Article Text

Abstract
Background In this partially randomised intervention study, we assessed the effect of social networks on the improvement of type 2 diabetes management in a largely African–American population in Baltimore.
Methods Patients in the intervention group (n=68) were asked to recruit peers, form small groups, and attend monthly diabetes education sessions, emphasising peer support. Patients in the control group (n=70) were recruited individually to attend standard diabetes education sessions. The primary outcomes were changes in haemoglobin A1C (HbA1c) and blood glucose. Secondary outcomes included blood pressure, weight, functional status, self-efficacy, perceived cohesion, social network connectedness and diabetes knowledge. General linear mixed models were built to assess mean absolute changes in primary and secondary outcomes at 3 and 6 months.
Results At 6 months from baseline, the social network intervention group achieved a larger reduction in HbA1c of −0.32% (p<0.0001) and blood glucose of −10.6 mg/dL, (p<0.0001) compared to the control group. In analyses of secondary endpoints, the intervention group had more favourable outcomes over time for weight, quality of life, self-efficacy, social network scores and diabetes knowledge, compared to the control group. While blood pressure decreased, and perceived cohesion increased in both groups over the duration of the study, the difference between groups was not statistically significant.
Conclusions The social networks intervention showed improved integration of patients within their existing networks leading to a greater reduction in HbA1c and blood glucose, as well as improved behaviour mediating outcomes.
- Diabetes
- Health Education SA
- Health Promotion
Statistics from Altmetric.com
Introduction
The evidence on type 2 diabetes self-management programmes highlights the finding that programmes organised as group interventions are more likely to report significant results compared to those administered on a one-to-one basis.1 This has been explained by the observation that in group interventions, a support environment emerges that stimulates patient activation.2 Such social support and activation help nurture self-efficacy (confidence in one's ability to take action) and a skill set for behaviour change, which are believed to promote better health outcomes and lower total medical costs.2 ,3 A sustainable patient activation approach that could be integrated into existing and future healthcare delivery systems is needed.2 ,4 The fragmentation of the healthcare system, missing reimbursement mechanisms for coordinated care,3 lack of available time and staff shortage,5 ,6 however, present significant barriers to implementing such interventions.
A central construct of chronic care models is based on the integration of elements of care related to activating patients, allowing for the time availability of providers, and engaging the community.5 ,7 New delivery approaches use the help of non-professional peer community members, who have been found to be as effective as trained health specialists in providing ongoing support for diabetes self-management.8–10 In this study, we capitalise on the activation of diabetic patients to become peer support coaches of one another, using a teach-back method. Our approach is based on the formation of clusters of peers, structured around the patients’ natural social networks of friends and relatives.11 Built on the principles of trust and reciprocity, social networks trigger support mechanisms resulting in increased levels of self-efficacy to maintain healthy lifestyle and treatment compliance.12
The goal of the ‘Diabetes Peer to Peer (P2P) Study’ was to assess the effect of social networks on the improvement of type 2 diabetes management in a largely African–American population from the Baltimore metropolitan area. The high burden of cardiovascular disease and diabetes, and their recalcitrant nature in African–American communities contributes to the existence of ethnicity-related health disparities and inequalities, thought to be best addressed by community-based participatory research.13–15 We hypothesised that social networks would activate patients to help improve haemoglobin A1C (HbA1c) and blood glucose. Additionally, we surmised that leveraging patients’ natural social networks will also help improve behaviour change mediators, such as social connectivity indicators, cohesion, self-efficacy and the knowledge of diabetes.16–18
Methods
An initial group of patients with type 2 diabetes was enrolled from medical practices and community sites associated with the University of Maryland School of Medicine and the University of Maryland Medical Center. The study population included patients who met the following eligibility requirements: HbA1c>7%, blood glucose >110 mg/dl and age 18 years or older. We estimated that with an average of three persons per cluster and a total of 150 patients, the study would have 81% power to detect an estimated 15% reduction in the effect size of HbA1c levels in the intervention arm compared to the control. The intervention referred to henceforth as P2P is described below. All patients signed an informed consent form. The study was approved by the Investigational Review Board at University of Maryland (HP-00051994).
