Article Text

Abstract
Objective This study describes trends (1994–2007) in smoking in pregnancy (SIP) among an Australian population sample of women. This study also examines trends in the socioeconomic distribution of SIP over the 14-year period.
Methods Bivariate and multiple logistic regression analyses of the NSW Midwives Data Collection were used to explore the associations and trends in SIP by sociodemographic factors.
Results The prevalence of SIP in New South Wales (NSW) declined from 22.1% (1994) to 13.5% in 2007. However, the largest decrease in SIP rates was among the highest socioeconomic group (67.9% decline), and smaller declines were observed among teenage and remote rural mothers. Maternal age, ethnicity, Aboriginality, area of remoteness and socioeconomic status were independently associated with SIP. The distribution of NSW mothers has changed, with fewer younger mothers and more from an Asian background.
Conclusion This study reported large declines in SIP prevalence, with a population effect similar to that expected following exposure to (Cochrane-defined) intensive behavioural interventions. However, no specially targeted public health efforts were made during this period to influence SIP, so that social norm change is the likely explanation for these population health changes. The relative decline in SIP was smaller among low-socioeconomic status mothers, by language spoken at home, Aboriginality and area of remoteness, suggesting that inequalities in SIP have increased over this 14-year period. This information informs equity-based approaches to targeting further smoking cessation programs for pregnant Australian women.
- Pregnancy
- smoking
- socioeconomic status
- trends
- epidemiology FQ
- socioeconomic
Statistics from Altmetric.com
Many epidemiological studies have demonstrated that smoking in pregnancy (SIP) is associated with an increased risk of adverse pregnancy outcomes such as miscarriage, stillbirths, prematurity, low birth weight babies, neonatal morbidity, perinatal deaths, maternal mortality and even postnatal child health outcomes (eg, sudden infant death syndrome, brain tumour, childhood cancer, hearing problem, asthma and other respiratory infections).1–15
Over the last two and a half decades, there have been some declines in the prevalence of SIP worldwide.2–6 16 17 In some countries, rates remain high and continue to contribute to important and preventable public health problems.3–5 In the USA, the median State prevalence of SIP for 2006 was 22.4% and ranged from 5.8% to 34.7% across States.5 For the same period in Australia, overall 17.3% of women smoked during pregnancy, with a variation from 13.5% in New South Wales to 29.3% in the Northern Territory.3 Findings from the most recent survey (2005) reported that the rates of SIP were relatively similar with 17% across England and the UK overall and 22% in Wales.4 Cross-sectional studies have shown SIP to be related to socioeconomic status (SES), maternal age, partner smoking and cultural and ethnic background.16 18 19
Serial population surveys in Australia have reported that adult smoking rates in the general population have declined from 34% in 1980 to 19% in 2007, and this had occurred across both sexes (males: from 40% to 21%; females: from 29% to 18%).20 However, this decline was not evenly distributed across age and socioeconomic groups.20
Any SIP remains a public health concern in Australia, 3 16 21 and further investigation of socioeconomic trends and correlates may provide guidance for more targeted population-level interventions. The purpose of this paper is to describe the sociodemographic correlates of and trends in SIP in NSW and to investigate trends across socioeconomic groups in order to describe whether inequalities are widening.
Methods
The data were from the NSW Midwives Data Collection (MDC) 1994–2007, a population-based surveillance system administered by the NSW Health Department that covers all births (including homebirths and stillbirths) of at least 20 weeks' gestation or at least 400 g birth weight in NSW public and private hospitals.21 22 It relies on the attending midwife to complete a notification form when a birth occurs, and almost complete data enumeration occurs from all mothers giving birth. The form includes demographic items and items on maternal health, smoking, the pregnancy, labour, delivery and perinatal outcomes. Validation information on the MDC reported that the majority of the data items in the MDC showed more than 90% agreement, and the κ coefficients were 0.70 or higher.23
Pregnant mothers were classified as smokers or non-smokers according to their self-reported smoking status during pregnancy. They were classified as smokers if they ever smoked during the current pregnancy. The trends of smoking during pregnancy were examined for the following variables: mother's age, ethnicity (country of birth grouped into English-speaking background (ESB) and non-English-speaking background (NESB)), Aboriginal status and SES. SES was based on a geographic census-based measure, the socioeconomic index for areas (SEIFA) calculated by postcode of residence.24 The SEIFA describes the socioeconomic attributes of small geographical areas in Australia, using a number of underlying variables such as family and household characteristics, individual educational qualifications and occupation.24 For purposes of analysis, the SEIFA was used as both continuous (higher values indicate higher SES) and grouped variable. The SEIFA was grouped into quintiles from the most disadvantaged: (first quintile) to the least disadvantaged (fifth quintile). Trends of SIP were assessed over two time periods. As the SEIFA data are available only for census years (eg, 1996, 2001, 2006), the two points of time periods for trends were selected based on the census years and an earlier period (1995–1997) compared with recent data (2005–2007).
