Article Text

Abstract
Objectives Workers with common mental disorders (CMDs) frequently experience recurrent sickness absence but interventions to prevent this are lacking. The goal of this study was to evaluate the effectiveness of the Stimulating Healthy participation And Relapse Prevention at work intervention in preventing recurrent sickness absence in workers who returned to work after sickness absence due to CMDs.
Methods We performed a cluster-randomised controlled trial with 3 months, 6 months and 12 months follow-up. Treatment providers were randomised to either a 2-day training in the Stimulating Healthy participation And Relapse Prevention at work intervention, that is, a problem-solving intervention, or usual care. Primary outcome measures were the incidence of recurrent sickness absence and time to recurrent sickness absence. Secondary outcome measures were mental health complaints, work functioning and coping behaviour.
Results 80 participants were randomised in the intervention group and 78 in the control group. The adjusted OR for the incidence of recurrent sickness absence was 0.40 (95% CI 0.20 to 0.81) and the adjusted HR for time to recurrent sickness absence was 0.53 (95% CI 0.33 to 0.86) for the intervention group compared with care as usual.
Conclusions This study demonstrates the 12-month effectiveness of a problem-solving intervention for reducing recurrent sickness absence in workers with CMDs and emphasises the importance of continuous attention in the post return to work phase for workers who have been on sickness absence due to CMDs.
Statistics from Altmetric.com
What this paper adds
-
Workers who returned to work after sickness absence due to common mental disorders (CMDs) frequently experience recurrent sickness absence.
-
No studies have been published on interventions to prevent recurrent sickness absence in workers with CMDs.
-
The present study showed that a problem-solving intervention for workers who returned to work after sickness absence due to CMDs was effective in reducing the incidence of recurrent sickness absence and increasing time to recurrent sickness absence compared with care as usual.
-
Occupational healthcare providers need to have continuous attention in the post-RTW phase for workers who have been on sickness absence due to CMDs.
Introduction
Common mental disorders (CMDs), such as depressive, anxiety and adjustment disorders, are an important contributor to the global burden of disease.1–4 Besides detrimental effects on the individual, CMDs have an enormous impact on society in terms of medical care consumption, work disability and associated costs.3 ,5–14 Moreover, reduced job performance persists after symptom reduction,15 ,16 and recurrent sickness absence is experienced frequently. Recent findings from the Netherlands and Finland showed that 20–30% of the workers who returned to work after sickness absence due to CMDs experience recurrent sickness absence. Additionally, the risk of sickness absence due to a CMD is higher in workers with previous sickness absence due to a CMD compared with a general worker population.17–19 Although several studies evaluated the effectiveness of cognitive behavioural and problem-solving interventions for facilitating return to work (RTW) of workers on sickness absence due to CMDs,20–25 little attention has been paid to the prevention of recurrent sickness absence. Recurrent sickness absence has a major health impact because it increases the risk of work disability in later years.19 ,26 Furthermore, recurrent sickness absence after an initial sickness absence episode due to CMDs is often more serious and long-lasting.17 Hence, interventions to prevent recurrent sickness absence in workers with CMDs after RTW to prevent recurrent sickness absence are of paramount importance.
To our knowledge, no interventions have been developed and evaluated that focus on the prevention of recurrent sickness absence in the post-RTW phase. This study aims to evaluate the effect of the Stimulating Healthy participation And Relapse Prevention at work (SHARP-at work) intervention, developed to prevent recurrent sickness absence in workers who returned to work after sickness absence due to CMDs. The intervention is based on the guideline ‘Management of mental health problems of workers by occupational physicians (OPs)’ of the Netherlands Society of Occupational Medicine. This evidence-based guideline, developed in 2000 and revised in 2007, facilitates RTW of workers on sickness absence due to mental health problems by OPs.20 ,27 ,28 According to the guideline, one relapse prevention consultation has to take place after RTW, but this is rarely done by OPs.29 The SHARP-at work intervention was developed to prevent recurrent sickness absence by structuring OP treatment after RTW. We hypothesise that compared with care as usual (CAU) the SHARP-at work intervention (1) prevents recurrent sickness absence, (2) reduces mental health complaints and (3) enhances work functioning and problem-solving coping.
