Article Text

Abstract
Background Quantifying the potential health benefits of improvements in the nutritional quality of the average diet of a population would provide evidence for resource allocation between population-level interventions aimed at reducing chronic disease.
Methods A model was built linking consumption of food components with biological risk factors (blood pressure, serum cholesterol and obesity) and subsequent mortality from coronary heart disease, stroke and cancer. Meta-analyses of individual-level studies that quantified the RR of increased consumption/increased risk factor level on disease outcomes were used to build the model. The sensitivity of the model to the results from the meta-analyses was assessed with Monte Carlo simulations. Country-specific estimates of current nutrient intake compared against dietary recommendations for the UK were used to demonstrate the model.
Results Approximately 33 000 deaths per year would be avoided if UK dietary recommendations were met. The modelled reduction in deaths for coronary heart disease was 20 800 (95% credible interval 17 845–24 069), for stroke 5876 (3856–7364) and for cancer 6481 (4487–8353). Over 15 000 of the avoided deaths would be due to increased consumption of fruit and vegetables.
Conclusions The developed model estimates the impact of population-level dietary changes and is robust. Achieving UK dietary recommendations for fruit and vegetable consumption (five portions a day) would result in substantial health benefits—equivalent benefits would be achieved if salt intakes were lowered to 3.5 g per day or saturated fat intakes were lowered to 3% of total energy.
- Diet
- nutrition
- coronary disease
- stroke
- cancer
- modelling
- cancer epidemiology
- heart disease
- modelling ME
- nutrition
- stroke DI
Statistics from Altmetric.com
- Diet
- nutrition
- coronary disease
- stroke
- cancer
- modelling
- cancer epidemiology
- heart disease
- modelling ME
- nutrition
- stroke DI
Introduction
The allocation of finite health resources comes with a responsibility on the part of policy makers to make judgements on the potential benefit of committing resources in one way rather than another. Ideally, these judgements should be informed by assessments of cost-effectiveness of potential interventions. For many population-level interventions, the first step towards calculating cost-effectiveness is to model the effectiveness of achieving the intervention goals across the entire population, by estimating the resultant change in disease burden. One example of such modelling has been reported in a recent UK government paper on food policy—Food Matters—which estimated that 70 000 premature deaths every year could be averted if the average UK diet matched dietary recommendations for fruit and vegetables, salt, saturated fat and added sugar.1 However, the methods employed to calculate the Food Matters estimate are not clear.
As a first step towards estimates of cost-effectiveness of population-level dietary interventions, there needs to be a transparent model that can estimate the potential health benefits associated with changing population dietary levels. Poor diet has been convincingly linked with the incidence of cardiovascular disease and cancer,2 3 which are responsible for the majority of disease burden in most developed countries,4 but diet is multifactorial—a model of potential health benefits associated with different levels of nutrient consumption would provide evidence of whether dietary recommendations are set at appropriate levels, and which dietary recommendations deserve the fullest attention.
In this article, we report on a model that uses systematically identified measures of association between diet and health and data on current nutrient intake levels to estimate the number of cardiovascular disease and cancer deaths that could potentially be averted if better nutrient intake levels were achieved. To demonstrate the model, it is used to estimate the potential health benefits of achieving UK dietary recommendations.
Methods
The DIETRON model reported here is based on a conceptual framework that leads from consumption of foods and nutrients through to biological risk factors for ill health, through to adverse health outcomes. The conceptual framework is displayed in figure 1.

Conceptual framework supporting the DIETRON model. CHD, coronary heart disease; MUFA, mono-unsaturated fatty acids; PUFA, poly-unsaturated fatty acids.
Data sources
The outputs for the model were specified as mortality from coronary heart disease (CHD), stroke or cancer. To demonstrate the model, age, sex, country and cause-specific mortality for the calendar year of 2007 for the UK were obtained from the Office for National Statistics, the General Register Office for Scotland and the Northern Ireland Statistics and Research Agency. Definitions of conditions by codes for the tenth revision of the ICD are provided in table 1.
Meta-analyses used to derive the links between foods, nutrients, biological risk factors and adverse health outcomes
Food components were included in the model as inputs if either (1) a quantitative estimate of the association between the food component and CHD, stroke or cancer has been derived from a meta-analysis of individual-level studies or (2) a quantitative estimate of the association between the food component and a biological risk factor has been derived from a meta-analysis of individual-level studies, and a further quantitative assessment of the association between the biological risk factor and CHD, stroke or cancer has been derived from a meta-analysis of individual-level studies. An additional condition was assigned for links with cancer: that the association be defined as either ‘probable’ or ‘convincing’ by the World Cancer Research Fund.3 Sugars were not included in the model, since the relationship between sugar and cardiovascular disease, cancer or biological risk factors has not been established in a meta-analysis.