Bivariate (cross-tabulation) and multiple logistic regression25 analyses were used to explore the associations between sociodemographic characteristics and SIP. The prevalence of SIP and adjusted odds ratios (ORs) from logistic regression analyses were used as the measures for comparisons over time between the groups. χ2 Tests and 95% confidence interval (CI) for differences were used to test for statistical significance between the groups and across the periods. Because the SES was constructed based on census sociodemographic characteristics of a small geographic area, geographic region might be correlated with individual-level SES. Similarly, maternal country of birth and English-speaking born background are highly correlated. To deal with the problem of potential multicolinearity, this study excluded geographic region and maternal country birth from the logistic regression analysis.
Results
Trends in SIP by sociodemographic characteristics of the mothers
There was an annual increase in the absolute numbers of mothers in NSW, as well as decreases in the proportion of younger mothers (up to 29 years) and increases in the proportion of mothers from an NESB.
Between 1994 and 2007, the prevalence of SIP declined from 22.1% to 13.5% among NSW mothers (figure 1), which represented an overall 35.7% decline. During this period, a sharp declining rate was observed among NESB mothers (from 8.1% to 3.1%) as compared with ESB mothers (from 25.5% to 13.6%). Decline in smoking among all women in NSW MDC 1997–2007 was from 21.1% to 15.4% or around 0.57% per annum, compared with SIP rate among pregnant women, which declined from 20.6 to 12.8% or around 0.78% per annum (figure 1).

Trends in SIPi by maternal country of birth as compared with smoking for women at population levelii, 1994–2007. iSource: New South Wales Midwives Data Collection (NSW MDC) data 1994–2007, iiSource: NSW population health surveys 1997, 1998 and 2002–2007. There was no population health survey conducted during the period 1999–2001. Estimates are based on the following numbers of respondents for NSW: 1997 (17 496), 1998 (17 457), 2002 (12 616), 2003 (13 002), 2004 (9418), 2005 (11 490), 2006 (7957) and 2007 (7510). The indicator includes those who smoked daily or occasionally, and rates are weighted at population level.20
Comparing the two time periods (1995–1997 and 2005–2007), the proportion of SIP declined in each of the sociodemographic categories (tables 1 and 2). The rate of SIP decreased in all age groups, with greater decreases in the older mothers (30–39 years) compared with teenage mothers. SIP declined mostly among mothers from the highest-SES mothers, with a 67.9% decline between 1995–1997 and 2005–2007. The decline in SIP was comparatively lower among the ESB mothers compared with the NESB mothers. Overall, the SIP rate declined more slowly among the mothers living in rural and remote regions, compared with urban mothers (table 1). Irrespective of the time period, much higher rates of SIP were observed among teenage and Aboriginal mothers, with much lower rates of smoking among overseas-born mothers (tables 1 and 2).
Smoking rate (in %) during pregnancy by sociodemographic characteristics of mothers in NSW, 1995–1997 and 2005–2007
Likelihood of smoking in pregnancy (SIP) over the different periods of time by selected sociodemographic characteristics: results from multiple logistic regression analyses
Additional correlates of SIP compared for both time periods are shown in table 2. Compared with older mothers, those aged <30 years were more likely to smoke in pregnancy at both time periods, especially during the teenage years. English-speaking mothers were 4.2 and 5.6 times as likely to smoke during pregnancy for the 1995–1997 and 2005–2007 periods compared with NESB women, and indigenous mothers were more than three times as likely to smoke during pregnancy during both time periods (table 2).