Methods
Study setting and participants
The study was designed as a cluster-randomised controlled parallel-group trial (cluster-RCT). OPs, responsible for conducting the intervention, were recruited through 365/ArboNed, one of the largest Occupational Health Services (OHS) in the Netherlands. OPs were organised in group practices. Research participants were recruited by participating OPs. Inclusion criteria were: age 18–63 years; employed in a paid job; a diagnosis of a CMD given by their OP (based on International Classification of Diseases, version 10 (ICD-10)) at the start of the sickness absence period; an episode of sickness absence of at least 2 weeks; a planned RTW within 2 weeks (ie, the intervention could begin directly when a worker started RTW). Exclusion criteria were: a sickness absence episode >12 months; a prior sickness absence episode due to a CMD in the past 3 months; severe mental disorders, such as psychotic disorder or bipolar disorder; somatic complaints/disorders that would affect RTW; pregnancy, an upcoming retirement/resignation/lay-off; not able to read, write and understand Dutch. More detailed information can be found elsewhere.30 The Medical Ethical Board of the University Medical Center Groningen provided approval for the study design, the research protocol, questionnaires, information letters and the informed consent. Workers participated voluntarily in this study and signed an informed consent.
Interventions
SHARP-at work intervention
The intervention consisted of a five-step problem-solving process to find and implement solutions for problems experienced when back at work. Consultations between the worker and supervisor were included in this process as workers and healthcare professionals have stressed the importance of the supervisor during RTW.31 ,32 The problem-solving process comprised the following five steps:
-
Make an inventory of problems and/or opportunities encountered at work after RTW
-
Brainstorm about solutions
-
Write down solutions and the support needed and assess the applicability of these solutions
-
Discuss solutions and make an action plan with the supervisor
-
Evaluate the action plan/implementation of solutions
The OP started the intervention during the first 2 weeks of RTW, monitored that all steps were taken and activated and supported the worker if needed. The role of the OP was to counsel the worker on the process level; not to comment on the content of the problems or solutions of the worker. The OP empowered the worker to define his own problems and design his own solutions. Two to five OP consultations were recommended within 3 months after RTW, depending on the needs of the individual worker, with a minimum of two to conduct the intervention. The duration of an intervention consultation was 30 min which equals OP consultation time in the Netherlands. Five assignments were developed to facilitate the problem-solving process. The first assignment (ie, making an inventory of problems and opportunities and assessing the help needed to solve them) instigated the problem-solving process and was therefore a key element. More detailed information on the content of the intervention and the process evaluation has been described elsewhere (Arends et al, submitted).
OPs received a 2-day intervention training, provided by experienced trainers in occupational health interventions. Three feedback moments of 2 h were organised to jointly discuss the negative and positive aspects of conducting the intervention. As intervention OPs could work in the same group practice as OPs from the CAU group, intervention OPs were restricted to only talk about the intervention with each other and the feedback moments were also specifically developed to provide them with the opportunity to talk about their experiences with the intervention.
Care as usual
OPs were supposed to deliver CAU according to the guideline on ‘Management of mental health problems of workers by OPs’.27 This guideline does not contain a structured approach for preventing recurrent sickness absence (which is the focus, and thus the added value, of the SHARP-at work intervention). No specific attempts were made to ensure that the OPs followed the guideline and they received no information about the content of the SHARP-at work intervention.
Primary outcome measure
Recurrent sickness absence
Based on administrative OHS data, we measured recurrent sickness absence days and recurrent sickness absence incidence due to all causes at 3 months, 6 months and 12 months follow-up and time to first episode of recurrent sickness absence (measured in calendar days). Recurrent sickness absence was defined as ≥30% decrease in working hours per week due to sickness absence. No limits were set for the duration of the ≥30% decrease. When a worker increased again in number of working hours per week above the 30% threshold, this was recorded as the end of the recurrence episode. In the Netherlands, RTW is often a gradual process, that is, recurrent sickness absence can occur during the RTW process and not only after full RTW. Recurrent sickness absence days were corrected for part-time sickness absence by dividing the sickness absence days by 1/RTW percentage.
Secondary outcome measures
Mental health complaints
The Hospital Anxiety and Depression Scale was used to assess depression and anxiety (each seven items). The questionnaire has been validated for working populations33 and for the Dutch population.34 Each item is scored on a 4-point Likert scale indicating the extent to which an item was experienced in the past week.
