, number of persons in household, and house type) on those with early biological risk whereas children without this risk seem unaffected by noise exposure.
Multiple regression model of children's psychological health (self reporting scale) (comparison of the effects (mean differences (95 % confidence intervals)) in the two samples
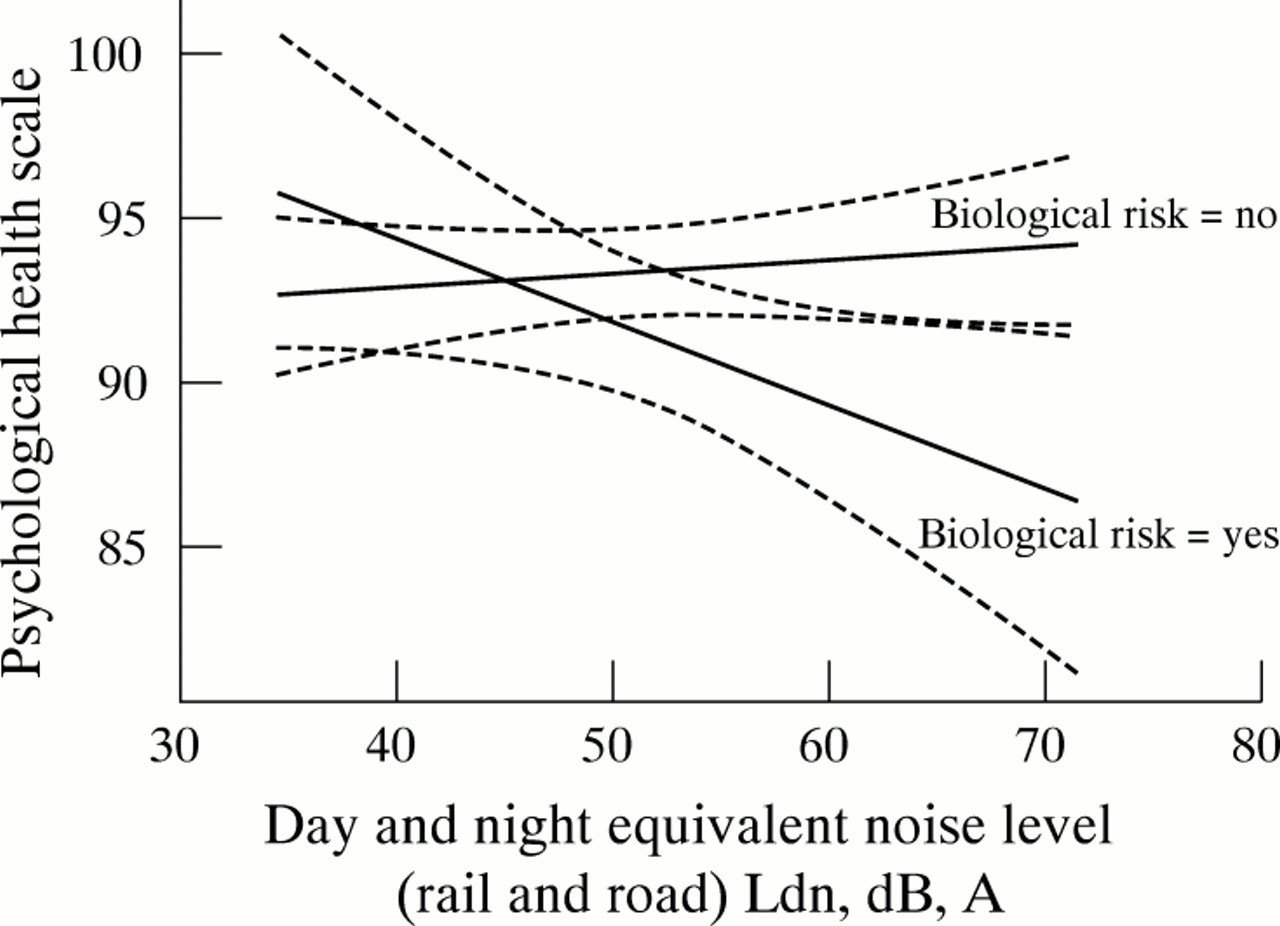
Dose-response (adjusted for maternal education, sex, number of people in household, and house type) for noise exposure and children's psychological health (self reported, based on the KINDL21 and a sleeping scale) by early biological risk (birth weight <2500 g or <37 weeks of gestation) from a representative sample of a population study.
Although the main effects are less consistent in the extreme noise exposure sample, the interaction is replicated and shows large effects (table 3). Note, that the explained variance of the model increases to 23% in the extreme exposure group design.