Study design
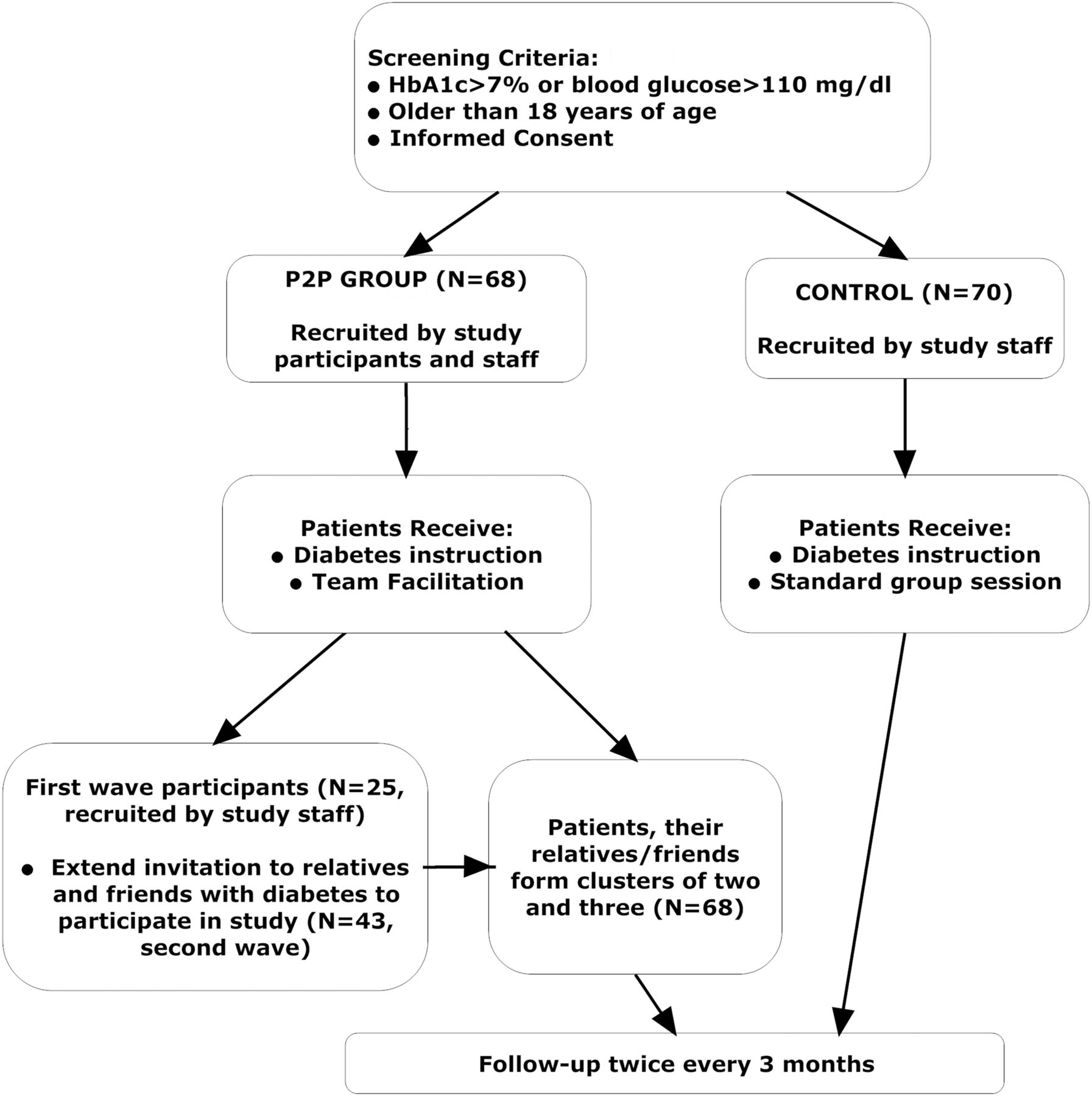
This was a partially randomised intervention study in which only index patients (approximately one-third of all patients) were allocated by randomisation. A first wave of 50 patients enrolled by the study staff was randomised into either of the two study groups. The initial 25 patients (first wave) who were randomised to P2P were asked to identify three to four peers (ie, neighbours, friends, or family members—second wave) who meet the study inclusion and exclusion criteria, for participation in the intervention arm of the study. Each first-wave participant, along with the two second-wave participants they recruited to the study collaborated as a group, resulting in small social network clusters of three participants each. All patients in the control group were intended to be enrolled by the study staff and were neither asked to refer peers nor instructed to form clusters (figure 1). While complete randomisation between the two groups would have been very difficult to accomplish given the differential recruitment schemes of the study and non-fully concurrent cohorts, we randomised index study participants to minimise any participation bias in favour of the intervention group.

Study design.
