Article Text

Abstract
Objectives Work-related asthma (WRA) is an important public health problem affecting one quarter of adults with asthma. Although cleaning substances are routinely used in hospitals, few studies have addressed their potential adverse respiratory health effects on healthcare professionals (HCPs). This study attempts to identify relationship between work-related exposure to cleaning-related chemicals and development of WRA among HCPs.
Methods Of 5600 HCPs surveyed, 3650 responded to a validated questionnaire about their occupation, asthma diagnosis, variability of asthma symptoms at and away from work, and exposure to individual cleaning substances. Workplace asthma was defined as a categorical variable with four mutually exclusive categories: work-related asthma symptoms (WRAS), work-exacerbated asthma (WEA), occupational asthma (OA) and none. Multivariable logistic regression analysis was used to evaluate the association between self-reported use of cleaning substances and asthma outcomes among HCPs.
Results Prevalences of WRAS, WEA and OA were 3.3%, 1.1% and 0.8%, respectively. The prevalence estimates were generally higher among female than male HCPs. The odds of WRAS and WEA increased in a dose-dependent manner for exposure in the longest job to cleaning agents and disinfectants/sterilants, respectively. For exposure in any job, the odds of WRAS were significantly elevated for both factor 1 (bleach, cleaners/abrasives, toilet cleaners, detergents and ammonia) and factor 2 (glutaraldehyde/ortho-phtaldehyde, chloramines and ethylene oxide). Significantly elevated odds of WEA were observed for exposure to bleach, factor 2 and formalin/formaldehyde. Exposure to chloramines was significantly associated with an almost fivefold elevated odds of OA.
Conclusions HCPs are at risk of developing WRA from exposure to cleaning substances.
- Occupational asthma
- work-exacerbated asthma
- work-related asthma
- healthcare professionals
- chemical substances
- occupational exposures
- epidemiology
- asthma
- occupational asthma
Statistics from Altmetric.com
- Occupational asthma
- work-exacerbated asthma
- work-related asthma
- healthcare professionals
- chemical substances
- occupational exposures
- epidemiology
- asthma
- occupational asthma
What this paper adds
Approximately one quarter of all cases of adult asthma in the USA and Europe are work related.
Women make up almost half of the US workforce and greatly outnumber men in health-related occupations, placing them at higher risk of exposure to cleaning-related substances.
Prevalences of work-related asthma symptoms, work-exacerbated asthma and occupational asthma were higher among female healthcare professionals.
Workplace exposures to cleaning-related chemicals were associated with the development of work-related asthma symptoms, work-exacerbated asthma and/or occupational asthma among healthcare professionals.
Introduction
A consensus panel of the American College of Chest Physicians recently defined work-related asthma (WRA) as “asthma that is exacerbated or induced by inhalation exposures in the workplace”.1 Based on this definition, WRA can be further subclassified into two, frequently overlapping, categories: (1) work-exacerbated asthma (WEA) which refers to exacerbation of existing asthma due to workplace exposures, and (2) occupational asthma (OA) which refers to new-onset asthma induced by workplace exposures.1 Up to one quarter of adults with asthma in the USA2 3 and in Europe4 have WRA. The list of respiratory sensitisers and irritants that are linked to asthma and OA has grown steadily over the past decade.1
According to the US Bureau of Labor Statistics, in 2008, the healthcare industry employed more than 14 million workers in the USA5 and this number is projected to grow by 22% through 2016. In the USA, the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) sets performance and infection control standards for healthcare organisations, including hospitals and nursing homes. To comply with these standards, hospitals should have strict procedures in place for maintaining general cleanliness, sterilising medical equipment and handling chemical spills, all of which require extensive use of cleaning chemicals. Cleaning substances commonly used in hospitals include, but are not limited to, acetic acid, ammonia, quaternary ammonium compounds, bleach, glutaraldehyde and ortho-phthalaldehyde (OPA).6 Many of these cleaning chemicals are highly volatile and frequent exposure may pose a respiratory health risk in certain occupational groups, including healthcare professionals (HCPs). With the exception of short-term high level chemical exposures due to accidental spills, which may result in inhalational injury to the lungs, adverse respiratory health effects such as WRA due to recurring exposure to lower levels of cleaning chemicals are less likely to be recognised.
