Article Text

Abstract
Background Population-based data are paramount to investigate the long-term course of diabetes, for planning in healthcare and to evaluate the cost-effectiveness of primary prevention. We analysed regional differences in the incidence of self-reported type 2 diabetes mellitus in Germany.
Methods Data of participants (baseline age 45–74 years) from five regional population-based studies conducted between 1997 and 2010 were included (mean follow-up 2.2–7.1 years). The incidence of self-reported type 2 diabetes mellitus at follow-up was compared. The incidence rates per 1000 person-years (95% CI) and the cumulative incidence (95% CI) from regional studies were directly standardised to the German population (31 December 2007) and weighted by inverse probability weights for losses to follow-up.
Results Of 8787 participants, 521 (5.9%) developed type 2 diabetes mellitus corresponding to an incidence rate of 11.8/1000 person-years (95% CI 10.8 to 12.9). The regional incidence was highest in the East and lowest in the South of Germany with 16.9 (95% CI 13.3 to 21.8) vs 9.3 (95% CI 7.4 to 11.1)/1000 person-years, respectively. The incidence increased with age and was higher in men than in women.
Conclusions The incidence of self-reported type 2 diabetes mellitus shows regional differences within Germany. Prevention measures need to consider sex-specific differences and probably can be more efficiently introduced toward those regions in need.
- Epidemiology of diabetes
- Cohort studies
- GEOGRAPHY
- Epidemiological methods
Statistics from Altmetric.com
Introduction
Epidemiological data on the incidence of type 2 diabetes mellitus (T2DM) on a regional level are scarce in Germany as well as in other countries. For Germany, one study based on patient data from a large German statutory health insurance (Techniker Krankenkasse) showed an incidence rate of 1.4/1000 person-years for the age group 45–49 years up to 8.6 per 1000 person-years for the age group 70–74 but was not stratified by regions.1 Another population-based study the Cooperative Health Research in the Region of Augsburg (KORA) conducted in the South of Germany showed a standardised incidence rate of 15.5/1000 person-years for individuals aged 55–74 years, which was among the highest in Europe (based on validated physicians’ diagnosis or an oral glucose tolerance test).2 Of note, this study region in the South demonstrated the lowest standardised prevalence estimate for self-reported T2DM with 5.8% compared to other regions in Germany.3 The highest prevalence was observed in the East and Northeast which was almost twice as high as in the South. Thus, it remained unclear, whether the regional incidence estimates from KORA are representative for other regions of Germany or whether regional differences in incidence might explain the regional pattern we found for the self-reported prevalence of type 2 diabetes.3
The pattern of regional differences in the prevalence of T2DM is in accordance with regional differences in risk factors for T2DM such as obesity. In the USA,4 the regional prevalence of T2DM is mainly linked to the regional obesity prevalence, similar to Germany.5–7 Historically, in Germany after the reunification in 1989, there existed between East and West considerable differences in healthcare which have been assimilated in the past 20 years.8 However, there are still remaining differences which are probably related to risk factors for T2DM.
Prevalence data are important to explore the current needs of regional healthcare. Incidence data are needed to assess the prognosis of newly diagnosed cases by practices of treating physicians, to identify high-risk groups to face the challenge of changing modifiable risk factors, and to plan future healthcare allocations. Regional differences in T2DM incidence was examined in the USA in the youth (10–19 years) based on clinical information.9 Further incidence differences for clinically diagnosed T2DM in rural and metropolitan areas were examined in China.10 As for other European countries for Germany data on possible regional differences in the incidence of the T2DM is missing.
The aim of our study is to provide population-based estimates for the incidence of self-reported T2DM on a regional level within Germany. Data originate from five population-based cohort studies that used comparable methods in individuals aged 45–74 years at baseline within the Diabetes Collaborative Research of Epidemiologic Studies (DIAB-CORE) consortium in Germany.