Intervention
P2P patients got in-person education sessions and were encouraged by a nurse practitioner to engage in team building exercises and share health information with their own cluster, turning it into a supportive group. The intent was to consolidate social networking and reinforce group cohesion, with a central theme of improving health outcomes, as mediated by improved dynamics. Patients in the control group were asked to attend diabetes education session with no further intervention. They received the same amount of in-person educational sessions, but the class style was a standard lecture class as opposed to the more interactive style of classes given to P2P patients. Control patients were neither taught nor encouraged to function as clusters. To minimise the chance of communication between groups, monthly sessions of the two groups and their follow-up visits were scheduled on different days, thus minimising the chance of interaction between groups.
The education curriculum included medical, nutrition, pharmacy and nursing, as well as non-smoking and exercise components. Information related to medications, the effects and the recognition and management of symptoms was also delivered. The pharmacy education programme was based on the P3 Programme at the University of Maryland School of Pharmacy.19 We focused on medication therapy management and used a patient-centred approach to education on drug-drug interactions, appropriate medication use and side effects.
Assessment of outcomes and follow-up
All patients completed a baseline assessment and underwent an initial medical evaluation. Data on age, gender, race, health condition, smoking, alcohol, education, marital status, insurance, use of medications, comorbidities, as well as parents’ medical history were recorded. Clinical indicators (HbA1c, blood glucose, blood pressure and weight) and survey data, including quality of life, self-efficacy, perceived cohesion, social network index and diabetes knowledge were collected on an individual basis. All assessments were completed at baseline and at two 3–4 month follow-ups.
The primary outcomes were HbA1c and blood glucose levels change from baseline. Blood pressure was measured with a blood pressure cuff, patient in the sitting position; two measures were taken and their mean was recorded. HbA1c was recorded from measures taken by a glucometer in clinical settings, either from the medical chart or from self-report. Secondary outcomes included mental and physical quality of life (SF-12 health survey,20) social network connectivity (Social Network Index questionnaire,21 which measures three social connectivity metrics—number of high contact roles, number of people in social network and number of embedded social networks), self-efficacy (General Self-Efficacy Scale,22) cohesion (the Perceived Cohesion Scale,23) and diabetes knowledge (Diabetes Knowledge Survey.24)
Statistical analysis
A descriptive analysis was performed to compare subjects’ characteristics at baseline and first and second follow-ups. Formal statistical analyses were based on multivariate general linear mixed effects models accounting for the repeated measures from the same patients and the clustering of the patients into teams. Multivariate analyses were performed using the ‘proc mixed’ procedure in SAS (V.9.2.; SAS Institute, Cary, NC). The best model fit for each modelled endpoint was determined using the ‘proc glmselect’ procedure with a model selection method based on the Schwartz Bayesian Information Criterion. The primary analysis was intention to treat, where any missing primary or secondary outcomes were assumed to be missing at random, and was based on patients who had at least one follow-up visit. The secondary analysis was performed on a population where missing baseline or first follow-up outcomes at 3 months were imputed under the assumption of no change between those two periods. More specifically, missing first follow-up values were imputed by using the observation carried forward method. We also looked into multiple imputation methods. However, the fit for those models was relatively poor—adjusted R-square of less than 30%—and a decision was made to not pursue further analysis due to uncertainty as to the amount and direction of bias this imputation technique will generate.
Results
A total of 140 patients were recruited into the study, of whom 138 completed the first follow-up and were retained in the analytic cohort—70 in the control arm and 68 in the intervention P2P arm (constituting 23 clusters from the first and second recruitment waves). Of those 138 patients, 6 dropped out after the first follow-up while another 37 did not complete a second follow-up due to late recruitment. Thus, there were 95 patients who completed both follow-ups (38 vs 57 in the control and P2P groups, respectively). Forty-four patients underwent their first follow-up 30–60 days past their original follow-up date (28 control and 16 P2P patients, representing 40 and 24% of each cohort, respectively).
Unadjusted analysis
The two groups were generally similar across all variables at baseline. The intervention group had higher BMI, lower prevalence of adverse medical history of the father, lower self-efficacy and lower diabetes knowledge than the control group (table 1).
Baseline characteristics
In the unadjusted analyses, both groups had statistically significant drops at the first follow-up (at 3 months) for HbA1c of −0.34 versus −0.50% (p=0.03) and of −5.60 versus −10.2 mg/dL for the control and P2P groups, respectively (figure 2 and table 2). At the second follow-up (at 3 months), both groups continued to exhibit decreasing values for HbA1c of −0.51% versus −0.77% (p=0.03) and blood glucose of −9.64 versus −17.4 mg/dL, respectively. For secondary endpoints, overall, the P2P group had more favourable outcomes over time: a recorded decrease in weight, and improvements in quality of life, self-efficacy, social network scores and diabetes knowledge, than the control group. While blood pressure decreased and perceived cohesion increased in both groups over the duration of the study, the difference between groups was not statistically significant (see online supplementary table).