The Four-Dimensional Symptom Questionnaire was used to assess symptoms of distress, depression, anxiety and somatisation. The 50-item Four-Dimensional Symptom Questionnaire has been validated in primary care and working populations35 ,36 and is scored on a 5-point Likert scale ranging from 1=no to 5=very often or continuous. Lower scores indicate lower symptom levels.
Work functioning
Work functioning was assessed with the Work Role Functioning Questionnaire, which has been cross-culturally adapted to the Dutch language and validated in the working population.37 ,38 The 27-item Work Role Functioning Questionnaire assesses perceived difficulties in meeting work demands given physical or emotional problems and is scored on a 5-point Likert scale from 100% (all of the time) to 0% (none of the time), with an option ‘not applicable’. Scores are converted to 0 and 100, with higher scores indicating better work functioning.
Coping behaviour
Coping behaviour was assessed with the 14-item version of the Utrecht Coping List.39 The questionnaire consists of three scales: (1) active problem focused coping, (2) emotional coping and (3) looking for distraction and decreasing tension. Each item is scored on a 4-point Likert scale ranging from 1=seldom or never to 4=very often. Lower scores indicate low usage of a certain coping behaviour.
Sample size
The sample size calculation was based on the outcome of recurrent sickness absence days. Recurrent sickness absence days of a first recurrent episode (after full RTW) within 1 year were extracted from the OHS sickness absence registry, including data of 4443 workers. The variance in recurrent sickness absence days at OP level (ie, the cluster design) was taken into account. The mean number of days of recurrent sickness absence was 68.5 days (SD=119.6). The target of the present study was to reduce recurrent sickness absence days with 20%, that is, an average of 12.7 days. We calculated that 25 OPs per group were needed, each providing five participants, in order to have 80% power to show a mean difference in decrease of 12.7 recurrent sickness absence days during 1 year, assuming an α of 0.05 and an intraclass correlation coefficient of 0.05.40
Randomisation
Randomisation took place at OP level, because workers could not be randomly assigned to OPs. A computerised random allocation sequence was developed by an independent statistician to randomise the OPs over the SHARP and the CAU groups. When all OPs were recruited, the independent researcher, who was blinded to the identity of the OPs, used the allocation sequence to randomise the OPs. After randomisation, the allocation of the OPs could not be changed and the statistician informed the researchers about OP allocation.
Blinding
In this prerandomised trial, the allocation of the workers followed the allocation of their OPs. Therefore, we were able to provide different information about the study to the intervention and control groups.41 Participants were blinded for study design and group comparison. Blinding OPs for allocation was not possible. An independent researcher at the OHS, blinded for study group, collected the administrative data on recurrent sickness absence days.
Statistical analyses
Baseline characteristics of the participants were compared to assess the success of randomisation. At each follow-up measurement, the number of workers with a recurrence and the median number of recurrent sickness absence days were calculated per study group. We predefined the following potential confounders based on previous research42–45: age, sex, educational level, mental health complaints and days of sickness absence at baseline. All outcome measures were assessed at baseline and at 3 months, 6 months and 12 months follow-up.
Primary outcome measures
Differences in number of recurrent sickness absence days between the two treatment groups were not analysed because of the skewed distribution; at each follow-up measurement, more than 50% of the study population had no recurrent sickness absence days. We examined the difference in incidence of recurrent sickness absence between the two treatment groups during follow-up with multilevel longitudinal regression analyses to account for the three-level design. Random intercepts were included for the OP-level as well as for the patient level (random slopes were not applicable due to randomisation at the OP-level). In addition, we analysed whether differences between the two groups in incidence of recurrent sickness absence varied over the three follow-up measurements (ie, were differences between the two groups bigger or smaller at 3 months, 6 months or 12 months follow-up or were differences similar at all follow-up measurements). Therefore, we included the interaction term ‘treatment group×time’ in the regression analysis. Crude analyses were followed by analyses adjusted for the predefined confounders.
Kaplan-Meier survival analyses were conducted to compare time to recurrent sickness absence in the two treatment groups. Participants were censored when lost to follow-up or when recurrent sickness absence had not occurred at the end of the 12 months follow-up period. The Cox proportional hazard model was used to estimate HRs. The proportional hazard assumption was tested.46 A separate model was run to adjust for the predefined confounders. No clustering effect was found in the multilevel logistic regression analyses, that is, we did not adjust for clustering in the Cox model.