Materials and methods
Study population
For this current analyses based on pooled individual data and stratified by study, we included follow-up data from five regional population-based cohort studies carried out in Germany (table 1): Northeast: the Study of Health in Pomerania (SHIP), Mecklenburg West Pomerania; East: the Cardiovascular Disease, Living and Ageing in Halle Study (CARLA) in the city of Halle (Saale), Saxony-Anhalt; West: the Dortmund Health Survey (DHS) in the city of Dortmund, North Rhine-Westphalia and the Heinz Nixdorf Recall Study (HNR) in the cities of Essen, Bochum and Mülheim of the Ruhr-Area, North Rhine-Westphalia; South: the Cooperative Health Research in the Region of Augsburg (KORA) study, city of Augsburg and municipalities in surrounding rural districts, Bavaria. Data collection for baseline studies was performed between 1997 and 2006 and for follow-up examinations between 2002 and 2010 (table 1). The mean follow-up duration varied between 2.2 and 7.1 years (table 1). Data of the DIAB-CORE studies used herein are similar regarding study design (population-based sampling), selection of study population (two-stage cluster sampling, stratified random sampling), response rates (61–69%) and measurement methods, mainly derived from the German National Health Interview and Examination Survey 1998 (DHS, West; HNR, West) and from the Multinational MONItoring of trends and determinants in CArdiovascular disease (MONICA) project (CARLA, East; KORA, South; SHIP, Northeast).3 Specific study details have been described elsewhere.11–15 All studies were approved by local ethics committees and public data protection agencies. Informed written consent was obtained from all participants. All studies were monitored by review boards of independent scientists.
Baseline and follow-up characteristics by studies in the Diabetes Collaborative Research of Epidemiologic Studies (DIAB-CORE)
To enhance comparability of studies, only the age group 45–74 years at baseline was included. From 11 688 participants (5832 women), individuals who did not participate in the follow-up studies (n=2015), with self-reported T2DM at baseline (n=731), missing data in drop out weights (n=52) or in self-reported diabetes status at follow-up (n=101) were excluded. A total of 8787 participants (4484 women) were eligible for the present analyses. The exclusion criteria for each study are represented in table 2.
Exclusion criteria from baseline to follow-up by study
Measurement
A history of self-reported diabetes mellitus, sociodemographic information, and data on health-related behaviour was assessed by standardised face–t- face computer-assisted personal interviews. Body mass index was calculated as body weight divided by body height squared (kg/m2) which was assessed by measurement. Smoking status was assessed (never/former/current smoker). Different types of alcohol (g/d) including wine, beer and liquor and their amount was assessed for an average week. Education was categorised into three sections according to the German school system (low, <10 years/intermediate, 10 years/high, >10 years). Information on the monthly household per capita net income was collected (<600/600–900/>900–1200/>€1200). We applied a commonly adopted procedure to divide the household income by the square root of the number of household members, thus assuming an equivalence parameter of 0.5.16
Ascertainment of incident T2DM
In all studies, incident T2DM was defined based on self-reported physicians’ diagnosis within the follow-up period. The KORA study (South) was the only study where—in a subsample of participants aged 55–74 years—an oral glucose tolerance test was performed at baseline in participants without a self-reported T2DM.2 Owing to the fact that this baseline study uncovered a high prevalence of yet unknown T2DM in the South German population, the results of the oral glucose tolerance test may have led to a subsequent physicians’ diagnosis which influenced the estimates of self-reported T2DM at follow-up. In our analyses we did not further differentiate whether self-reported incident T2DM was validated by physicians directly following the result of an abnormal oral glucose tolerance test at baseline or if it was diagnosed independently from the baseline investigation during follow-up.
Statistical analyses
Characteristics of the study population are reported as the median (25th, 75th centile) for continuous variables and as percentages for categorical variables. All incidence calculations were weighted multiplicatively for poststratification according to the German adult population (reference date 31 December 2007)17 and for loss to follow-up in each study.18 The assumption for using drop out weights is that the missing mechanism is at random meaning that missingness can be explained by the available data. For derivation of the non-response weights we have run a logistic regression model for participation at follow-up (1 if participant attended at follow-up; 0 if not) with baseline variables as independent variables (age, sex, smoking status, physical activity, education, equivalent income, alcohol consumption and body mass index). From this regression model we calculated the probability to participate at follow-up and took the inverse of this as drop out weight. Since drop out mechanisms may vary across studies, we calculated non-response weights for each study separately.
We checked the final weights for outliers and did not detect any extreme values. Therefore, we did not trim the weights. We did not consider base weights, which are used to account for different sampling probabilities of individuals into a study, since these weights were not available in all studies. In SHIP we did a calculation for T2DM incidence using all three sample weights multiplicatively and setting the appropriate survey design for the two-stage sampling, but found no difference in T2DM incidence compared to the calculation with the drop out weight multiplied by the post-stratification weight.