Previous studies which have identified HCPs as an at-risk population for developing or exacerbated asthma often define their respiratory outcomes based on self-reported asthma attack,7 physician diagnosis8 or in combination with response to non-specific bronchial challenge testing.4 In an earlier report6 on the same population as in the current study, we defined asthma outcomes based on self-reported physician diagnosed asthma and an eight-item bronchial hyper-responsiveness-related symptom predictor. This limited its usefulness for describing work-related aspects of asthma as these definitions do not include information on how asthma symptoms vary at and away from work, an important characteristic of WRA.
This current study differs from our earlier analysis6 in two important aspects. First, in contrast to our previous work, in this study we have exclusively focused on exposure to cleaning-related substances, which are defined in two different ways: self-reported frequency of exposure to groups of cleaning agents and disinfectants in the longest held job and self-reported exposure to individual cleaning chemicals. Second, using information collected on the variability of work-related asthma symptoms (WRAS) and keeping in mind clinical relevance, we constructed a working definition of asthma in the workplace with four mutually exclusive categories: WRAS, WEA, OA and none. Hence, this study sought to address two questions: (1) ‘What is the prevalence of WRAS, WEA and OA in a healthcare population?’ and (2) ‘Is there an association between self-reported exposures to cleaning chemicals and WRAS, WEA and OA outcomes?’.
Methods
In 2004, we conducted a large population-based survey of 5600 licensed HCPs in Texas. A detailed description of the survey has been provided elsewhere.9 Briefly, a sample of 5600 HCPs which included physicians (n=1400), nurses (n=1400), respiratory therapists (n=1400) and occupational therapists (n=1400) with active Texas licences in 2003 were surveyed using a validated questionnaire. A total of 3650 questionnaires were received for an overall response rate of 66%.9 To ensure the study sample was representative of the actual population of licensed HCPs, which included a disproportionately large number of nurses and physicians, post-stratification weights were constructed.
Dependent variables
A single dependent variable with four mutually exclusive categories (WRAS, WEA, OA and none) was defined for this study. First, the work-relatedness of asthma was determined based on responses to the following questions:
Have you had wheezing or whistling in your chest while you were at work at any time in the last 12 months? If yes:
While you were away from work at any time in the last 12 months, was your wheezing or whistling: better, worse, no change?
After returning to your work at any time in the last 12 months, was your wheezing or whistling: better, worse, no change?
Have you had an attack/episode of shortness of breath while you were at work at any time in the last 12 months? If yes:
While you were away from work at any time in the last 12 months, was your shortness of breath: better, worse, no change?