Figures 2 and 3 examine the relationship between the continuous form of the SEIFA and the population rates of SIP. This was examined using Pearson's correlation coefficients that were calculated for both the periods (1995–1997 and 2005–2007) to examine whether the association between SES and SIP had changed and was examined separately for English-speaking (figure 2) and non-English-speaking mothers (figure 3). The correlation coefficient between the SEIFA and the prevalence of SIP showed a significant negative association for 1995–1997 (r=−0.616, 95% CI −0.56 to −0.66, ie, R2=0.379; p<0.001) and 2005–2007 (r=−0.681, 95% CI −0.64 to −0.72, ie, R2=0.463; p<0.001). This correlation coefficient indicates that SEIFA alone was a significant community-level determinant of SIP and accounted for 37.9% of the explained variation of SIP in 1995–1997 and 46.3% in 2005–2007. The strength of association between SEIFA and SIP for the later period was stronger than in the earlier period. This was consistent with the adjusted ORs for SES where, in 2005–2007, mothers in the lowest-SES quintile were 5.7 times more likely to smoke compared with the highest-SES mothers, while this was only 2.7 times as likely in 1995–1997 (table 2).

Socioeconomic index and prevalence of smoking in pregnancy (SIP) in New South Wales (NSW), 1995–1997 and 2005–2007. Equation for 1995–1997: fitted regression line (r=−0.616, 95% CI −0.66 to −0.56, p<0.001). Equation for 2005–2007: fitted regression line (r=−0.681, 95% CI −0.72 to −0.64, p<0.001). The proportion of SIP for each of the socioeconomic index for areas (SEIFA) was calculated, and the SEIFA was arranged in an ascending order (lower to higher) and treated as x-axis, and the corresponding percentage of smoking during pregnancy was plotted on y-axis. Same aggregate data set was used for correlation coefficient.

{kind=link}
{kind=link}
{kind=link}
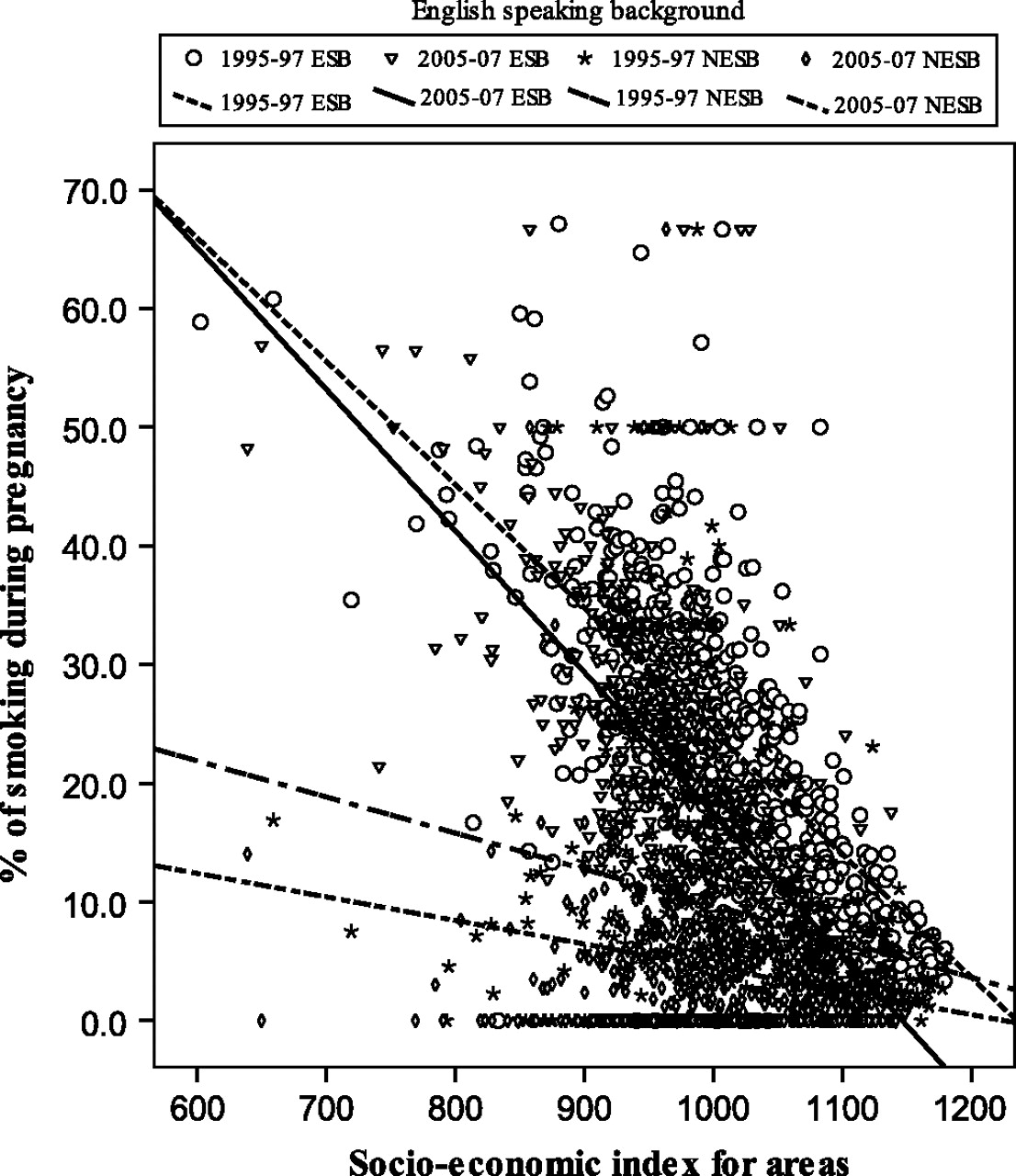
Socioeconomic index and prevalence of smoking in pregnancy (SIP) for English-speaking born (ESB) and non-English-speaking born (NESB) mothers in NSW, 1995–1997 and 2005–2007. Equation for 1995–1997 ESB: fitted regression line (r=−0.698, 95% CI −0.74 to −0.65, p<0.001). Equation for 2005–2007 ESB: fitted regression line (r=−0.717, 95% CI −0.75 to −0.68, p<0.001). Equation for 1995–1997 NESB: fitted regression line (r=−0.205, 95% CI −0.29 to −0.12, p<0.001). Equation for 2005–2007 NESB: fitted regression line (r=−0.195, 95% CI −0.28 to −0.11, p<0.001). The proportion of SIP for each of the socioeconomic index for areas (SEIFA) was calculated, and the SEIFA was arranged in an ascending order (lower to higher) and treated as x-axis, and the corresponding percentage of smoking during pregnancy was plotted on y-axis. Same aggregate data set was used for correlation coefficient.