The follow-up period in each study for participants without T2DM was defined as the interval between baseline and follow-up examinations, for participants with T2DM as the mean of this interval. The calculation of the incidence rate implies the assumption that the incidence is constant over different time periods. As the exact onset of T2DM is unknown for our data, the follow-up period in each study was defined as the interval between baseline and follow-up assessment. For each of the age-specific and sex-specific strata, the cumulative incidence (%) was calculated for the follow-up period of each study as well as the incidence rate per 1000 person-years and the average incidence per year with 95% CIs. Poisson regression models with robust SEs were applied to investigate whether incidence of T2DM differs across the different studies and to investigate which risk factors including body mass index, age and sex were associated with incidence of T2DM in the single studies. Statistical analyses were performed with STATA V.13.1 (Stata Corporation, College Station, Texas, USA). Geodata used for figure 1 were provided by the German Federal Agency for Cartography and Geodesy and by EuroGeographics.
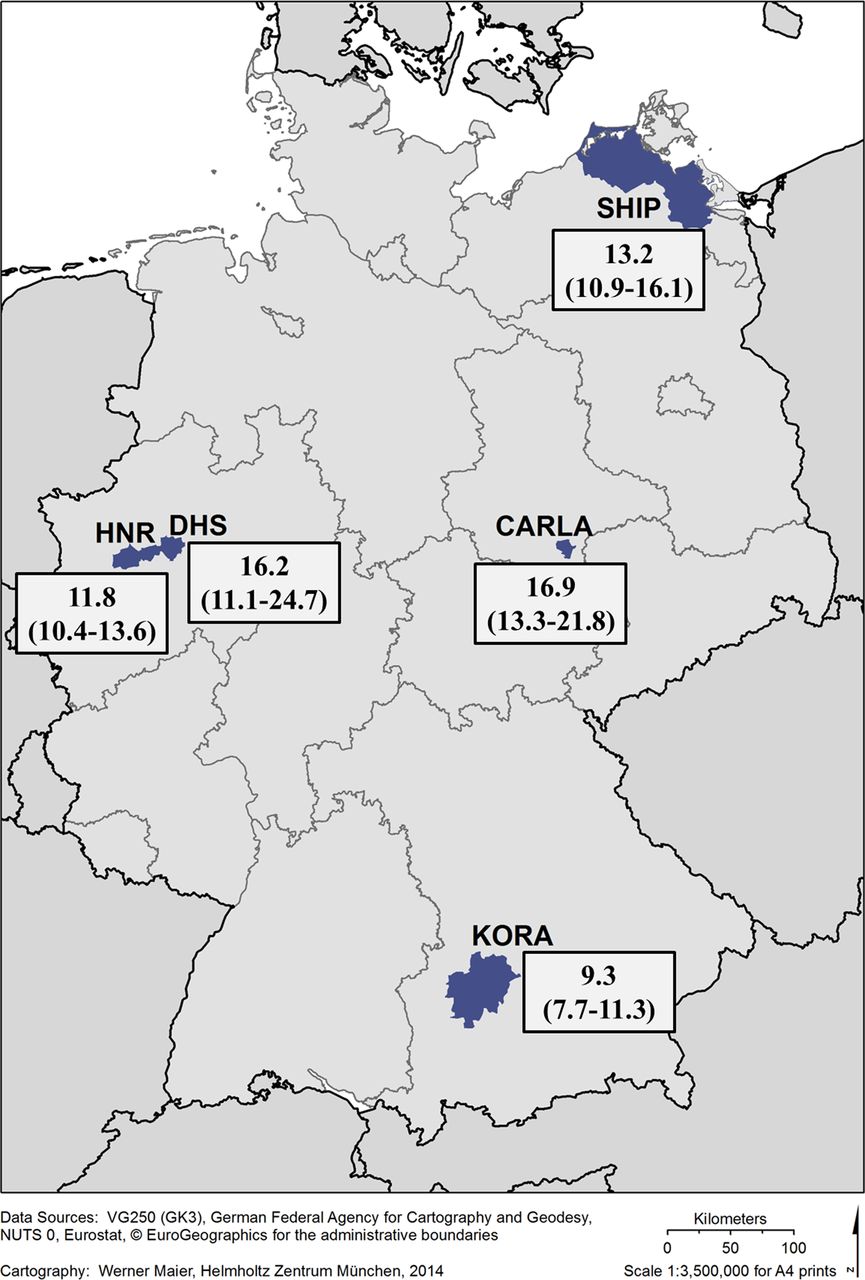
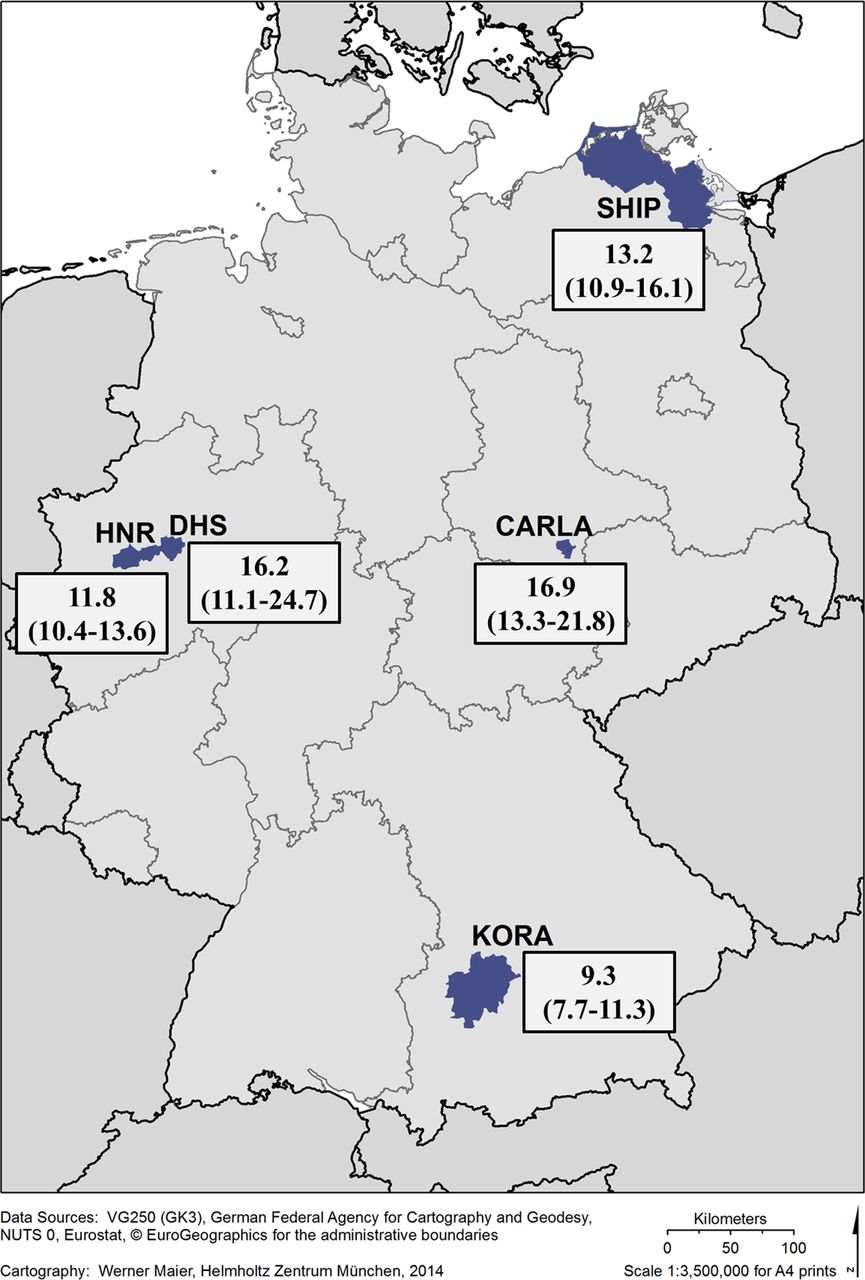{kind=link}
Regional incidence rates per 1000 person-years (95% CI) of self-reported type 2 diabetes mellitus (45–74 years at baseline) standardised to the German adult population (31 December 2007).
Results
Among the 8787 participants, 521 (5.9%) reported an incident T2DM corresponding to a standardised overall incidence rate of 11.8 (95% CI 10.8 to 12.9)/1000 person-years and an average incidence per year of 1.2% (95% CI 1.1% to 1.3%; table 3).
