Article Text

Abstract
Background The incidence of autism rose dramatically between 1992 and 2001, while the age at which children were first diagnosed declined. During this period the size and composition of the autism caseload has changed, but little is known about whether the factors associated with the timing of diagnosis may also have shifted. Using a multilevel analysis strategy, the individual and community-level factors associated with age of diagnosis were modelled across 10 birth cohorts of California children.
Methods Linked birth and administrative records on 17 185 children with diagnoses of autistic disorder born in California between 1992 and 2001 and enrolled with the California Department of Developmental Services (DDS) were analysed. Information on cases, their parents and their residential location were extracted from birth and DDS records. Zip codes of residence were matched to census data to create community-level measures. Multilevel linear models were estimated for each birth cohort, with individual-level effects for sex, race, parental characteristics, poverty status, birth order and symptom expression. At the community level measures of educational and economic composition, local autism prevalence and the presence of a child psychiatrist were included.
Results Children with highly educated parents are diagnosed earlier, and this effect has strengthened over time. There is a persistent gap in the age of diagnosis between high and low socioeconomic status (SES) children that has shrunk but not disappeared over time.
Conclusion Routine screening for autism in early childhood for all children, particularly those of low SES, is necessary to eliminate disparities in early intervention.
- Age of diagnosis
- autistic disorder
- children
- multilevel analysis
- multilevel models
- social epidemiology
- socioeconomic
Statistics from Altmetric.com
- Age of diagnosis
- autistic disorder
- children
- multilevel analysis
- multilevel models
- social epidemiology
- socioeconomic
During the 1990s and early 2000s, autism diagnoses increased at a near-exponential pace.1 2 Simultaneously, the age at which children were diagnosed dropped.1 While in the recent past children may not have received an autism diagnosis until they entered school, they are now likely to be diagnosed in the preschool years.3 The spread of knowledge about autism among parents, physicians and teachers, widespread screening, and the belief that early treatment is associated with better outcomes for children all probably play a role in both increased and earlier diagnosis. However, the age of diagnosis has not declined uniformly for all children, and previous research suggests that factors such as sex, race, access to health care and severity of symptoms are associated with age of diagnosis.4 5 A recent analysis of a large sample of US children born in 1994 found that being male, having a low IQ, and experiencing developmental regression were all associated with earlier diagnosis.4
Early diagnosis is the crucial first step to early intervention, widely seen as important for later behavioural and cognitive outcomes in autism.3 6–11 In this article we report findings from a population-based study of age of diagnosis for autism in a large and racially diverse state, with a dataset sufficient to reveal how the factors leading to early diagnosis have shifted over the 10 birth cohorts spanning 1992–2001.
Timely diagnosis depends partly on the social contexts in which children are embedded. Information about typical child development, as well as the availability of resources, may flow to parents through contact with persons and institutions. Therefore, communities with differing levels of educational and financial resources, visibility of children with autism and access to health services may also differ in their tendency to facilitate or delay diagnosis. As prevalence of autism has risen sharply, so has its visibility. Furthermore, the socioeconomic gradient of autism diagnosis has shifted over this period; when once autism was diagnosed disproportionately among the wealthy and educated, it has recently begun to spread more evenly through the population (MD King and PS Bearman, 2010, unpublished manuscript). It is thus possible that as these factors have changed, so has the role of parental and community resources for the early identification of autism. We thus examine both individual and community-level factors that may affect the age of diagnosis.
Sample and methods
Description of data
The study includes all children with diagnoses of autistic disorder (Diagnostic and Statistical Manual of Mental Disorders, version IV (DSM-IV) code 299.0) enrolled with the California Department of Developmental Services (DDS) and born in California from 1992 to 2001. The California DDS, through its 21 regional centres, coordinates services and support for persons with developmental disabilities, including autistic disorder, and is the largest administrative source of data on persons with autism. Since 1992, DDS client development evaluation reports (CDER), including diagnostic and evaluative information, have been maintained electronically for each client; the vast majority are updated annually.