For the UK analysis, the current intake of the foods and nutrients included in the model was taken from the following sources: an average of 2005–2007 values for intake of fatty acids, fibre and fruit and vegetables derived from the Expenditure and Food Survey15; 2006 estimates of salt intake measured by urinary analysis, as part of an update of the National Diet and Nutrition Survey series16–18 (table 2). Estimates of intake for all food components were stratified by country of the UK, but were not further stratified by age or sex. Recent estimates of salt intake levels in Northern Ireland were unavailable, so it was assumed that salt intake levels were the same as in Scotland.
Sources of dietary current intakes and goals or recommendations
The DIETRON model was used to estimate the lives saved if the UK dietary recommendations for fats, salt, fibre and fruit and vegetables were achieved. Government dietary recommendations were taken from reports of the Committee on Medical Aspects of Food Policy or its successor, the Scientific Advisory Committee on Nutrition, and Department of Health policy documents19–21 (table 2).
Sources of data on association between food components, biological risk factors and CHD, stroke or cancer
Using computerised database and hand searching, we identified reviews providing estimates of RR for changes in food or nutrient intake in adults based on meta-analyses of studies on individuals. A meta-analysis was used in the model if it included data from randomised trials, cohort studies or case–control studies. Where more than one meta-analysis was available, priority was given to meta-analyses of randomised trials, then cohort studies and finally case–control studies. Details of the meta-analyses included in the model are provided in table 1. Where age- and sex-specific quantitative estimates of increased risk were available, they were included in the model. For both saturated fat and trans fatty acids, meta-analyses were available that would allow us to model the association between food component and health outcome directly or via blood cholesterol levels. In each instance, we chose to model via blood cholesterol levels. This was in order to follow the general principle that, where data are available, it is advantageous to generate structural models of disease risk that incorporate the underlying system under investigation.22
Assumptions
By combining a series of meta-analyses of individual-level studies, the DIETRON model estimates the change in RR of the adverse health outcomes for an individual who changes consumption of the food components included in the model. To estimate the total change in adverse health outcomes for a change in the average diet of a given population, the model uses the difference between current average consumption levels and modelled average consumption levels (eg, current UK recommended levels) of the food components as the input. It then interprets the estimated change in individual-level RR as the relative reduction in the number of adverse health outcomes that would be expected if the average consumption levels of the food components were changed to modelled levels.
The model therefore makes the following assumptions:
Combined changes in RR for individuals are multiplicative (eg, if consuming one extra portion of fruit and vegetables reduces risk of CHD death by 10%, and reducing salt intake by 1 g/day reduces risk of CHD death by 12%, then both of these behaviour changes reduce risk of CHD death by 1–(1–0.10)×(1–0.12)=20.8%).
Changes between current food component consumption levels and recommended consumption levels will be made by all individuals within the population changing consumption by the same amount (ie, a population shift in the overall distribution of consumption).
Reductions in RR for a unit change in food component consumption or proximal risk factor follows a dose–response relationship (eg, a change in consumption of fruit and vegetables from 2 to 3 portions a day has the same effect on RR as a change in consumption from 8 to 9 portions a day).
Uncertainty analysis
To test the uncertainty of the model to the estimates of association identified in the literature, a Monte Carlo simulation was conducted. Each of the estimates used in the model was allowed to vary according to the distribution reported in the accompanying literature. The 95% credible estimates reported here are based on the 2.5th and 97.5th percentiles of results generated from 5000 iterations of the model.
Results
The health benefits of achieving UK dietary recommendations estimated by the model are displayed in tables 3 and 4, with the potential reduction in mortalities split between sexes, age groups (all ages and under 75 deaths), country, disease and food component. Trans fat, MUFAs, PUFAs and dietary cholesterol have not been included in these results, since current government recommendations for these nutrients are for no change in consumption levels. The model estimates that there would be a reduction of around 33 000 deaths per year from CHD, stroke and cancer in the UK if dietary recommendations for fruit and vegetables, fibre, total fat, saturated fat and salt were achieved. This represents 14% of all deaths from the diseases that were included in the model. The model predicted the greatest (relative) reduction of mortalities in Northern Ireland and Scotland. This is because the populations of Northern Ireland and Scotland are furthest from achieving the dietary recommendations (especially fruits and vegetables). Around 18 000 of the reduced deaths were for men (15 000 for women), and around 12 500 of these deaths occur in people aged 75 and under.