Baseline characteristics of participants of the analytic sample used as weighting factors by study and diabetes status
Regarding baseline characteristics which were used as weighting variables for losses to follow-up, participants differed according to study with respect to a number of characteristics (table 3). More men reported having T2DM with the highest proportion in CARLA (East), followed by SHIP (Northeast) and HNR (West). Participants with T2DM had a higher body mass index with the highest body mass index measured in SHIP (Northeast) and DHS (West), followed by CARLA (East). Current and former smokers were more frequent in T2DM, except for DHS with the highest proportion reported in CARLA (East), followed by SHIP (Northeast).
Regarding regional differences in the incidence of T2DM across Germany (table 4, figure 1), the incidence rate was highest in CARLA (East) and DHS (West), followed by SHIP (Northeast) and lowest in KORA (South). Along these lines, the average incidence per year was highest in CARLA (East) with 1.7% (95% CI 1.3% to 2.1%), followed by DHS (West) with 1.6 (95% CI 1.1 to 2.4), SHIP (Northeast) 1.3 (95% CI 1.1 to 1.6), HNR (West) 1.2 (95% CI 1.0 to 1.3) and KORA (South) with the lowest average incidence per year of 0.9 (95% CI 0.7 to 1.1; data not shown).
Regional incidence rates per 1000 person-years (95% CI) of self-reported type 2 diabetes mellitus (45–74 years at baseline) by sex and age*
We carried out a Poisson regression to estimate inter-regional differences for the incidence of T2DM. In comparison to the KORA in the South, the incidence rate ratios (IRR) were higher all other studies: SHIP, Northeast (IRR 1.44; 95% CI 1.09 to 1.90); CARLA, East (IRR 1.88; 95% CI 1.37 to 2.57); DHS, West (IRR 1.81; 95% CI 1.16 to 2.80); and HNR, West (IRR 1.31; 95% CI 1.03 to 1.66).
The incidence of T2DM increased with age and men were nearly twice as commonly affected as women (table 4). The highest incidence in men was generally found in those aged 55–64 years, whereas in women the incidence was highest in those aged 65–74 years.
We carried out a Poisson regression to estimate the association between the additional weighting variables (eg, education, smoking, body mass index) and incident T2DM. For all studies, body mass index was strongest associated with incident T2DM. The IRRs varied from 1.12 (1.09; 1.16) in KORA to 1.18 (1.14; 1.23) in CARLA.
Discussion
In the present study we investigated regional differences in the incidence of self-reported T2DM within Germany using data from five population-based cohort studies. The regional incidence rates varied from 16.9/1000 person-years in the East to 9.3/1000 person-years in the South. Compared to Germany as a whole, data provided by a large German statutory health insurance showed incidence rates of 1.4/1000 person-years for the age group 45–49 years and 8.6/1000 person-years for the age group 70–74.1 For England, population-based data estimated an incidence for T2DM of 7.3/1000 person-years.19 For the USA, the new cases of diabetes will rise from 8 cases per 1000 inhabitants in 2008 to 15 cases/1000 inhabitants in 2050.20 For Canada, the trend in incidence of diabetes increased from 6.6/1000 inhabitants in 1997 to 8.2/1000 inhabitants in 2003.21
The observed regional differences in the incidence parallels the differences recently reported for the prevalence of self-reported T2DM.3 The regional pattern in the occurrence of T2DM is tightly associated with previously reported regional differences in risk factor profiles including overweight, obesity and the metabolic syndrome.5–7 In our analysis, the body mass index was strongest associated with incident type 2 diabetes in all studies. According to nationwide data for Germany (1998–2011), among adults aged 18–79 years the prevalence of obesity increased considerably from 18.9% to 23.3% in men and 22.5% to 23.9% within a decade, in particular among younger adults.22 The prevalence of overweight has been stable with 53.0% for women and 67.1% for men within this decade. In the USA, about one-third of the differences in the prevalence of T2DM is associated with sedentary lifestyle and obesity.4
There are probably further factors for explaining the regional differences in the incidence rates. Differences in health and health-related behaviour are probably related to differences in the distribution of education, unemployment, income and private property among the federal states, cities or municipalities.8 The educational level demonstrated an association with the time to onset of T2DM.23 ,24 Both individual socioeconomic status (measured by educational level and equivalent income) as well as regional deprivation were associated with the prevalence of type 2 diabetes and obesity in Germany.23 The prevalence increased with increasing area deprivation with the highest deprived region in the Northeast and the lowest in the South of Germany.23 ,25
The comparison of KORA (South), HNR (West), CARLA (East) and SHIP (Northeast) data clearly demonstrates a regional gradient in the T2DM incidence. The DHS (West) region was located only 50 km away from the HNR (West) region, but DHS (West) demonstrated an incidence which was approximately one-third higher than the HNR (West) incidence and similar to the incidence of the East German studies CARLA (East) and SHIP (Northeast). When interpreting these results the small number of participants in the DHS (West) study which only counted for 26 incident cases of T2DM should be taken into account. This potentially resulted in a relative overestimation of the incidence. Nonetheless, public health initiatives are often carried out at a country level. With our results, scarce resources for prevention measures can probably be more efficiently implemented in regions in need.