Enrolment with the DDS is voluntary; however, the provision of free services and support provides a strong incentive and so most eligible persons are enrolled.12 We matched DDS records on 18 127 individuals with autism born in California between 1992 and 2001 to their California birth records using probabilistic and deterministic matching algorithms based on first, middle and last name, birth date, race, zip code at birth and sex.13 Uncertain matches were manually reviewed. Overall, matches were found for 81% of all DDS cases; typically non-matches were born outside of California. We selected only the population of children with autism diagnoses (‘full syndrome’ or ‘residual state’, in DDS terminology) for whom California birth records could be matched for a total of 17 185 cases.
As a result of the 1992–2006 observation window for DDS records, the period of ascertainment diminishes for the later cohorts (eg, the 2000 birth cohort can only be observed to the age of 6 years). We thus restricted each cohort to children diagnosed between the ages of 2 and 8 years, in order to keep the observation period for each cohort as comparable as possible with respect to the range of age of diagnosis that is possible. We chose not to limit our sample further by the age of diagnosis, because this would arbitrarily limit the amount of variation on the dependent variable, and most importantly bias the estimates for the early birth cohorts when late diagnoses were common. We replicated our analysis on a sample of those diagnosed by age 6 years as a robustness check. This data structure might downwardly bias the magnitude of effect sizes relative to earlier cohorts with more age variation, making these conservative estimates.
This research was approved by the Institutional Review Boards at Columbia University and the California Committee for the Protection of Human Subjects.
Dependent variable
California statutorily requires that regional centres confirm eligibility for services, including verifying or conferring a diagnosis, within 120 days of intake, so the date at which DDS clinicians either provided or confirmed a first diagnosis of autism is within a few months of caregivers' initial request for assistance. Combined with the child's date of birth, we then used the date of entry from the first available CDER to calculate the age of diagnosis. Diagnoses earlier than age 3 years are empirically rare, as infants and toddlers below 36 months with suspected developmental delays and those considered at risk are served by the early start programme.
Independent variables
Individual-level variables include maternal race (as reported on the birth record), sex, comorbid diagnosis of mental retardation (from the CDER), maternal age in years, the maximum years of maternal or paternal education, maternal birthplace (within or outside the USA), poverty status (delivery paid for by Medi-Cal) and birth order (firstborn or later). These variables were chosen based on the results of earlier research, as well as theoretical considerations. We included birth order to test whether first-time parents are slower to recongize symptoms, and maternal immigration status to see if legal, cultural and language barriers affect the age of diagnosis.
The presence and severity of autism symptoms were captured by four variables extracted from the CDER: an index of communication function (a higher score means higher function); an index of social function (similarly coded); and dummy variables indicating the frequency of repetitive body movements and unacceptable social behaviours (see supplementary materials, available online only, for details on items and their coding). Reported autism severity, particularly the communication index, is correlated with age: older children tend to have higher function scores. Age-adjusted versions of the severity variables were considered, but rejected as age is the dependent variable. Although others have found cognitive function4 to be associated with the age of diagnosis, we could not include this measure as the DDS does not record IQ for clients with autism. We do include a dummy variable indicating if the child had a comorbid diagnosis of mental retardation, which should capture those with the lowest IQ; however, the absence of a measure of cognitive function is a limitation of this study. Descriptive statistics on all independent variables can be found in table 1.
Descriptive statistics on key measures, by birth cohort
Community-level variables are measured at the level of the zip code tabulation area (ZCTA)—geographical units created by the census bureau. ZCTA boundaries represent clusters of census tracts approximating the US Postal Service zip code service areas. Census tracts or block groups would prove too small to capture relevant environmental influences, and aggregations such as school districts are too large. Although imperfect, ZCTA provide plausible boundaries for the local residential environment. These variables are measured in the ZCTA associated with the five-digit zip code in which the child was living at the time of diagnosis, not birth, in order to capture the local social processes associated with timing of autism identification.
We calculate community autism prevalence as the square root (to reduce skewness) of the autism rate among children aged 0–10 years living in the ZCTA in the previous year. The educational and economic composition of the ZCTA are measured by the percentage of residents with a college degree, logged median property value, and the percentage of residents under the poverty line. These variables, as well as the denominator of the local autism rate, were taken from the 1990 and 2000 US census files. Linear interpolation and extrapolation were used to obtain estimates for the intervening years and for 2001–6. For zip codes created or eliminated by the postal service during the intercensile years (fewer than 5% of our sample resided in such places) we estimated growth based on the average growth rate in zip codes for which we had two points from which to interpolate. We also include an indicator for the presence of a child psychiatrist in the zip code, based on the American Medical Association physician master file from Medical Marketing Service, Inc.