Potential reduction in deaths by achievement of dietary recommendations by disease and dietary recommendation
Potential reduction in deaths by achievement of dietary recommendations by age, sex and country
The dietary recommendation that, if achieved, would produce the greatest reduction in mortalities is the recommendation to eat five portions of fruit and vegetables per day. Achieving this recommendation alone would reduce mortalities by approximately 15 000. Reducing the average salt intake to 6 g per day would reduce mortalities by around 7500 per year. Most of the predicted reductions in mortalities by achieving all recommendations are for CHD—nearly 21 000. In comparison, achieving the dietary recommendations would reduce stroke deaths by nearly 6000 a year, and cancer deaths by 6500.
Uncertainty analysis
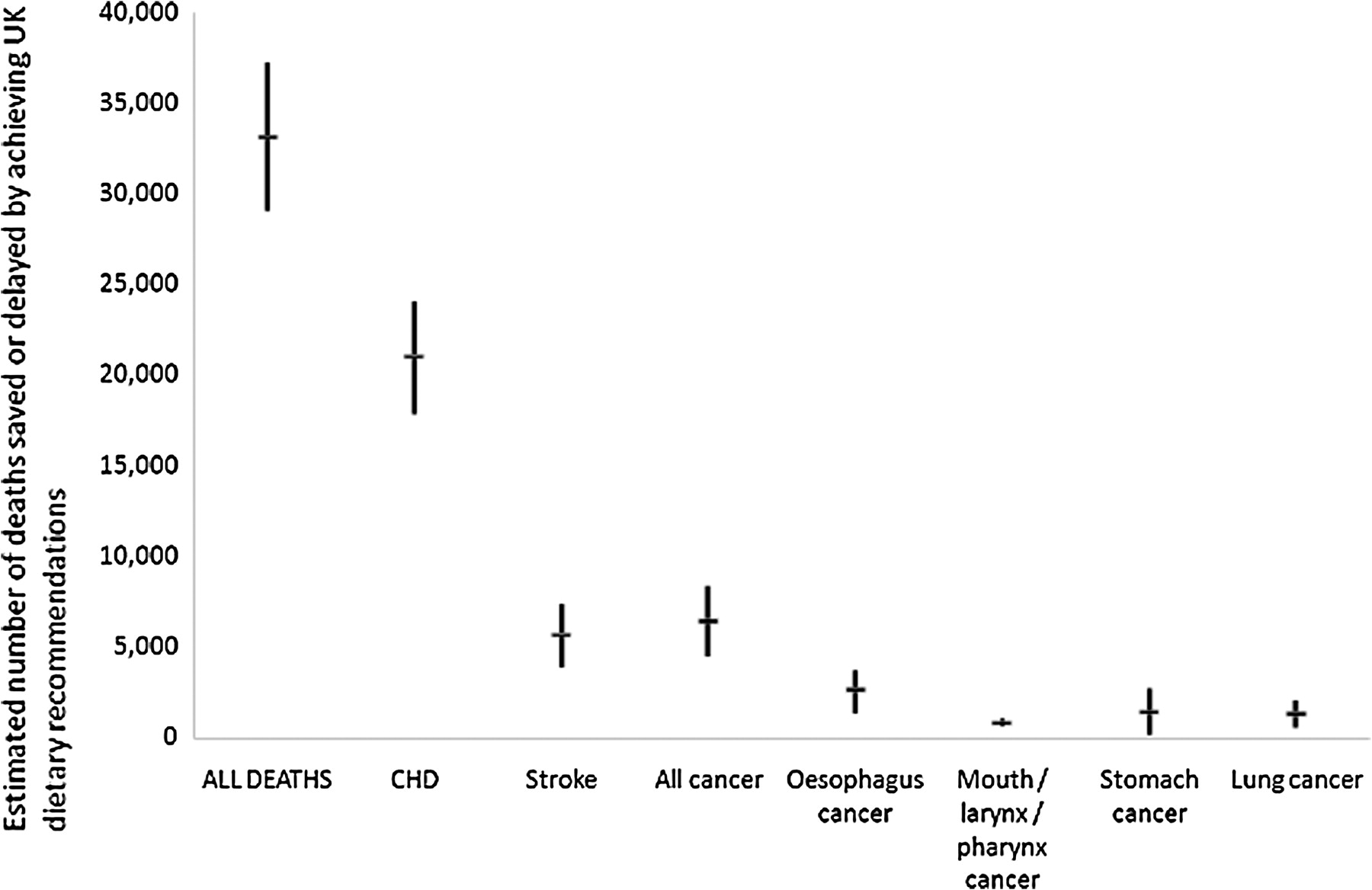
The Monte Carlo simulation suggested that the model is robust. The 95% credible estimates for predicted reduction in total mortalities ranged from 29 000 to 37 000. The model was relatively more sensitive to estimates of reductions in cancer mortalities than in CHD or stroke mortalities (see figure 2).