After returning to your work at any time in the last 12 months, was your shortness of breath: better, worse, no change?
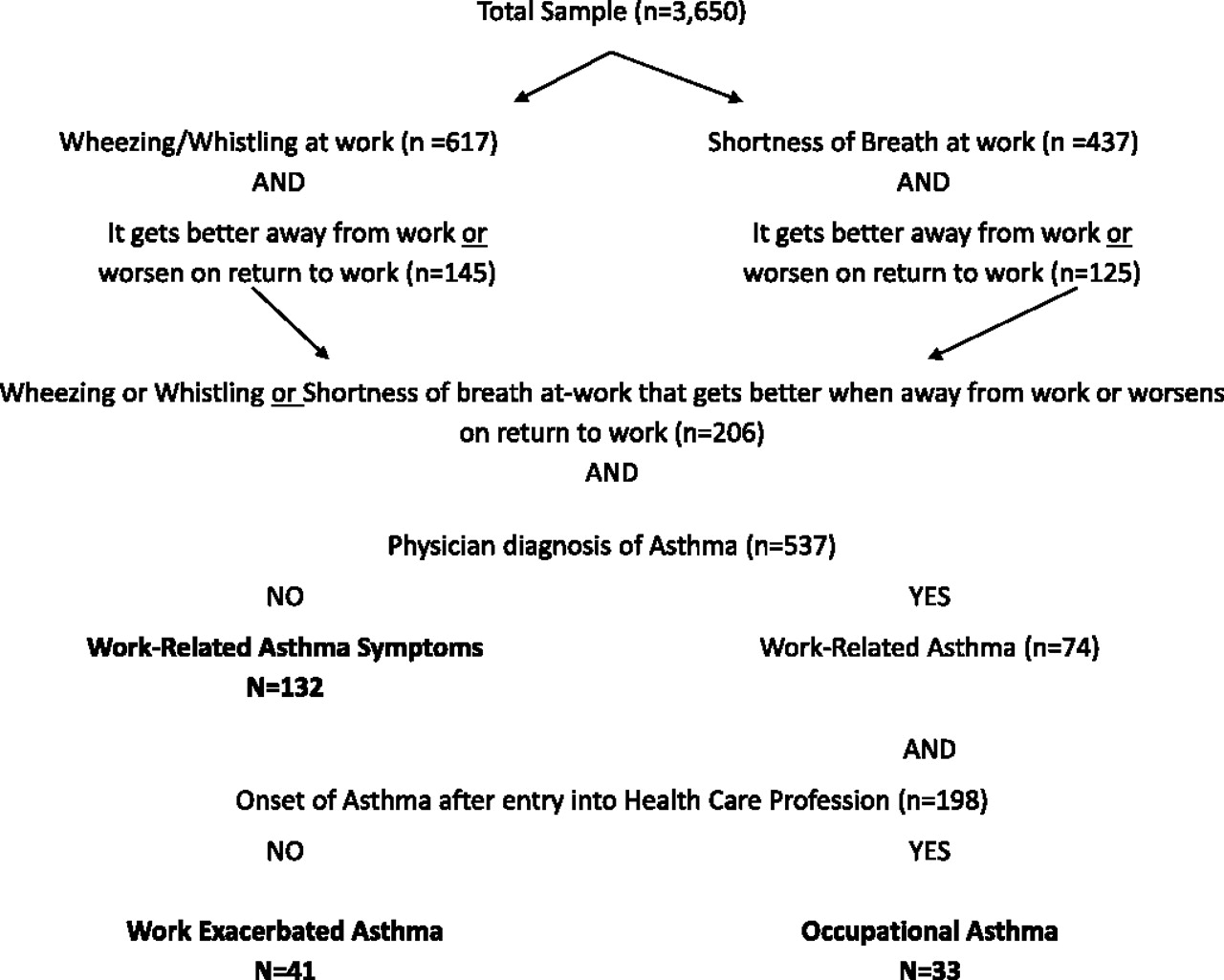
Those with asthma symptoms who also had a history of physician-diagnosed asthma were considered to have WRA and those without a history of physician-diagnosed asthma were considered to have WRAS (n=132). Within the WRA group, those whose asthma had developed after beginning work as a HCP were classified as having OA (n=33) and those whose asthma had not developed after beginning work as a HCP were considered to have WEA (n=41) (figure 1). Respondents with none of the outcomes present were coded as a reference group (n=3440). There were four respondents whose outcome status was not determined. Development of asthma after entry into a healthcare profession was determined by comparing the age at which a physician made the asthma diagnosis with the number of years spent in the healthcare profession.6
{kind=link}
Case definitions and sample selection flow chart.
Independent variables
The main exposures of interest were cleaning-related chemicals, defined in two different ways.
Self-reported exposures in the longest held job
A detailed history of the job held longest by the study participant was collected using the questionnaire. Each participant was asked: ‘While working at this job, indicate how often, on average, you handled or were exposed to any of the following products: (1) cleaning agents and (2) disinfectants/sterilants’. The responses were coded as never/once a month=0, at least once a week=1, more than once a day=2 and every day=3. For 2049 participants, their current/most recent job was also their longest held job.
Self-reported exposures in any job
In addition to self-reported exposures during the longest held job, a global question related to at-work exposure to any of a list of 28 chemicals or allergens was also asked: ‘Think about all of the jobs you have ever had. To the best of your knowledge have you ever been in contact with any of the following materials at least once a month for a period of 6 months or longer? (yes/no)’. Twelve of these materials were cleaning-related chemicals and were included in this analysis. Glutaraldehyde and OPA were later combined and a total of 11 cleaning-related chemicals were reduced to two factors using common factor analysis. These two factors were conveniently labelled as: (1) ‘general purpose cleaning’ (bleach, room cleaners, cleaners/abrasives, cleaners for restrooms and toilets, detergents, disinfectants and ammonia) and (2) ‘instrument cleaning/sterilisation’ (glutaraldehyde/OPA, formalin/formaldehyde, chloramines and ethylene oxide). Table 1 shows the factor loadings, after varimax rotation, for the individual cleaning-related chemicals. Cronbach's α coefficients, a measure of internal consistency, for the two constructs were 0.86 and 0.63, respectively. Factor scores were then generated by summing individual variables and coding the scores ranging from 0.5 to 1 as 1 (exposed) and <0.5 as 0 (unexposed). In addition, to explore dose–response relationships, a summary measure of cumulative exposure was generated by adding all the individual variables and categorising the summary variable into 0–2, 3–5 and 6 or more exposures.