Children's psychological health*
Classroom adjustment
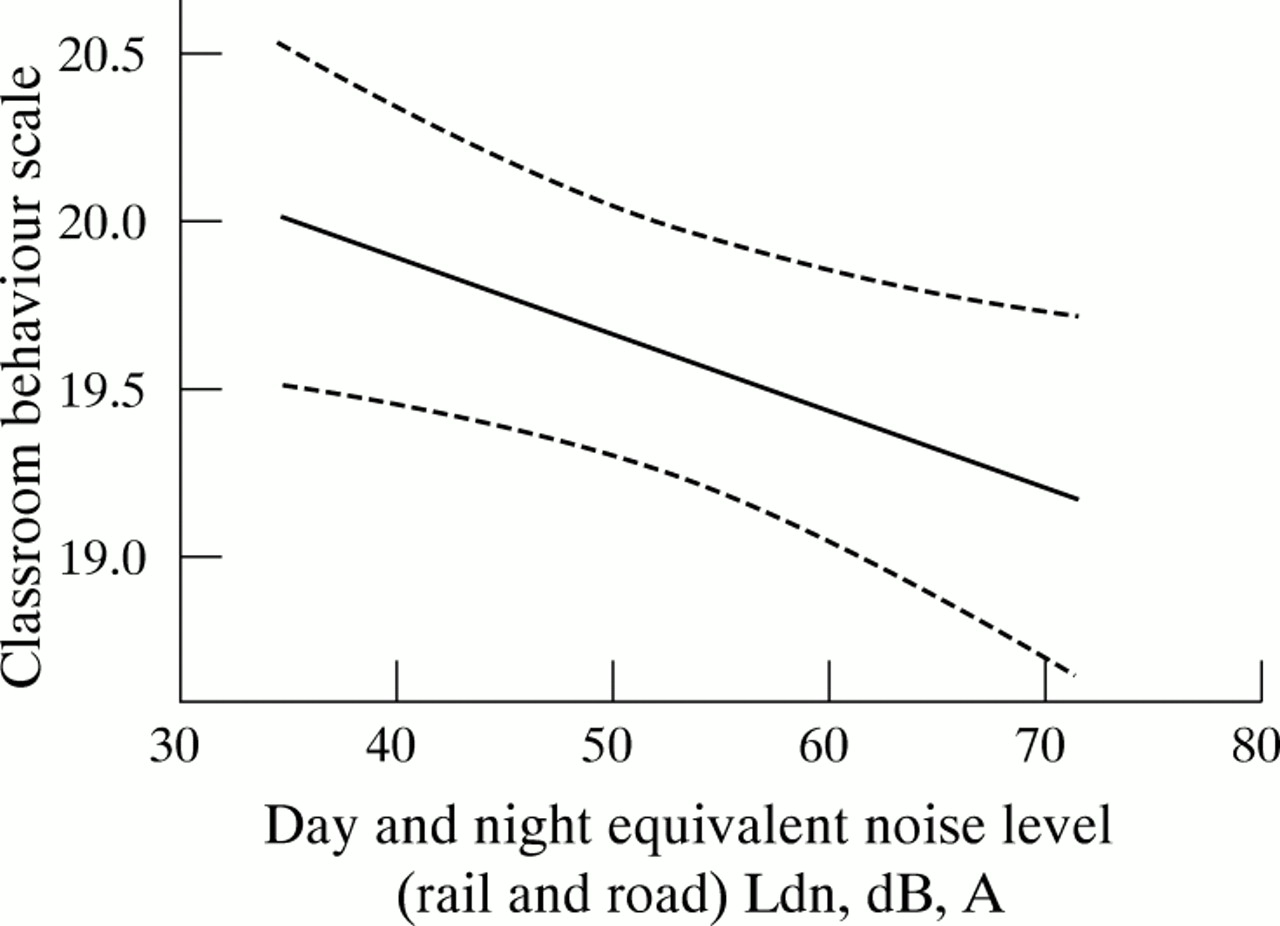
Table 4 presents the regression results for the second outcome measure—the teacher's rating of class room adjustment. In the population study no interaction was detected. However, significant main effects were evident for education, sex, house type, and exposure to noise, and biological risk was marginally significant. The direction of the effect was replicated for all factors, although household density did not reach significance. The total explained variance (R2=0.09) was slightly higher than for psychological health as rated by the children (R2=0.04). Figure 4 presents the adjusted dose-response pattern for the relation between noise and behaviour. A decrement in teacher ratings with increasing ambient noise was evident.
Multiple regression model of children's classroom adjustment (teacher-rating scale) (comparison of the effects of the differences (mean (95 % CIs)) between the two samples)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Dose-response (adjusted for maternal education, sex, number of people in household, and house type) for noise exposure and children's classroom adjustment (teacher rating scale, index of behavioural conduct22) from a representative sample of a population study.
The model results for the extreme exposure analyses resemble the field findings, except that house type and household density reversed their significance. The model total R2 increased to 0.21 from 0.09, again showing enhanced statistical power with the extreme exposure group design.
DISCUSSION
Ambient levels of noise in the community are associated with decreased mental health in elementary school children. This association, a linear dose-response function in a large population study, holds with multiple statistical controls, replicates in two samples, and was robust across reliable and valid self reported measures and teacher ratings. Furthermore, children with low birth weight and preterm delivery may be at greater risk of noise related mental health outcomes.