Secondary outcome measures
To assess differences between the two treatment groups on mental health complaints, work functioning and coping behaviour, linear mixed models with unstructured covariance matrices were used.
Effect modification
We analysed modification of the group effects by size of company, decision latitude and readiness to stay at work. Company size was assessed with one single question and dichotomised to <100 workers versus >100 workers. Decision latitude was assessed with the Job Content Questionnaire.47 ,48 Items were scored on a 4-point Likert scale ranging from 1=totally disagree to 4=totally agree. Scores were divided into tertiles ranging from: 34–64, 65–72 and 73–92. Readiness to stay at work was assessed with the 6-item Readiness to Stay at Work Scale.49 Items were scored on a 5-point Likert scale, ranging from 1=totally disagree to 5=totally agree. Scores were divided at the 50% percentile to form two groups (10–20 vs 21–29). Subgroups were too small to conduct subgroup analyses on ICD-10 diagnosis, supervisor participation in the RTW process and type of occupation.
All analyses were performed according to the intention-to-treat principle using MLwiN, V.2.23 and SPSS, V.20.0.
Results
Between January 2010 and June 2011, OPs recruited 212 workers with a mean number of 1.4 (SD=2.3) workers per OP. Of these workers, 158 agreed to participate in the study. Recruitment fell short according to the sample size calculation. Reasons for the recruitment problems have been described extensively elsewhere.50 Workers who did not want to participate did not significantly differ from those who agreed to participate with regards to gender and age. The participant flow and reasons for non-participation are presented in figure 1. Of the 158 included participants, 80 participants were randomised to the SHARP group and 78 participants to the CAU group. Table 1 shows the baseline characteristics of the participants in both groups. Follow-up measurements ended in June 2012.
Worker characteristics per study group
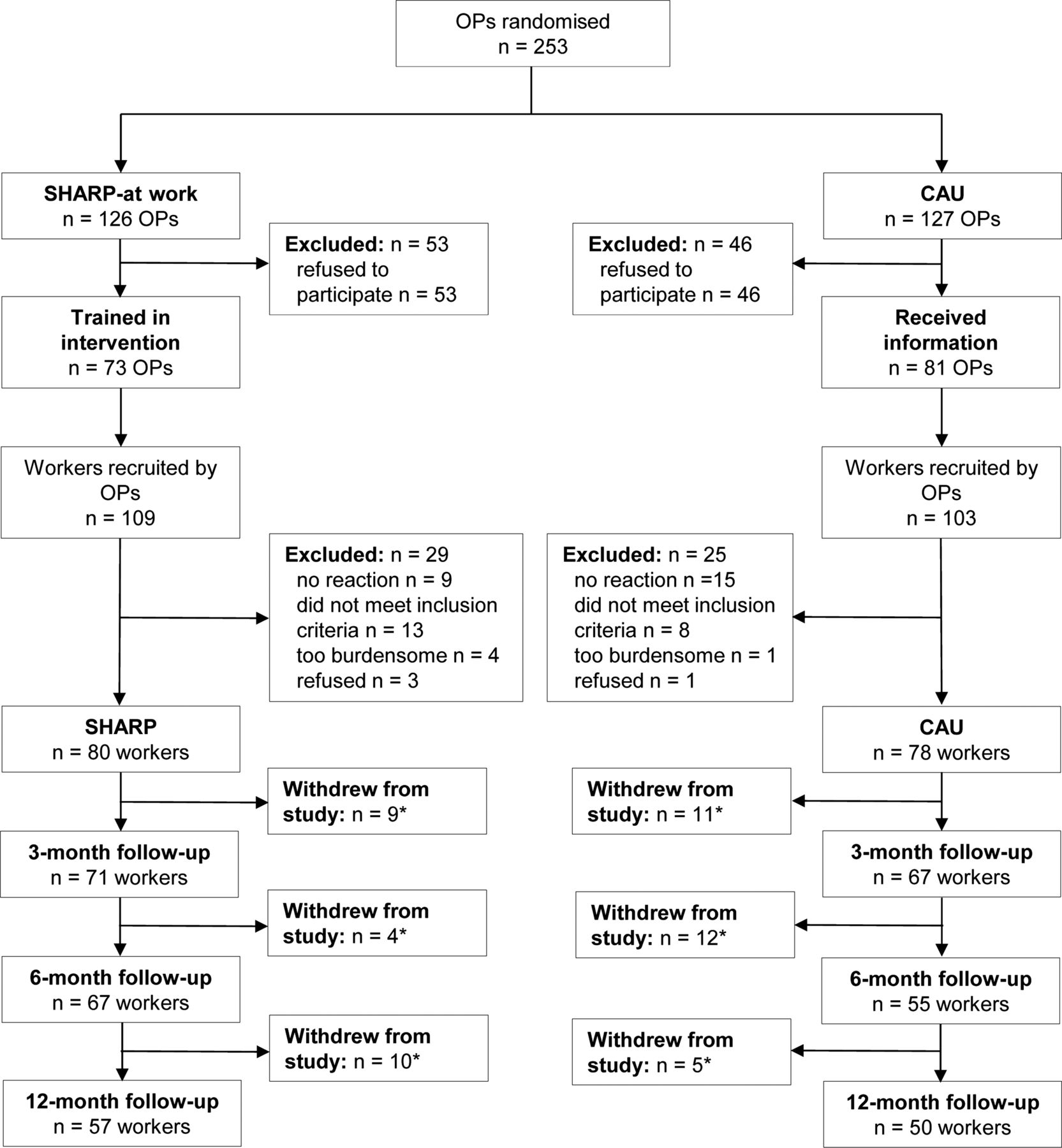
Flow chart of participant recruitment, allocation and outcome assessment. SHARP, intervention group; CAU, care as usual group; OP, occupational physician. *Reasons for withdrawal from the study for intervention group were: health problems (n=1), research too burdensome (n=2), a new OP (n=1), pregnancy (n=1), no time (n=2), job loss (n=2) or unknown (n=14). Reasons for the control group were: health problems (n=1), research too burdensome (n=1), job loss (n=2), refused (n=2), no time (n=2) or unknown (n=20). Numbers pertain to the secondary outcome measures.
Loss to follow-up