Factor analysis of self-reported exposure to individual chemical substances in any job
Other covariates
In addition to the main exposure variables of interest, information on potential confounders such as age, sex, race/ethnicity, body mass index (BMI), seniority (number of years as a HCP), atopy and smoking status were also collected.
Age and seniority variables were categorised into quartiles. The variable race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, other) was constructed using responses from two separate questions related to race (white, black, Asian, American Indian/Alaska native, other race) and ethnicity (not Spanish/Hispanic/Latino, Mexican, Mexican American, Chicano, Puerto Rican, Cuban, other Spanish/Hispanic/Latino). There were 47 white, 24 black, 21 Asian and 1 other race respondents who did not select their ethnicity. They were assigned to the non-Hispanic white, non-Hispanic black and other categories. BMI was defined as weight in kg/height in m2 and categorised as normal (BMI<25.0), overweight (BMI 25.0–29.9) or obese (BMI 30 and above). Atopy was defined by comparing self-reported responses to questions on allergies and dust to IgE and RAST panel serum titres, as described in our earlier validation study.9 Lastly, respondents' smoking status was classified based on the responses on two questions: ‘Have you smoked at least 100 cigarettes during your life?’ and ‘Do you smoke cigarettes now?’ into non-smoker, current smoker and ex-smoker.
Statistical analysis
Weighted prevalence analyses of WRAS, WEA and OA were performed. The OR and 95% CIs were computed using univariable and multivariable multinomial logistic regression analyses. Multinomial logistic regression analysis is used when the outcome variable has more than two discrete categories. In this study, the outcome variable had four mutually exclusive categories: WRAS, WEA, OA and none. Each of the three outcomes, WRAS, WEA and OA were simultaneously compared to the common baseline/reference category (none) using a multinomial logistic regression model, adjusted for age, sex, race/ethnicity, BMI, seniority, atopy and smoking status. All analyses were conducted using Stata Statistical Software Package v 11.0. The study was approved by the Committee for the Protection of Human Subjects of The University of Texas Health Science Center at Houston, Texas. Each participant provided informed consent before they took part in the study.
Results
The average age of the study population was 45.3 years (SD 11.9 years) and the majority were female. The prevalences of WRAS, WEA and OA were 3.3%, 1.1% and 0.8%, respectively. Female HCPs, on average, had a higher prevalence of WRAS (3.6% vs 1.8%), WEA (1.3% vs 0.3%) and OA (1.0% vs 0.1%) as compared to men (table 2). The overall prevalence of atopy was 14.7%. Over half the study population was overweight or obese. The prevalence estimates of the other covariates are presented in table 2.
Characteristics of the study population and prevalence (%) estimates of work-related asthma symptoms, work-exacerbated asthma and occupational asthma in health care professionals
Self-reported exposures in the longest held job
The odds of WRAS, adjusted for the potential confounding effects of age, sex, race/ethnicity, BMI, seniority, atopy and smoking status, increased in a dose-dependent manner from 2.64 (95% CI 0.57 to 12.14) for once a week exposure to cleaning agents in the longest held job to 5.37 (95% CI 1.43 to 20.16) for more than once a day exposure (p value for trend <0.001; table 3). For exposures to disinfectants/sterilants, the odds of WEA increased from 3.75 to 5.06 to 9.02 for at least once a week, every day and more than once a day, respectively (p value for trend =0.007; table 3). The odds of OA were substantially reduced for exposure to both groups of cleaning substances; however, they were significant for the once a week exposure category (table 3).
Prevalence (%) estimates of exposures and multinomial logistic regression analysis of association between exposure indices and work-related asthma symptoms, work-exacerbated asthma and occupational asthma
Self-reported exposures in any job held for 6 months or longer
The odds of WRAS were 3.93 (95% CI 1.66 to 9.32) and 2.14 (95% CI 1.06 to 4.32) times higher for the self-reported general purpose cleaning (factor 1) and instrument cleaning exposure constructs (factor 2), respectively. For exposure to individual cleaning substances, the OR ranged from as low as 1.48 (95% CI 0.71 to 3.07) for formalin/formaldehyde to as high as 4.60 (95% CI 2.12 to 9.95) for restroom/toilet cleaners, with eight of the 11 individual chemicals showing significant associations with WRAS (table 3).