Modelling strategy
We estimated multilevel linear models, with age of diagnosis as the dependent variable, on all autism cases, with both individual and community-level predictors. Separate models were estimated for each birth cohort, with the 1992–3 cohorts pooled due to small numbers in those years, using the ‘lme4’ and ‘arm’ libraries for fitting and displaying linear mixed-effects regression models in the R statistical software package.14 This mixed-effects approach accounts for the clustering of observations—persons within ZCTA—and allows us to model both individual-level and community-level effects simultaneously on the age of diagnosis of autism. Many ZCTA in the data contain only a small number of children, however multilevel regression is robust to small group size, so long as there is a sufficiently large number of groups.15
All continuous independent variables were mean centered and transformed into standard deviation units. Individual-level variables were centered by birth year; however, community-level variables were centered by year of diagnosis, as that is when the measurement occurred. Mean centering facilitates interpretable comparisons over time and between variables with different scales.
Results
Figure 1 displays the changing age of first autism diagnosis for the 1992 to 2001 birth cohorts. Clearly, there was a significant decline in the median age of diagnosis during this period, with most of the drop occurring after the 1996 birth cohort. Much of this decline is due to an increase in the proportion of children diagnosed at age 3 years.

Median age at autism diagnosis by birth cohort, with 95% CI for median. All cohorts are composed of those children born in a calendar year and diagnosed with autism without comorbid mental retardation before the age of 9 years but after 12 months.
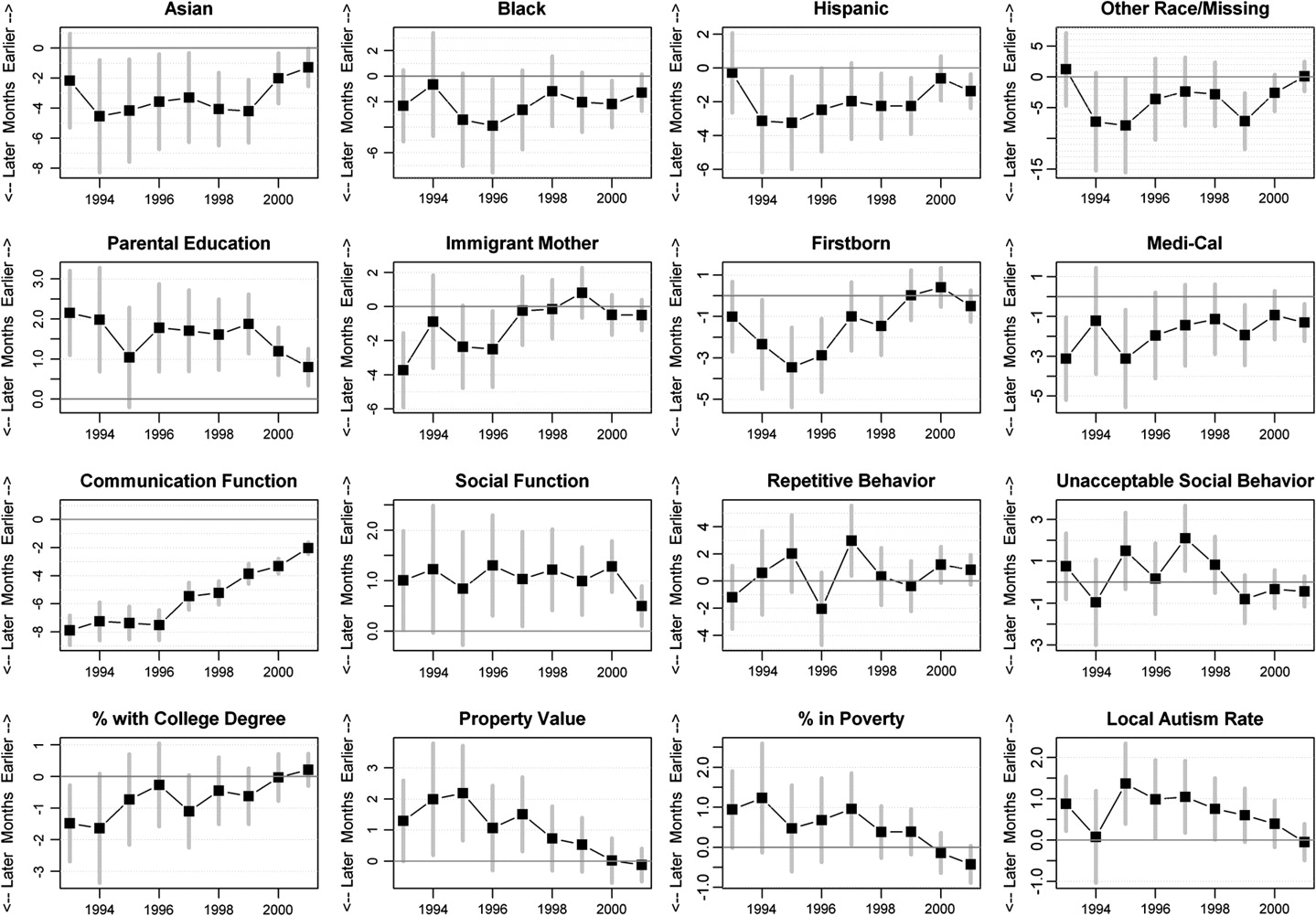
Full results from the multilevel regression models (including coefficient estimates, standard errors, and two-tailed p values) for all years are reported in table 2, where the dependent variable is the age of diagnosis in months, on a negative scale. Coefficients can be interpreted as the number of months earlier (or later, for negative coefficients) we would expect diagnosis to shift given a one standard deviation change (or shift from zero to one) in a predictor variable. Coefficient estimates with 95% confidence intervals for the selected variables discussed below are plotted over time in figure 2.