Change from baseline in primary outcomes at 3 and 6 months in the control and P2P groups modelled using general linear mixed effects models

{kind=link}
{kind=link}
Change in HbA1c and blood glucose at 3 and 6 months (unadjusted).
Multivariate adjusted analyses
Primary endpoints
The P2P group had a statistically significantly greater reduction in HbA1c of −0.22% (CI −0.08 to −0.35%, p=.002) at 3 months and of −0.32% (CI −0.16 to −0.47%, p<0.0001) at 6 months. Likewise, the P2P group had a greater reduction in blood glucose (−6.61 mg/dL, CI: −2.84 to −10.4 mg/dL, p=0.0007 at 3 months; −10.6 mg/dL, CI −6.24 to −15.0 mg/dL, p<0.0001 at 6 months) than the control group (table 2). In the multivariate models, patients with self-reported good health, with Medicaid insurance, with heart trouble, on insulin and with increased BMI had higher HbA1c and blood glucose.
Secondary endpoints
The P2P group had a statistically significant greater increase in self-efficacy (0.16, p=0.02 at 3 months; and 0.21, p=0.004 at 6 months), number of high contact roles in the social network (0.61, p=0.04 at 3 months; and 0.66, p=0.04 at 6 months), number of people in social network (3.15, p=0.001 at 3 months; and 4.48, p<0.0001 at 6 months), number of embedded social networks (0.62, p=0.001 at 3 months; and 0.65, p=0.001 at 6 months), and diabetes knowledge (1.40, p=0.05 at 3 months; and 1.97, p=0.01 at 6 months) than the control group. Furthermore, the P2P group had a greater increase in the physical (3.25, p=0.06 at 6 months) and mental (6.73, p=0.002 at 6 months) components of the quality of life survey instrument SF-12, as well as decrease in weight (−2.98 lb., p=0.07 at 6 months). The two groups did not differ significantly with respect to changes in perceived cohesion, in systolic or in diastolic blood pressure. Generally, the analysis on the cohort with imputed values due to missing data resulted in a reduced effect size not substantially different from estimates obtained from original unadjusted and adjusted analyses.
Discussion
In this small pilot study, we show that a peer-led approach to type 2 diabetes management is very effective at improving diabetes outcomes. Patients who participated in the intervention group had a significantly larger drop in HbA1c at 3 months from baseline than the control. A prior systematic review on the effect of peer-led programmes in diabetes highlights the significant heterogeneity of peer intervention designs, and concludes that no specific pattern of a peer support model is most effective in achieving favourable diabetic outcomes, whether they are clinical, psychological or behavioural.25 In order to compare the results of our study with similar peer interventions, we identified four studies that reported significant reduction in HbA1c and were of the same duration of 6 months26–29 (table 3). Those had differing intervention designs ranging from online interaction with peers, automated telephone reinforcement, reciprocal peer support via an interactive telephone platform, as well as face-to-face peer coaches. Our study is innovative in that we explored a new type of peer intervention leveraging diabetic patients’ natural social networks aimed at creating an environment of ongoing peer-to-peer support in a high-risk population of African–Americans.
Summary of effect of peer-led interventions in type 2 diabetes
An additional strength of this study is that it evaluated multiple secondary endpoints important factors associated with glycemic reduction or barriers to diabetes self-management.30–32 We assessed the impact of leveraging patients’ natural social networks on measures of social network connectivity and cohesion, with the assumption that those variables will support behaviour change and mitigate modifiable risk factors, such as diabetes knowledge, self-efficacy and overall satisfaction. The favourable findings of our study with respect to secondary outcomes are in line with those of the systematic review on peer support reporting improved blood pressure, BMI/weight, physical activity, self-efficacy, depression and perceived social support.25 A comparison of effect sizes of those intermediary endpoints across studies, however, is difficult due to the use of different survey instruments. Elsewhere, patient activation has been found to increase medication compliance and has suggested that patients with initially low patient activation scores benefited the most from social support interventions.2. 4 We thus propose that the relationship between secondary endpoints, adherence and the change in clinical outcomes such as HbA1c be examined in a future study.