Stratifying by country of birth showed different patterns for ESB and NESB mothers by SES. Figure 3 shows that SES was much more strongly correlated with SIP among ESB mothers (r=−0.698) compared with a much weaker ecological association for NESB mothers (r=−0.205). Further, the widening of socioeconomic differentials was not present among NESB mothers, shown by the similar correlations over the two periods (−0.205 in the earlier period and −0.195 in the 2005–2007 period).
Discussion
This study examined trends in SIP in NSW MDC 1995–1997 to 2005–2007. Consistent with that in other studies, the prevalence of SIP in NSW declined from 22.1% in 1994 to 13.5% in 2007.3 16 21 There has been a parallel but smaller decrease in smoking prevalence among the adult women (≥16 years) in the NSW general population (15.4% in 2007) and among adult Australian women (18% in 2007).2 20 However, smoking prevalence among pregnant women declined more steeply compared with that among adult women in the general population.
The effect size of this decline during 14 years is a remarkable public health achievement, even compared with secular declines in overall female smoking rates in the NSW population (figure 1). Other countries have also reported declines in SIP rates, with one national sample from Sweden showing educational differences in declines in SIP rates, with larger relative declines among more educated women.26 A Cochrane Collaboration systematic review of interventions for SIP was updated in December 2008,27 and estimated that intensive behaviour change-focused programs result in an average of 6% absolute differences in quit rates between intervention and control mothers. The population health change in NSW exceeds this level of change, with a 10% absolute difference in SIP rates over this period. This may be an international phenomenon, with similar declines in SIP rates reported for 2 decades in Sweden.26 28
It is interesting to note that no specific SIP-targeted campaigns or specific efforts were carried out in NSW during this period. Background antismoking efforts were strong and well funded, including NSW and national quit mass media campaigns; however, these mostly targeted the general population of smokers with no specific SIP campaign focus. Similarly, public health agencies in NSW concentrated their efforts on smoking policy (such as smoke-free hospitals) and on work targeting second-hand smoke (passive smoking risks to children) and targeting high indigenous smoking rates. Thus, this significant public health change appears to have occurred in response to a diffuse but generalised increased awareness among pregnant women,16 26 29 30 perhaps from increased advice provided through antenatal services16 and perhaps through unmeasured changes in community norms regarding SIP. Further research would be useful to elucidate the reasons for this change, including attitudinal and intention-to-quit measures as part of tobacco surveillance systems.