Regression results for multilevel models estimated for each birth cohort

Coefficient estimates with 95% CI by birth cohort for selected variables. Effect sizes can be interpreted as the number of months earlier a diagnosis occurs, on average, given a 1 SD change in the independent variable, ceteris paribus.
Individual-level factors
The top row of figure 2 contains results for maternal race/ethnicity, relative to non-Hispanic white individuals. In general, non-white and Hispanic individuals are diagnosed later. In the second row, we see that children with more educated parents are diagnosed earlier; this difference has remained robust over time. Having a mother born outside the USA and being first born were also associated with later diagnosis dates, although these effects disappeared in the later cohorts. Finally, children whose deliveries were paid by Medi-Cal were diagnosed later.
The third row contains the effects of symptom expression. With respect to autism symptom severity, we observe that on average, children with higher communication function were diagnosed much later than those with lower function. In the two earliest cohorts, this was nearly a 10-month difference; however, it shrank to only 2 months by the 2001 cohort. Recall, however, the problem of endogeneity with this measure, as older children tend to have higher communication function, net of age of diagnosis. A similar, but reversed, pattern holds for social function. Neither repetitive nor unacceptable social behaviour is associated with the age of diagnosis.
Community-level factors
Coefficients for community-level factors are in the bottom row of figure 2. While for individuals more education produces earlier diagnoses, high-education ZCTA tended to have later diagnoses, although the effect was marginally significant at first and diminished over time. The property value coefficient is consistently positive, suggesting that diagnoses occur earlier in wealthier communities. However, the coefficient for the percentage of households in poverty is also positive, although the effect size is quite small. Finally, areas with higher autism prevalence tended to diagnose autism slightly earlier. The coefficients for community-level variables tend to decline towards zero after 1998, indicating that the effect of community economic resources is disappearing as prevalence increases and diagnoses become more concentrated among 3 year olds.