Administrative OHS data on recurrent sickness absence at 3 months, 6 months and 12 months follow-up and time to recurrent sickness absence were available for 147 participants (N=72 for the SHARP group and N=75 for the CAU group). For six participants, administrative data could not be retrieved. Furthermore, one participant who became pregnant and experienced pregnancy-related complaints and four participants who left the company during follow-up were censored. For the self-reported outcomes, 20 participants did not respond at 3 months follow-up, 36 participants at 6 months follow-up and 51 participants at 12 months follow-up. Reasons for non-response per study group are reported in figure 1. No significant differences were found between respondents and non-respondents for age, sex, educational level, mental health complaints and duration of sickness absence at baseline.
Non-compliance
At 3 months follow-up, 67 participants of the SHARP group completed a questionnaire on received intervention components. Of this group, 43 (64%) participants reported that they had two or more OP consultations and had made the first intervention assignment.
Co-interventions
In the intervention group, two participants (2.5%) reported that they visited a psychiatrist, 34 (42.5%) a psychologist (mean number of visits in a 4-week-period was 1.6) and one (1.3%) a social worker. Seven participants (9%) reported that they used psychopharmacological medication. In the control group, 9 participants (12%) reported that they visited a psychiatrist, 21 (27%) a psychologist (mean number of visits in a 4-week-period was 1.7) and 3 (3.8%) a social worker. Psychopharmacological medication was used by 15 participants (19%).
Recurrent sickness absence
Compared with CAU, the SHARP group had a lower incidence of recurrent sickness absence at all follow-up measurements. In both groups, the median number of recurrent sickness absence days was 0 at all follow-up measurements, but there were some differences between the 75th percentiles of both groups (table 2). The multilevel logistic regression analyses showed an adjusted OR for recurrent sickness absence of 0.40 (95% CI 0.20 to 0.81) for the SHARP group compared with CAU. Analysis of the interaction between group and time showed that the effect of the SHARP-at work intervention on recurrent sickness absence did not significantly differ at the three follow-up measurements. Notwithstanding the fact that we did not detect differences in the effect over time, we felt it was insightful to provide the treatment effects per time point in order to show how the effect developed over time in the sample (table 3). None of the subgroup analyses on company size, decision latitude and readiness to stay at work showed a significant interaction with treatment group on the incidence of recurrent sickness absence.