Data from the population survey indicate that variations in typical community noise levels were associated with psychological symptoms and quality of life reported by the child, but only in those with a pre-existing biological risk (low birth weight, fig 3). This significant interaction was replicated in the extreme exposure study as shown in table 3. It is also interesting to note the evidence of a dose-response function for the high risk subsample in the general population study. For teacher ratings of children's behavioural adjustment, both in the general population and the extreme community noise exposure comparisons (table 4), there were significant main effects of noise on behaviour. All these significant results incorporate multiple adjustments for individual and social factors.
Examining each of our objectives, we showed that typical fluctuations in ambient community noise are associated with mental health among children. This finding replicates the only previous study of noise and mental health among children which showed an association between exposure to airport noise and psychological distress in 8–11 year old children.12 We extend this study by showing similar effects at lower, more typical levels of ambient noise, across two different measures of mental health in children, with a substantially larger array of statistical controls. We also provided the first evidence of a dose-response function between exposure to noise and mental health in children. Only two studies with adults have uncovered dose-response functions between those with high levels of transportation noise and mental health.25, 26 Thus the present study adds to the small amount of literature on noise and mental health in children and provides further evidence of a relation between noise and mental health.
As well as showing that everyday noise may have mental health consequences among children, we examined the potential moderating role of several biological and social risk factors. The data indicate that children who had a low birth weight or were born preterm may be more vulnerable to the adverse mental health consequences of exposure to ambient noise. These children could be more reactive to the harmful consequences of noise because of their known greater susceptibility to behavioural problems in early childhood27–30 or because of physiological effects of “early programming”.31–34 The evidence for greater vulnerability to noise among children with low birth weight is mixed, however. This interaction was restricted to the standardised self reported measure of mental health symptoms. We did not find a similar interaction between noise and biological risk for teacher ratings of behavioural adjustment in the classroom. One possible explanation for this are differences in the symptoms assessed by the two indexes. The self reported symptom checklist focuses primarily on anxiety and depression, whereas the teacher ratings emphasise interpersonal social skills and emotional and attentional regulation in the classroom.
The data on psychological distress reported by the children also illustrate the potential value to public policy of examining moderator functions. In the overall population, there is little or no evidence of mental health sequelae of exposure to noise in the community. This could have led to the incorrect conclusion that therefore ambient levels of noise are irrelevant for mental health among children. As figure 3 and table 3 clearly show, such a conclusion would be incorrect. There is a subsample of children who are reliably at risk of poorer mental health relative to even the lower levels of ambient noise found in rural, central European communities. Furthermore as explained earlier, the uncovering of such an interaction prohibits use of the same variable (low birth weight) as a statistical control when examining the main effects of noise on mental health.
Another objective of our study was to show the potential use of a mixed research design, incorporating both a general population study and a smaller, more focused analysis of people exposed to extreme levels of the environmental risk factor. As a comparison of the results from the two samples shows, the evidence for adverse effects of noise is much stronger in the extreme level comparisons (compare the total R2 in tables 2 and 4 for the two designs). Especially in the early stages of environmental risk investigations there is need for cost efficient designs18, 35 with high sensitivity to detect potential adverse environmental risk factors. The extreme exposure research design does have some limitations: it is not representative of the general population, and, relative to dose response evidence, is more subject to plausible rival hypotheses. None the less enhanced sensitivity to detect potential health effects, coupled with reduced costs and effort, make this type of design worthy of greater consideration in the field of environmental health. Ideally, investigators could combine both research designs in the same study.
It is important to reiterate that the cross sectional design of this study precludes drawing causal inferences. However, our data are stronger than a simple correlational study because of several features: (a) dose response function; (b) the replication and predicted stronger associations in the extreme exposure groups; (c) the use of multiple individual and social controls; (d) the predicted interaction between biological risk and noise. Nevertheless, unmeasured confounders and measurement error could bias the results.36 Short of random assignment of children to different noise exposures, probably the best approach to strengthening the evidence for the casual effects of noise on children's mental health would be to conduct a prospective longitudinal study comparing the same child across different noise conditions. It is worth mentioning that the study by Bullinger et al of aircraft noise and children's mental health was prospective.12
This Journal and other sources document adverse physical health consequences of suboptimal environmental conditions, both in the workplace and at home.37–41 Similar exploration of the mental health consequences of unhealthy social and environmental conditions is just beginning.42, 43 Population studies generating dose-response functions along with comparisons of groups with extreme environmental risk can assist us in this new area of environmental medicine and health. Due consideration of potential moderators is warranted for conceptual, statistical, and policy reasons, in physical and psychological morbidity studies of occupational and environmental health.44–46
Acknowledgments
We thank the many children, families, and teachers who participated in this research project. This research was supported by the Austrian Ministry of Science and Transportation, the Austrian-US Fulbright Commission, the National Institute of Child Health and Human Development, No 1F33 HD08473–01, and the College of Human Ecology, Cornell University.