Socioeconomic status
To illustrate the differential impact of SES on diagnostic timing, we calculated the predicted age of diagnosis for children with autism born at the high and low ends of the SES continuum in each birth cohort. Results are plotted in figure 3. The prediction equations used to calculate these values were based on the cohort-specific estimates presented in table 2, and assumed that children were at the mean or modal category for all variables except the selected SES-relevant variables. Panel A shows the fitted values for each hypothetical child, while panel B plots the trajectory of the SES ‘advantage’ gap over time. Low SES children (of Hispanic origin, with young and poorly educated, immigrant parents, on Medi-Cal, and living in poor, low-education areas) are represented by the solid line, while high SES children (white, with older and well-educated parents, in wealthy and educated neighbourhoods) are represented by the dashed line. In the early years of the study period, the gap was sizeable—high SES children were diagnosed approximately 16 months earlier. By the 2000 birth cohort, the size of this gap declined to approximately 6 months—not a small amount when you consider that these children only had approximately 3 years in which to receive a diagnosis.

{kind=link}
{kind=link}
{kind=link}
(A) Predicted age of diagnosis displayed for high and low socioeconomic status (SES) individuals. Predicted ages are calculated based on a mean of 10 000 posterior draws for coefficient fixed effects, for hypothetical individuals at the mean (or modal category) on all variables except those relevant to SES. The ‘high’ SES child is also male, white non-hispanic, has parental education and age at the 90th percentile, was born to a non-immigrant mother, was not born on Medi-Cal, and lives in a zip code at the 90th percentile for property value and education. The ‘low’ SES child is also male, but is of Hispanic origin, has parental education and age at the 10th percentile, was born on Medi-Cal to a mother born outside the USA, and lives in a zip code at the 10th percentile for property value and education. (B) The SES gap. Displays, in months, the relative advantage in early diagnosis for a high SES child compared with a low SES child.
Discussion
In this analysis of 10 birth cohorts of California children with autism, we found that socioeconomic factors, most notably parental education, race and maternal immigrant status, influence the age of diagnosis for autism. Socioeconomic status was a stronger predictor than even the severity of symptom expression at the point of diagnosis. Other significant risk factors include birth order, possibly because first-time parents may be less familiar with typical child development and thus slower to recognise the symptoms than more experienced parents, particularly in the early years before autism awareness was widespread. Unlike previous studies, we found no effect for sex.
At the community level, proximity to a child psychiatrist made no difference. Community-level socioeconomic factors had a small impact, although education had a negative effect, net of individual-level education and local financial resources. That is, living in a well-educated neighbourhood does not seem to matter, controlling for parents' education. Interestingly, the magnitude of community-level effects has diminished over time, as autism has become more prevalent. Some of this declining effect across nearly all risk factors may be due to diminishing variation in the dependent variable over time as age of diagnosis concentrated on age 3 years, leaving less to explain. This is true at both the individual and community levels.
The implications of this study are threefold. First, the factors leading to early diagnosis, although relatively consistent, do shift in their salience somewhat over time, which suggests that study designs pooling disparate cohorts over time might mask important patterns, and that it may be misleading to infer from past cohorts about children born and diagnosed in recent years. Second, as autism prevalence has increased, the age of diagnosis has become less dependent on the community in which a child with autism lives. Finally, we show that there are still risk factors for late diagnosis; since about 1998 these factors are mainly at the individual level.
Policy implications
Although autism awareness is widespread, certain parents, especially those with less education, may be less likely to identify their children's symptoms, or less able to marshal the resources required to obtain an autism diagnosis and services through the DDS system. Systematic differences persist between children in the typical age of diagnosis, as the results in figure 3 show. Underserved populations are still diagnosed 6 months later than those more advantaged. Although smaller than a decade before, this difference is non-trivial; early childhood is a time of rapid development. If early intervention is important, this disparity in the age of diagnosis has the potential to amplify socioeconomic differences in outcomes later on. These results suggests that physicians and healthcare providers should screen all children aggressively as a routine matter of care, including those whose parents may not have raised concerns. This strategy should continue to exert downward pressure on the age of diagnosis, and may result in the mitigation of durable socioeconomic disparities.
Limitations
Our data all come from California, which may limit generalisability to other locales. Other research has found significant regional variation in the timing of diagnosis.4 Variation in age at diagnosis should reflect such institutional factors as access to medical care, size and effectiveness of developmental services administration, availability of autism services, the presence of autism advocacy organisations, and visibility and awareness of autism in general. These factors vary by state, as health, disability and educational services are administered mainly at the state level. California's DDS, with its network of regional centres, is especially large and well developed, and has been shown to differ from other states with respect to its pattern of ascertainment of autism versus mental retardation.16 Furthermore, California is a large and geographically and ethnically diverse state, which may account for some differences between our data and those collected at other sites.