{kind=link}
{kind=link}
Estimate of number of deaths saved or delayed in the UK, by condition, with 95% credible intervals. CHD, coronary heart disease.
Discussion
This article introduces a model (DIETRON) that can estimate potential reductions in CHD, stroke and cancer deaths as a result of changes in average population dietary intakes, using parameters taken solely from high-quality meta-analyses of randomised controlled trials, cohort studies and case–control studies. The model has quantified avoidable mortality if the average diet of the UK population were consistent with government recommendations on intake of fruits and vegetables, fibre, salt and dietary fats. The results suggest that achievement of UK dietary recommendations would save or delay around 33 000 deaths annually, and go some way towards reducing geographic inequalities in health. The study was not concerned with either the cost or the effectiveness of potential interventions designed to achieve the recommendations, and as such the deliverability of these potential gains is not clear. The results contrast with the larger estimate of 70 000 potential deaths averted widely reported in the UK Government's Food Matters paper,1 which is over 30 000 deaths higher than the highest level set for the uncertainty analysis in this paper. The methods used for the Food Matters analysis were extrapolated from a previous impact assessment of the benefits of introducing restrictions of broadcast advertising of foods to children.23 The Food Matters model combines the effect of nutritional changes additively (as opposed to the DIETRON model, which combines changes multiplicatively) and uses individual studies (as opposed to meta-analyses) to quantify the association between nutritional change and health. The Food Matters estimate includes a reduction in 3500 deaths owing to reductions in added sugar intake, which is not included in the DIETRON model.
Our study suggests that increasing the consumption of fruits and vegetables to five portions a day is the dietary target likely to offer the most benefit in terms of deaths averted. According to the DIETRON model, in order to achieve a reduction in mortalities similar to those attained by achieving the fruit and vegetables recommendations, the salt recommendation should be set at 3.5 g per day; to achieve a similar reduction in cardiovascular mortalities, the saturated fat recommendation should be set at 3% of total energy.
Comparison with other dietary modelling techniques
There are at least two other models that have been developed that can estimate the impact on chronic health outcomes of changes in population dietary levels. One is a model that has been developed concurrently by the University of Liverpool.24 In contrast to the model presented here, the Liverpool model uses saturated fat, trans fat and salt as inputs, and CHD and stroke mortalities as outputs. The Liverpool model does not account for changes in body weight or for cancer-related health outcomes, does not allow for changes in population dietary intakes to be modelled simultaneously, and directly models the relationship between trans fats and cardiovascular diseases (as opposed to via changes in cholesterol). As a result of the difference in modelling trans fats, the Liverpool model predicts a greater impact of trans fats on cardiovascular mortality than the DIETRON model—we took the conservative approach of modelling the impact of trans fats via raised cholesterol only. The results presented in this paper are not affected by this decision, since the UK government does not explicitly recommend a reduction in trans fat levels in the average diet.
In the USA, the CHD Policy Model has been used to estimate the number of reduced CHD and stroke deaths that would be expected if dietary salt were reduced by 3 g/day.25 This model uses Markov cohort techniques to simulate state-transition in a representative simulated cohort of the US population. The same meta-analysis of the effect of salt intake on blood pressure is used for the DIETRON model and the CHD Policy Model, but different estimates of the effect of blood pressure on CHD and stroke are used. The CHD Policy Model estimates that between 44 000 and 92 000 deaths from CHD and stroke could be averted (between 8% and 16% of the 565 000 CHD and stroke deaths per year in USA)—a similar analysis using the DIETRON model on the UK population suggests that between 6000 and 8000 deaths from CHD and stroke could be averted (between 4% and 6% of the 145 000 CHD and stroke deaths per year in the UK). The difference lies in the estimation method—the CHD Policy Model follows a set population longitudinally and estimates the reduced number of mortalities over the lifetime of this population, whereas the DIETRON model estimates the number of reduced or delayed mortalities that would be expected every year, once the lag period of the impact of diet on CVD and cancer had passed. Comparison with the CHD Policy Model suggests that the total reduction in mortalities estimated here may be an underestimate of the total impact over the lifetime of the current UK population.