We found significantly elevated odds of WEA for exposure to bleach (AOR 3.13, 95% CI 1.08 to 9.08), formalin/formaldehyde (AOR 2.66, 95% CI 1.03 to 6.86) and the factor 2 construct (AOR 3.40, 95% CI 1.35 to 8.53). The odds of OA were almost fivefold elevated for chloramines (AOR 4.81, 95% CI 1.28 to 18.06).
Discussion
This study found that at-work exposure to cleaning-related substances is associated with WRAS, WEA and OA among HCPs. Across the three outcomes, the associations were especially pronounced for exposures related to general purpose cleaning substances, including bleach, detergents, disinfectants and ammonia, and instrument cleaning substances such as glutaraldehyde/ortho-phthalaldehyde, formalin/formaldehyde and chloramines.
Cleaning-related chemicals, disinfectants and sterilants are widely used in healthcare settings.10 Medical and surgical equipment (such as endoscopes) are usually thoroughly cleaned first with detergents followed by disinfection or sterilisation. Therefore, the potential for workplace exposure to multiple chemicals is high for healthcare workers who routinely perform these tasks.
Aldehydes are a group of organic compounds containing a carbonyl group. In this study we found a twofold elevated odds of WRAS for self-reported exposure to glutaraldehyde/OPA. Glutaraldehyde, a colourless high level disinfectant and a chemical sterilant, is used in healthcare facilities to disinfect and sterilise a wide variety of heat sensitive instruments such as surgical and dialysis equipment, endoscopes and bronchoscopes, as well as in chemical film developing solutions.11 It is widely used in healthcare facilities, although some facilities have switched to using OPA instead. Exposure to glutaraldehyde has been linked to asthma and other respiratory symptoms among HCPs in several previous studies.8 12–15 High level exposure to glutaraldehyde via inhalation or skin contact can occur when a glutaraldehyde solution is activated or when equipment is processed manually in open vats under poor ventilation conditions.10 The Occupational Safety and Health Administration (OSHA) has not established a permissible exposure limit for glutaraldehyde exposure; however, the Centers for Disease Control and Prevention suggest taking action if the level is higher than 0.05 ppm, the ceiling limit established by the American Conference of Governmental Industrial Hygienists.16 Waters et al17 reported glutaraldehyde exposures of up to 0.15 ppm among nurses engaged in endoscopy disinfection. The authors reported a significant mean reduction of 30 ml and 50 ml in cross-shift forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC), respectively in the exposed group. Similarly, in a cross-sectional study of Australian nurses working in endoscopy units, Pisaniello et al18 reported glutaraldehyde exposure levels decreasing from 0.093 ppm to 0.022 ppm when a ventilation system was installed in an endoscopy unit. Because of the increasing evidence for the adverse respiratory effects of glutaraldehyde, OPA has been introduced into hospitals as a less toxic alternative to glutaraldehyde. Although we asked about exposure to glutaraldehyde and OPA separately, we opted to combine both in our analysis since it is easy to confuse them as both chemicals have similar trade names and during our 2003 walk-through surveys9 of hospitals we found both to be regularly present.
Exposure to formaldehyde, an indoor air contaminant, has been linked to asthma and asthma-like symptoms in several occupational and non-occupational studies.15 19–23 Formalin is used in hospitals for disinfection purposes as well as to fix, stain and preserve tissue. Healthcare workers may be exposed to formaldehyde volatiles while preparing formalin solutions, processing tissue specimens and disinfecting haemodialysis machines. OSHA considers it a carcinogen and has set an 8 h time-weighted average exposure concentration of 0.75 ppm and a short-term exposure limit of 2 ppm during a 15 min time period.24 Appropriate ventilation conditions and good workplace practices including appropriate use of personal protective equipment and chemical substitution where possible, can help reduce exposure to glutaraldehyde and formaldehyde and improve the safety of HCPs.