Number of workers with a recurrent sickness absence episode and duration of recurrence in the SHARP and CAU groups
Multilevel regression analyses of differences in incidence of recurrent sickness absence, mental health complaints, work functioning and coping behaviour between the SHARP-at work intervention and CAU
Time to recurrent sickness absence
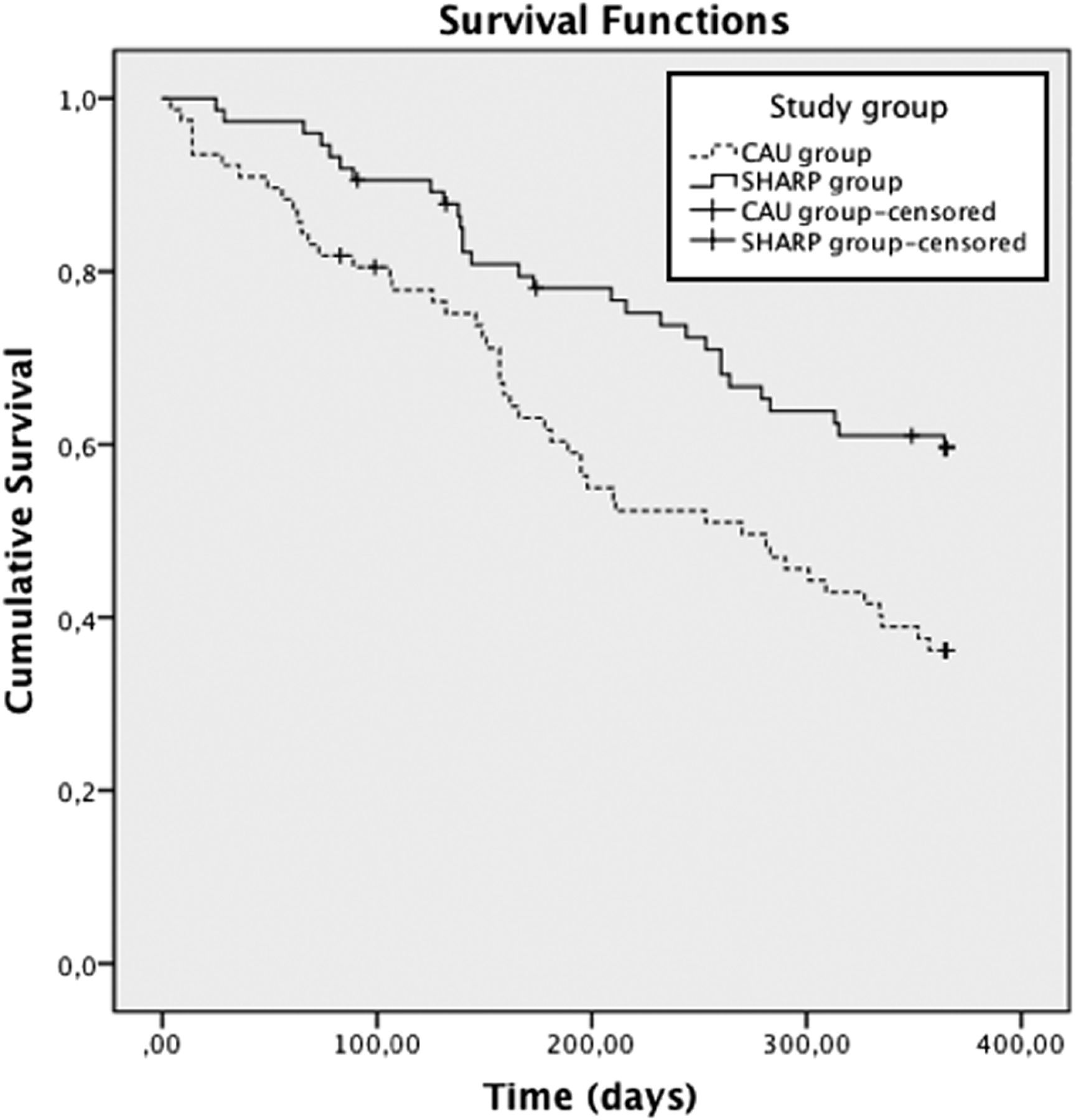
Figure 2 shows the cumulative survival curves of time to recurrent sickness absence for the SHARP and CAU group. Because the event was defined as first recurrent sickness absence, longer survival indicated a favourable outcome. The SHARP group had a median of 365 days (IQR 174–365) to recurrent sickness absence and the CAU group had a median of 253 days (IQR 117–365) (logrank test; p=0.003). When adjusted for confounders, time to recurrent sickness absence was significantly longer in the SHARP group compared with the CAU group (adjusted HR=0.53, 95% CI 0.33 to 0.86). No violation of the proportional hazards assumption was found based on three analyses of interactions between treatment group and dichotomised time variables. The three time variables were constructed using three different cut-off points based on time points in the survival plot that seemed to indicate a change in survival between the two groups (at 100 days, 150 days and 200 days).