Strengths and limitations
This article reports on a model that quantifies the links between dietary factors, biological risk factors and adverse health outcomes using only high-quality meta-analyses to assess the associations between the elements of the model. The model is capable of estimating the impact of changes in many dietary elements on cardiovascular disease and cancer in any population provided that the necessary input data are available for that population. The development of the model was systematic, and the assumptions, data sources and connectivity of the model are described here transparently. This allows for an adequate assessment of the biases that could have been introduced in the modelling processes. The model included age-specific estimates of relative risks wherever possible, and included age, sex and country specific estimates of mortality to allow an in-depth assessment of how achieving the dietary recommendations could affect different populations within the UK. Country-specific estimates of current dietary intakes were included to allow for an assessment of the impact of achieving dietary recommendations on geographical inequalities. The multiplicative nature of the model accurately reflects the quantitative estimates of relationships between food components, biological risk factors and health outcomes that have been used to build the model. These quantitative estimates are of two types: relative risks for the links between food components/biological risk factors and health outcomes; estimates of change in biological risk factor for change in food component independent of other nutritional factors. Additively combining such estimates could produce erroneous results such as >100% reduction in mortalities.
The estimates of RR that have been used to parameterise the model were taken from results of meta-analyses reported in the scientific literature. Not all of the studies included in the meta-analyses adjusted their results for each of the dietary factors or biological risk factors that are included in the model. For example, the relative risks for CHD and stroke for 1 kg/m2 increase in BMI were not adjusted for serum cholesterol levels, and vice versa. Similarly, the effect of fruit and vegetables on CHD risk is likely to be partially mediated by dietary fibre, which is not accounted for in our model. It is therefore likely that some degree of double counting affects the model, and that (on these grounds) the estimate of reduced mortalities if UK recommendations are met is likely to be overestimated.
The model assumes that dietary recommendations will be achieved by shifting the current distribution of consumption levels within the population either to the left or to the right (ie, a population-level approach26). However, most dietary interventions—even interventions aimed at the whole population—are likely to be more effective in some groups than in others depending on their pre-existing levels of intake. For example, ‘5-a-day’ campaigns for increasing consumption of fruit and vegetables are unlikely to encourage individuals who already consume more than five portions of fruit and vegetables per day to consume more. It is also mathematically implausible to expect a whole population shift of distribution in nutrients such as salt where consumption is bounded at a minimum level of zero g/day. It is theoretically possible to model different changes to the distribution of dietary intake, and this could potentially improve the model developed here. The model also assumes that the associations between nutrients, foods, biological risk factors and health outcomes follow a linear dose–response relationship. In most cases, this linearity is supported by the meta-analyses used to construct the model as is demonstrated in table 1. However, this was not always the case: the associations between fruit and mouth, pharynx, larynx cancer, fruit/vegetables and stomach cancer, vegetables and stroke, and cholesterol and stroke did not demonstrate a linear dose–response relationship. These associations were included in the model, despite the non-linear relationship between intake and outcome, since it was felt that the inaccuracies introduced by assuming linearity were smaller than would be introduced by not including the association in the model at all. For the relationship between cholesterol and stroke, the deviation from linearity was not excessive.12
Conclusion
The DIETRON model estimates the impact of population-level changes in dietary intake and is robust. Achieving UK dietary recommendations could potentially reduce mortalities from cardiovascular disease and cancers by 33 000 a year. This figure, although substantial, is lower than a previous government estimate of 70 000. Most of the reduced mortalities would be achieved by increasing consumption of fruit and vegetables.
What is already known on this subject
A number of dietary factors have been shown to be associated with cardiovascular disease and cancer outcomes in meta-analyses. Achieving population dietary targets is therefore likely to reduce cardiovascular disease and cancer mortalities.
What this study adds
This study introduces a model which predicts change in population cardiovascular disease and cancer mortality levels given changes in mean consumption levels for fruit and vegetables, salt, fibre and fats. The parameters of the model are all derived from meta-analyses. The model can be used to estimate the effectiveness of population-level dietary interventions.
References
Footnotes
Funding British Heart Foundation and National Heart Forum.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.