Bleach (sodium hypochlorite), chloramines and other chlorine-based products are commonly used as disinfectants to clean medical instruments, water supply, floors and other surfaces in hospitals.10 In this study exposure to bleach was independently and significantly associated with WRAS and WEA. A similar magnitude of association was observed with OA, but the results were statistically not significant. Chloramines are highly stable compounds and do not dissipate easily. Several case reports have reported chloramine-induced OA or asthma-like inflammation in nurses,25 26 dental personnel27 and indoor swimming pool cleaners.28 29 However, to our knowledge this is the first population-based workplace study that has shown this association in healthcare workers. Similarly, bleach has also been linked to asthma and asthma-like symptoms in earlier studies.7 30 31 In a case–control study of Spanish female domestic cleaning workers, a fivefold increase in the odds of work-related respiratory symptoms was observed among those exposed to bleach.30 In a panel study of 43 female domestic cleaners, the same authors reported a more than threefold increased odds of lower respiratory symptoms (OR 3.5, 95% CI 1.4 to 8.5) among cleaners exposed to bleach.31 Shakeri et al32 in their systematic review identified chlorine as the most common agent linked to reactive airways dysfunction syndrome (RADS). In a large population-based international study, based on the European Community Respiratory Health Survey (ECRHS), nurses who reported using bleach or ammonia were found to have an elevated risk of new-onset asthma (RR 2.16, 95% CI 1.03 to 4.53).7 Results from our study provide further support for the likely adverse role of chlorine-based chemicals in the development of WRA.
Self-reported use of ammonia was significantly associated with WRAS only in this study. Ammonia, a colourless gas with a distinct odour, is a strong respiratory irritant and when dissolved in water is commonly used for general purpose cleaning. Acute exposure to ammonia can lead to severe upper respiratory symptoms and RADS, whereas chronic exposure to ammonia has been linked to the development of asthma. Using data from the Sentinel Event Notification System for Occupational Risks (SENSOR), Rosenman et al33 linked 14 cases of WRA among janitors and cleaners to work-related exposure to ammonia. Similarly, the prevalence ratio for asthma was 3.4 times higher among Spanish indoor cleaners reportedly exposed to ammonia (PR 3.4, 95% CI 1.9 to 5.9).34
This is one of the largest population-based studies to report adverse respiratory health effects among healthcare workers using cleaning-related chemicals. However, certain study limitations should be noted. We used self-reported exposure to cleaning groups in the longest held occupation and to individual cleaning agents in any job to characterise workplace exposures. In our earlier study,35 using job-exposure matrix-based exposure indices, we found differences in sensitivity, specificity and agreement among those with and without asthma for exposures with odours, suggesting some differential misclassification bias. Longest held occupation better reflects a worker's cumulative exposure experience. It is possible that HCPs who experience severe asthma symptoms early in their job or notice exacerbation of their existing asthma may change jobs, with the result that there is a lower prevalence of WEA and OA, as observed in this study. This was further evident from the fact that the prevalence of WRAS, WEA and OA decreased in the highest quartile of seniority (data not shown), suggesting that some workers may have left the workforce because of respiratory health issues. This healthy worker survivor effect can result in selection bias that is difficult to correct in cross-sectional epidemiological studies. Although it would be ideal to have had personal level exposure data for each individual study participant, to minimise exposure misclassification, personal sampling is not generally feasible in large population-based studies. Finally, the low prevalence of OA among HCPs affected our ability to estimate the odds ratio of association for certain exposures with precision, as evident by the wide confidence intervals in some instances. The significantly lower odds of OA observed for using cleaning substances at least once a week in the longest held job could be an artefact due to the small number of observations or it could reflect the healthy worker survivor effect. The cross-sectional nature of the study precludes us from making any conclusions regarding the temporal relationship between the cleaning-related exposures and workplace asthma outcomes.
Most hospitals in the US are accredited by JCAHO and are required to use appropriate disinfection and sterilisation procedures to prevent infection and maintain the health and safety of both patients and staff. There are guidelines in place on safe use of these otherwise very effective cleaning products.10 But, despite this, the increased occurrence and reporting of work-related asthma and asthma symptoms among healthcare workers exposed to cleaning-related chemicals remains a concern.
Future studies should consider incorporating quantitative measurements into their exposure assessments, and identify processes that could lead to high workplace exposures. Also, individual behaviours and attitudes towards workplace safety and the use of personal protective equipment should be explored. Furthermore, due to widespread non-occupational use of cleaning substances, especially in homes, the potential health implications of this use in the general public should be studied.
References
Footnotes
Funding This work was supported in part by grant nos. 5R01OH03945-01A1 and T42CCT610417 from the National Institute for Occupational Safety and Health/Centers for Disease Control and Prevention.
Competing interests None.
Ethics approval This study was conducted with the approval of the University of Texas at Houston, School of Public Health, Houston, Texas.
Provenance and peer review Not commissioned; externally peer reviewed.