Men in the youngest age group (45–54 years) had higher prevalence estimates than women, whereas women had higher prevalence estimates in the oldest age group (65–74 years).3 This sex-specific pattern is mirrored by differences in risk profiles for developing T2DM such as the metabolic syndrome and its components,26–28 the cardiovascular morbidity and mortality in men compared to women.29 ,30 Interventions should focus on sex-specific differences and have to consider particularly preventive measures tailored for men.
As expected, we found a general age-dependency of the T2DM incidence. Regarding overall sex-specific differences, men had an almost twofold higher incidence than women except for DHS (West). In the DHS (West), the estimates are based on a short follow-up time and a smaller number of cases limiting the precision. The mean follow-up time varied between the studies, for example, KORA (South) with 7.1 years and DHS (West) with 2.2 years. Since the incidence is more easily discovered and reported as people get older, our method of using the mean of the interval between baseline and follow-up may have resulted in an underestimation of the follow-up time for the participants with type 2 diabetes and thus to an overestimation of the incidence rate in studies with a short follow-up time.
Another methodological issue need to be taken into account. A subsample of participants aged 55–74 years of the KORA (South) study received an oral glucose tolerance test at baseline and was informed about the results. It is likely that participants were subsequently diagnosed for T2DM by the treating physicians. In addition, participants with disturbed glucose tolerance may have been followed-up closely by their treating physicians for identifying the diabetes onset at an early stage. In KORA (South), 8.7% of these participants had known T2DM at baseline, 8.2% had unknown T2DM, 7.2% impaired fasting glucose and 16.4% impaired glucose tolerance.14 Therefore, 50% of T2DM cases at baseline were detected by oral glucose tolerance test or fasting glucose. Furthermore, at the 7 years follow-up in KORA (South), another oral glucose tolerance test was carried out in all age groups. Based on this test, an incidence rate of 15.5/1000 person-years was estimated, which was among the highest in Europe.2 At baseline, almost 50% of T2DM cases were detected by oral glucose tolerance test or fasting glucose (unknown T2DM) and a similar fraction was found at follow up.14 ,31 Therefore, excluding undiagnosed T2DM for a homogeneous incidence estimation in all studies resulted in a comparatively lower incidence in KORA (South). Overall, in our analysis, the KORA (South) incidence (based on self-report) was even lowest among all five studies.
In addition to the aforementioned methodological considerations, two further limitations need to be considered when interpreting our results. First, possible misclassification of diabetes may have occurred by using self-reported T2DM only. The incidence of self-reported T2DM may be underestimated due to undetected cases and false-negative self-reports of diabetes diagnoses. In general, the specificity of self-reported incident T2DM can be considered as high, whereas the sensitivity is relatively low.32 Consequently, we may have underestimated the incidence for Germany. However, there is no reason to assume a differential information bias regarding self-reported information among the studies, which may have influenced our results on regional differences in incidence. Owing to the fact that healthcare is accessible for the whole population and more than 90% of the population utilise the ambulatory medical care in all of the 16 federal states in Germany, the regional differences in the incidence were probably not driven by under-utilisation of healthcare in some regions.33 Owing to diagnostic recommendations provided by the German Diabetes Association, differences driven by different diagnostic criteria probably play a minor role.34 Second, drop out is a common bias in cohort studies, which may have led to an underestimation of T2DM incidence. We partly controlled the bias by applying statistical weights that accounted for drop out from baseline to follow-up. Since responses were similar across the studies, selection may have played a minor role in biasing our results.
The strengths of the present study include the strict population-based design of all studies using comparable methods of data collection and diabetes definition. All studies are similar regarding selection of study population (two-stage sampling, stratified random sampling) and similar response rates. Except for DHS (West) and KORA (South), data were collected during similar time periods which reduced bias by temporary public health initiatives.