{kind=link}
{kind=link}
Cumulative probability of recurrent sickness absence from baseline measurement to 12 months follow-up per study group. CAU, care as usual (n=76); SHARP, intervention group (n=74).
Mental health complaints, work functioning and coping behaviour
The effects of the intervention on mental health complaints, work functioning and coping behaviour are presented in table 3. Both groups improved on mental health complaints and work functioning. No clear differences were found between the two groups on mental health complaints at the follow-up measurements. The SHARP group reported a better score on work functioning at 12 months follow-up and a slightly higher usage of all three coping behaviours at all follow-up measurements. No significant group×time interaction was found for mental health complaints, work functioning and coping behaviour.
Discussion
Our primary aim was to evaluate the effectiveness of the SHARP-at work intervention in preventing recurrent sickness absence compared with CAU. At each follow-up measurement, the incidence of recurrent sickness absence was lower in the SHARP group compared with the CAU group. The longitudinal analyses showed that over 12 months follow-up the odds of recurrent sickness absence was 60% lower for the SHARP group compared with the CAU group. We found the strongest effect at 6 months follow-up, but this effect was not statistically different from the effect sizes at the other time points. Time to recurrent sickness absence was significantly longer in the SHARP group compared with the CAU group (median number of 112 days longer for the SHARP group). The expected effects on improved work functioning and problem-solving coping and reduced mental health complaints were not observed.
Currently, no other studies have been published on the effects of an intervention to prevent recurrent sickness absence in workers with CMDs. Van der Klink et al, evaluated an intervention primarily aimed at enhancing RTW in workers with adjustment disorders, and they also analysed the effect on recurrent sickness absence. The authors found no significant differences between the intervention and control groups on incidence of recurrent sickness absence and time to recurrent sickness absence.20 Although the SHARP-at work intervention is comparable with the intervention of van der Klink et al, the different results might be explained by the different timing of the interventions. Whereas the intervention of van der Klink et al took place at the start of and during the sickness absence period and focused on helping the worker to RTW, the SHARP-at work intervention was offered when a worker started RTW and focused on the prevention of recurrent sickness absence and helping the worker to stay at work.
To assess whether the observed effect on recurrent sickness is truly due to the intervention, a process evaluation has been conducted alongside the effect evaluation investigating treatment fidelity. The results of the process evaluation showed that the intervention was conducted as planned. Compared with the CAU group, participants in the SHARP group had significantly more often ≥two OP consultations, ≥one consultation with the supervisor and made more assignments (Arends et al, submitted for publication). Therefore, we conclude that the observed effect on recurrent sickness absence is due to the intervention. The SHARP-at work intervention could be used as an extension of the existing Dutch OP guideline, reinforcing the problem-solving process in the post-RTW phase and preventing recurrent sickness absence.
Our finding that the SHARP-at work intervention was not associated with significant reductions in mental health complaints compared with CAU, is corroborated by findings of several other studies on the effectiveness of different interventions (eg, cognitive behavioural treatment, problem-solving treatment and occupational therapy) to enhance RTW in workers with mental health problems.20–23 Thus, the effect on recurrent sickness absence cannot be explained through a mediating effect of better mental health. In the literature, explanations for the lack of effect on mental health complaints vary. It has been suggested that CAU is of such quality that a difference in symptom level is hard to achieve or that natural recovery may hinder the detection of treatment effects.21 Another explanation could be that the interventions are primarily aimed at improving social functioning and not the reduction of mental health complaints,21 as is the SHARP-at work intervention. Finally, participants might already have a higher level of mental health complaints before they develop a mental disorder (trait effect).51
Strengths and limitations
A strength of this study is the cluster-randomised design which allowed participant blinding. Participants knew that the study was aimed at investigating the treatment process after RTW but were unaware that groups were compared. Because participants were recruited by OPs that worked for companies of different sizes, in different sectors and in different parts of the Netherlands, our study population was quite diverse regarding type of occupation, company size and geographical location. This enhances the generalisability of our results.