Despite the reported positive findings, we should emphasise that this is a small pilot study. An additional limitation of our study is that its results may not be readily transferred to the general population. For example, African–American patients have been found to rely more heavily on social networks to manage their diabetes than Caucasian patients.33 African–American patients also resort to family members as the most trusted health information source, even when health professionals are a common source of information.34 More studies in other high-risk ethnic minorities are needed to glean insight into the effect of social network peer support on the self-management of diabetes on a broad community level. Another limitation of the P2P study is its short duration of 6 months, which may not be long enough to evaluate whether the favourable effects of the intervention continue being sustained over a longer period of time. Furthermore, the lack of consistency in using the same brand glucometer or, perhaps, replicating the exact situations in which measures were taken might present some limitations to our study. Last but not least, there were 28 control and 16 P2P patients who had a late first follow-up. This, however, should bias our findings in favour of the control group as more patients in the control had a longer follow-up and thus a greater probability of reduction in HbA1c.
To the extent that our intervention was mostly focused on patients interacting together, we can assert that the effect was largely the result of peer-to-peer interactions. However, it is also true that the motivational skills used by study staff members implementing the intervention could also likely influence the effect size of the benefits of the intervention. While we did not use a standardised survey or any other metric to measure the separate impact of interpersonal skills of care providers in the study on patient outcomes, we do believe that those positive traits have helped facilitate the patient sessions and ignite patients interest and interactions. However, the same care providers also conducted the sessions for the control group, albeit with no emphasis on peer-to-peer interactions. Therefore, overall, the possibility of differential rate of motivational interaction among patients and intervention providers is limited.
While long-term outcomes of peer support intervention have been mixed,25 different health plans have already successfully incorporated new health delivery models for patient activation with diabetes.35 The Project Dulce model is perhaps the longest standing example of a feasible cost-effective partnership between the community and the health system, as it has been implemented in community health centres in San Diego County for more than 15 years.36 Furthermore, shared medical care models, where diabetic patients attend medical visits in a group, have also been shown to effect clinically significant improvements and to not be subject to financial barriers from the current US provider reimbursement system.37 The fragmentation of the US healthcare system also seems to not pose an insurmountable hurdle for implementing new care delivery systems engaging the community. Results from demonstration projects evaluating the usefulness and feasibility of patient-centred medical homes in managing chronic diseases, a care delivery model that emerged under the new healthcare reform in the USA holds further promise for the practicality of coordinating care in a joint community health system environment.38
The P2P social networks intervention showed improved social efficacy, diabetes knowledge and integration of patients within their existing clusters leading to a higher reduction in patients’ HbA1c and blood glucose at 3-month and 6-month follow-ups. Given the ample evidence on the existence of successful chronic care delivery models involving the community, the results from this study hold promise for changing diabetes management by organising care delivery and education efforts around diabetic patients’ natural social networks of friends, neighbours and relatives. Future studies should assess the effect of the intervention over a longer period of time than 6 months, and should expand the study population to include other races besides African–Americans.
What is already known on this subject
-
The effectiveness of educational intervention programmes in diabetes decreases after their discontinuation unless frequent patient–educator interaction is provided over a longer period of time, which is expensive.
-
The use of non-professional peer community members, found to be as effective as trained health specialists in providing ongoing support for diabetes self-management, can secure the sustainability of intervention programmes at the community level.
What this study adds
-
We found that leveraging patients’ natural social networks of friends and relatives leads to a greater improvement in diabetes self-management compared to a standard education intervention, and is an approach that could be integrated in new models for care delivery.
Acknowledgments
This study was approved by the Institutional Review Board of the University of Maryland, approval number HP-00051994. We are thankful to all study coordinators, investigators and patients who participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Contributors FS: conceived and designed this study, achieved funding, supervised data collection, contributed to data analysis and data interpretation, critically contributed to and approved the writing. VC: data entry and management, data analysis and data interpretation, wrote the manuscript and approved its final version. DH: patient recruitment, data collection, project management, contributed to manuscript writing, conducted patient education sessions and approved manuscript's final version. CF: patient recruitment, data collection, conducted patient education sessions, and approved the manuscript's final version. JC: study conception and acquisition of data, reviewed and approved manuscript's final version. SS: patient recruitment, acquisition of data and medical advice; approved the manuscript's final version. JF: study conception and acquisition of data, reviewed and approved manuscript's final version; KK—study conception and acquisition of data, reviewed and approved the manuscript's final version.
-
Funding The study was funded by Sanofi US. The Sanofi US authors provided input throughout the project; however, the principal investigator, Dr Shaya, maintained full control of the study design and conduct, data analysis and interpretation and final approval of the paper.
-
Competing interests JC, JF and KK are employees of Sanofi US. None of the other authors declare competing interests
-
Ethics approval University of Maryland (HP-00051994).
-
Provenance and peer review Not commissioned; externally peer reviewed.