In conclusion, our DIAB-CORE consortium demonstrates relevant regional differences in the incidence of self-reported T2DM within Germany. The incidence pattern parallels the regional differences in the prevalence of T2DM. Our results strengthen the hypothesis that the observed differences may partly linked to prevalence differences in common risk factors for T2DM reflecting also sex-specific differences. Our findings are important for identifying groups at high risk to face the challenge of increasing prevalence of modifiable risk factors and for translating the results into municipality initiatives for preventing T2DM on a regional level.
What is already known on this subject?
-
In general, type 2 diabetes estimates are presented for the whole country. Epidemiological data on prevalence and incidence on a regional level are scarce. Furthermore, estimates are often less comparable due to different methodological issues. Previously, regional differences in the distribution of risk factors for type 2 diabetes mellitus have been reported.
What this study adds?
-
The present study includes a large sample size with high comparable data of population-based studies within the Diabetes Collaborative Research of Epidemiologic Studies (DIAB-CORE) consortium in Germany. Regional differences in the incidence of self-reported type 2 diabetes mellitus were detected within Germany. Our results give rise to the hypothesis that the observed differences may at least partly be due to the differences in risk factors for type 2 diabetes.
References
Footnotes
-
Contributors SS was involved in the conception and design of the study, carried out the data management and wrote the manuscript. TI performed the statistical analyses and contributed to the discussion and reviewed/edited the manuscript. TT contributed to the pooling of data and discussion and reviewed/edited the manuscript. RH, MS, WM, CM, BT, AK, KHG, KB, GM, SM, US contributed data and reviewed/edited the manuscript. AI contributed to the discussion and reviewed/edited the manuscript. WR provided data, contributed to the discussion and reviewed/edited the manuscript. HV provided data, contributed to the discussion and interpretation of the data and reviewed/edited the manuscript. All authors read and approved the final version.
-
Funding This work was supported by the Competence Network Diabetes mellitus of the German Federal Ministry of Education and Research (BMBF, grant 01GI0805-07). The Study of Health in Pomerania (SHIP) is part of the Community Medicine Research net (http://www.community-medicine.de) at the University of Greifswald, Germany. Funding was provided by grants from the German Federal Ministry of Education and Research (BMBF, grant 01ZZ0403); the Ministry for Education, Research, and Cultural Affairs; and the Ministry for Social Affairs of the Federal State of Mecklenburg–West Pomerania. The Cardiovascular Disease, Living and Ageing in Halle Study (CARLA) was supported by a grant from the Deutsche Forschungsgemeinschaft as part of the Collaborative Research Center 598 “Heart failure in the elderly - cellular mechanisms and therapy” at the Medical Faculty of the Martin-Luther-University Halle-Wittenberg, by a grant of the Wilhelm-Roux Programme of the Martin-Luther-University Halle-Wittenberg; by the Ministry of Education and Cultural Affairs of Saxony-Anhalt, and by the Federal Employment Office. The collection of sociodemographic and clinical data in the Dortmund Health Study (DHS) was supported by the German Migraine & Headache Society (DMKG) and by unrestricted grants of equal share from Astra Zeneca, Berlin Chemie, Boots Healthcare, Glaxo-Smith-Kline, McNeil Pharma (former Woelm Pharma), MSD Sharp & Dohme and Pfizer to the University of Muenster. We thank the Heinz Nixdorf Foundation (Germany) for the generous support of the Heinz Nixdorf Recall Study (HNR). The study is also supported by the German Ministry of Education and Science. We acknowledge the support of the Sarstedt AG & Co. concerning laboratory equipment. We thank the investigative group and the study staff of the Heinz Nixdorf Recall Study. The KORA research platform (KORA, Cooperative Health Research in the Region of Augsburg) was initiated and financed by the Helmholtz Zentrum München – German Research Center for Environmental Health, which is funded by the German Federal Ministry of Education and Research and by the State of Bavaria. The KORA Diabetes Study was partly funded by a German Research Foundation project grant to W.R. from the German Diabetes Center. The German Diabetes Center is funded by the German Federal Ministry of Health, and the Ministry of School, Science and Research of the State of North-Rhine-Westfalia.
-
Competing interests None.
-
Ethics approval All studies were approved by local ethics committees.
-
Provenance and peer review Not commissioned; externally peer reviewed.