A limitation concerns the low number of recruited participants according to the sample size calculation. The calculation was based on the outcome of recurrent sickness absence days, which we were not able to analyse due to a skewed distribution. However, we detected relevant differences between the SHARP and the CAU groups for the incidence of recurrent sickness absence and time to recurrent sickness absence. The distribution of baseline characteristics between the SHARP and the CAU groups showed some differences between the two groups regarding gender, educational level and sickness absence days. For ‘educational level’ this was probably due to certain selection mechanisms by OPs in the SHARP group. During feedback moments, OPs mentioned that it was easier to conduct the intervention with better educated workers. The baseline data showed that participants in the SHARP group had a higher educational level. All analyses were adjusted for baseline differences in educational level, sickness absence, gender, age and mental health complaints. However, some residual confounding might still have biased our results and the results might not be generalisable to workers with a low educational level. Although there was a difference between the two groups in diagnosis, the expected influence on the results is rather small. The diagnoses were made by OPs who are not specifically trained to differentiate between CMDs. Thus, the reported differences in diagnoses between the two groups may not be valid. This is also reflected in the scores on the subjective measures of CMDs where no differences between the groups were found. . Finally, we could not distinguish between different reasons for recurrent sickness absence because these were not consistently registered in the administrative OHS database.
Future research
Although the incidence of recurrent sickness absence was significantly lower in the SHARP group compared with the CAU group, the SHARP group showed a considerable incidence of recurrent sickness absence episodes at 6 months and 12 months follow-up (21% and 34%, respectively). Because the SHARP-at work intervention took place during the first 3 months following RTW, future research should investigate whether follow-up ‘booster’ treatment after 6 months might help to further reduce recurrent sickness absence and enhance mental health and work functioning. It is important to investigate the long-term effect of the intervention. Furthermore, an in-depth analysis of the specific characteristics of the workers who experience recurrent sickness absence, persistent mental health complaints and work functioning problems can help to focus the intervention on the needs of the most vulnerable workers. Although the SHARP and the CAU groups showed a reduction in mental health complaints, both still had relatively high scores on some of the mental health scales at 12 months follow-up. In addition, both groups showed improvements in work functioning over time, but after 12 months follow-up the mean score on work functioning was still lower compared with a healthy working population.38 Possibly, not being fully recovered from mental health complaints impedes optimal work functioning, which would explain why both groups still had suboptimal work functioning scores. Recently, Lerner et al52 found that a work-focused intervention for workers with depression, who were not on sickness absence, did decrease depression symptom severity and increase at-work performance. Future research needs to focus on how reductions in mental health complaints and improvements in work functioning can be accomplished for workers who have returned to work after sickness absence due to CMDs. Furthermore, research would benefit from including outcome measures related to social functioning, such as colleague/supervisor support.
Implications
The SHARP-at work intervention is effective in reducing the incidence of recurrent sickness absence for workers who returned to work after sickness absence due to CMDs. Our study shows that continuous attention is needed in the post-RTW phase for workers who have been on sickness absence due to CMDs. Before implementation in daily practice, the cost effectiveness and cost benefit of the intervention needs to be demonstrated.
Acknowledgments
The authors thank 365/ArboNed and the occupational physicians that participated in the study for their collaboration. Special thanks go out to Petra Koopmans, Johan de Bruin and Giny Norder for extracting the administrative data for the study. Also, we would like to acknowledge Benjamin C Amick III for providing comments on a previous version of this manuscript.
References
Footnotes
-
Trial registration number NTR1963.
-
Contributors IA, JJLvdK and UB designed the study; IA and WvR recruited the participants; IA and MRdB analysed the data; IA, JJLvdK, UB, MRdB and WvR interpreted the data; IA wrote the manuscript; JJLvdK, UB, MRdB and WvR commented on the manuscript and all authors approved the final manuscript. IA is the guarantor.
-
Funding The project was funded by ‘Stichting Instituut GAK’, a Dutch funding organisation (grant number 2007636). The authors were independent of the funder, and the funder had no role in the study design, data collection, analysis and interpretation of results or the writing of the report.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The Medical Ethical Board of the University Medical Center Groningen.
-
Provenance and peer review Not commissioned; externally peer reviewed.