However, we believe the particular characteristics of California also provide advantages. In our data, we observe the effects of California DDS improving its system of ascertainment as the caseload rises and the age of diagnosis declines. As other states also improve their systems—particularly in the wake of the federal Combating Autism Act of 2006—we might hope to see less regional variation in the age of diagnosis. The size of the state and the DDS system further allow us to examine these relationships over time and for more recent birth cohorts than other studies. Finally, California is an unusually diverse state, and therefore may provide a glimpse of the country's diverse ethnic future.
The administrative nature of the DDS database is itself a limitation. First, although we do believe that the vast majority of eligible children are enrolled in the DDS, it is voluntary and so probably misses some autism cases in a non-random fashion, such as among underdiagnosed groups. In addition, we are limited by the collection of variables we have assembled from the DDS and the birth registry systems, which collect information for a different purpose than ours. For example, the lack of a measure of cognitive function is lamentable, as it is a factor shown in previous studies to be associated with the age of diagnosis. We remedy when we can with creative uses of available data, and by exploiting geographical variation to incorporate measures of social context. However, the possibility of omitted variable bias remains.
Future research
Replication of this type of analysis in other regions would tell us if these patterns are typical, or particular to California and the DDS system. Databases with both geographical and temporal variation, such as the Center for Disease Control and Prevention's autism and developmental disabilities monitoring network will be crucial for understanding patterns of autism diagnosis. Research is also needed to quantify the practical implications of differentials in diagnostic age. A 6-month delay in diagnosis and intervention might have very different meanings for a 3 year old and an 8 year old; however, it is unclear exactly what that difference might mean. Although there is evidence that early identification and intervention is beneficial to children with autism,3 6–11 little is known about how much earlier a diagnosis needs to occur for it to matter, and how the early intervention advantage varies with age.
Conclusion
This is the first paper to examine factors associated with the changing age of diagnosis of autism across a decade of successive birth cohorts at both the individual and community levels. We found that the effects of several individual and community-level variables have declined over time. At the individual level, however, children of highly educated parents reap greater benefits with respect to early diagnosis for autism and consequent opportunity for engagement in treatment, net of the severity of their disorder, than those whose parents are less educated. In general, children of high socioeconomic background continue to be diagnosed earlier than the less privileged, and although the gap has diminished it remains significant. It is thus crucial for paediatricians and policy makers to ensure that all parents, regardless of their level of educational attainment, have adequate information and the tools they need to identify autism early.
What is already known on this subject
Over the past two decades, as autism prevalence has increased, the age at which it is diagnosed has fallen. Previous research has identified several risk factors for late diagnosis, including parental education, race, sex, access to medical services and condition severity. This article investigates the correlates of diagnostic timing for a very large and ethnically diverse population of children with autistic disorder in California, born between 1992 and 2001. It is the first to examine risk factors at both the individual and community levels, and to analyse these relationships separately by birth cohort in order to observe changes over time.
What this study adds
As autism has become more prevalent and visible, the impact of community characteristics on the age of diagnosis has faded. However, some individual-level risk factors remain important, particularly parental education. The gap in the age of diagnosis between the highest and lowest SES children has declined over time, but a substantial and persistent gap remains. Awareness campaigns encouraging routine screening for autism among young children have had significant success; however, in order to eliminate socioeconomic disparities parents of disadvantaged children must have the knowledge and resources necessary to recognise symptoms and obtain services.
Acknowledgments
The authors would like to thank Keely Cheslack-Postava, Diana Dakhlallah, Ka-yuet Liu, Soumya Mazumdar and Noam Zerubavel for helpful suggestions.
References
Footnotes
Funding This research was supported by the NIH Director's Pioneer Award program, part of the NIH Roadmap for Medical Research, through grant number 1 DP1 OD003635-01.
Competing interests None.
Ethics approval This study was conducted with the approval of the Columbia University Institutional Review Board and the California Committee for the Protection of Human Subjects.
Provenance and peer review Not commissioned; externally peer reviewed.