Irrespective of period and other demographic correlates, area of remoteness and SES were significantly associated with SIP. Population samples from Germany, Holland and the USA have also noted educational gradients in SIP31 32 or gradients according to mothers' occupational prestige.33 During the 14-year-period, the SES gradient in SIP in NSW increased, indicating widening socioeconomic inequalities in smoking. Other research has also noted widening socioeconomic inequalities in women who continue to smoke while pregnant.16 26 29 At-risk groups, similar to those in previous research, remain, including teenagers and Aboriginal mothers.16 18
Although ethnic differences in SIP have been previously reported,31 this NSW research shows that the SES gradient may be different for some subpopulations. NESB mothers showed less clear SES gradients and also showed more rapid declines in SIP in NSW. The lack of a socioeconomic gradient in NESB mothers smoking suggests a more complex relationship between maternal age of pregnancy, SES and ethnicity.
One of the limitations of this study was that the self-reported smoking status has not been validated for this data set, and the potential remains for differential social desirability to influence these estimates. However, for similar data sets in previous studies in Australia and overseas, validated self-reported smoking status showed very good association with urinary cotinine levels.18 34–37 The study measured the smoking status based on simple “smoke” versus “never smoke” dichotomy, which does not provide the information on smoking behaviour.38–40 Another limitation of this study was that SES was measured at an ecological level. Individual-level education and income status were not available and were not adjusted for in our analysis. A further limitation of this study was that mothers' SES was constructed based on the index of socioeconomic disadvantage for areas (SEIFA) calculated for NSW 1996 and 2006 census population by postcode of residence. The SEIFA was constructed from a set of census variables (annual income, ownership of motor cars, number of bedrooms, ownership of the household, qualification, employment status, number of men and women employed, number of dependants, number of adults aged 15+ years with marital status, occupied dwelling sharing with none, one or more families, Aboriginal status, country of birth (ESB or NESB) and English fluency) at postcode level, which might differ from individual-level measures of SES. This aggregate or population-level index is used in this analysis.
Many factors may have contributed to the decline in the prevalence of SIP, including the generic antismoking campaigns reinforced by environmental regulatory strategies.4 These efforts may have contributed to a lower prevalence of SIP but have not addressed the social and economic factors that are causing a widening of inequalities in this area. Specific audience segmentation may be required for the next generation of SIP prevention efforts, with targeting of messages, programs and services to those residents in socially disadvantaged regions.
Conclusion
Over the years, the prevalence of SIP has declined markedly across all sociodemographic groups in NSW, but in some subgroups, it remains a significant public health concern. The findings showed that sociodemographic characteristics of mothers were significantly associated with SIP. The particular concern in this study is the relative decline in SIP during the comparison period between 1995–1997 and 2005–2007 by SES, ethnicity, Aboriginality and area of remoteness suggesting that inequalities in the likelihood of SIP may be increasing rather than reducing. The information provided in this study will be useful from a policy perspective in focusing public health efforts and social marketing campaigns on more specific population segments, particularly young mothers, indigenous mothers, and all those resident in socially disadvantaged regions.
What this paper adds
This paper has provided strong evidence that a marked decline has occurred in SIP over the past 15 years, but in some population groups, the prevalence of maternal smoking remains high. The relative decline in SIP during the comparison period between 1995–1997 and 2005–2007 by SES, ethnicity, Aboriginality and area of remoteness has confirmed that SIP inequalities are increasing rather than decreasing.
Acknowledgments
The authors are grateful to the Centre for Epidemiology and Research, NSW Department of Health, for providing access to the NSW MDC data.
References
Footnotes
Competing interests We are not aware of any conflicts of interest associated with this research.
Ethical approval This study did not require ethics committee approval.
Provenance and peer review Not commissioned; not externally peer reviewed.