Article Text

Abstract
Background Hypertension is becoming increasingly important in sub-Saharan Africa. However, evidences in support of this trend with time are still not available. The aim of this study was to evaluate the 10-year change in blood pressure levels and prevalence of hypertension in rural and urban Cameroon.
Methods Two cross-sectional population-based surveys in Yaounde (urban area) and Evodoula (rural area) in 1994 (1762 subjects) and 2003 (1398 subjects) used similar methodologies in women and men aged ≥24 years. Data on systolic and diastolic blood pressures (SBP and DBP), body mass index, educational level, alcohol consumption and tobacco smoking were collected during the two periods.
Results Between 1994 and 2003, blood pressure levels significantly increased in rural women (SBP, +18.2 mm Hg; DBP, +11.9 mm Hg) and men (SBP, +18.8 mm Hg; DBP, +11.6 mm Hg), all p<0.001. In the urban area, SBP increased in women (+8.1 mm Hg, p<0.001) and men (+6.5 mm Hg, p<0.001), and DBP increased only in women (+3.3 mm Hg, p<0.001). The OR (95% CI) adjusted on confounders comparing the prevalence of hypertension (blood pressure≥140/90 mm Hg and/or treatment) between 2003 and 1994 ranged from 1.5 (1.1 to 2.2) in urban men to 5.3 (3.2 to 8.9) in rural men.
Conclusion Blood pressure levels of this population have deteriorated over time, and the prevalence of hypertension has increased by twofold to fivefold. Adverse effects of risk factors could account for some of these changes. Prevention and control programmes are needed to reverse these trends and to avoid the looming complications.
- Hypertension
- blood pressure
- trends
- sub-Saharan Africa
- Cameroon
Statistics from Altmetric.com
Sub-Saharan African countries are experiencing rapid demographic and epidemiological transitions.1 These transitions are associated with increased susceptibility to non-communicable diseases (NCDs), dominated by cardiovascular diseases (CVDs) and related risk factors, such as obesity, diabetes mellitus and hypertension.1–5 Hypertension is a massive health problem, affecting about 20% of the adult population in developing countries.6 It has been projected that by 2025, 29% of the world adult population will suffer from hypertension, and most of those affected will be found in developing countries.6 Conscious efforts in many affluent countries, both at population and individual levels, have lowered the burden of CVD over the past few decades.4 7 Part of this change has resulted from the improvement in detection and control of individual risk factors and better management of cases.
Besides the already reported high prevalence of hypertension and other cardiovascular risk factors among African populations,8–11 we do not know how these factors change with time in the rapidly evolving African rural and urban settings, both as the result of their natural history and as the consequence of control and prevention programmes.
To explore some of these issues, we studied the temporal change in blood pressure levels and prevalence of hypertension in urban and rural Cameroonian adults over a 10-year period. We also sought to characterise urban–rural differences and identify potential predictors of the changing prevalence of hypertension.
Material and methods
Study design, setting and participants
Two cross-sectional surveys were conducted in 1994 and 2003 at the same sites in Cameroon, using similar methodology.12–14 The study sites were the Cité Verte urban health district in Yaounde (the capital city of Cameroon) and three villages of the Evodoula rural health area, 60 km from Yaoundé. In 1994, all individuals aged 24 years and above were invited to participate. The age of those finally recruited into the study ranged from 24 to 74 years. To keep the same age range across surveys, in 2003, we invited only individuals aged 24–74 years to participate. For each survey, the selection of participants was restricted to people who have been living on the study sites for at least 1 year before the surveys. Pregnant women were excluded from the study. The response rates in rural and urban areas were 95% and 91% in 1994 and 92% and 87% in 2003. The main reasons for not participating in the study were fears about the quantity of blood to be collected and of possible screening for HIV. A total of 1804 subjects took part in the 1994 survey, of whom 1762 had complete data. In 2003, 1478 subjects were recruited into the study, and 1398 had complete data. Only the participants with complete data were included in the analysis.
Data collection
Data collection took place at the nearest health facility and was conducted by nurses trained for the purpose of the study.9 Initial screening of participants included assessment of their alcohol consumption and tobacco smoking, their level of education, history of established hypertension and treatment and family history of hypertension. The classifications used were non-smoker (had never smoked), ex-smoker (had stopped smoking for at least 1 year) and smokers (current smokers). Alcohol consumption was based on the intake of alcoholic beverages during the last year, with three classes, such as non-drinkers (had never drank alcohol), ex-drinkers (had drank alcohol in the past, but had stopped for at least 1 year) and drinkers (current drinkers). The type of last educational institution attended was used, giving three categories, including illiterate (never attended), primary (1–7 years) and secondary or higher (7–14 years) in the rural area, and primary or lower (<7 years), secondary (7–14 years) and university (more than 14 years) in the urban area.
Height (to the nearest centimetre) and weight (to the nearest kilogramme) were measured using standard methods, and body mass index (BMI) was calculated for all subjects. They were classified as underweight (BMI<18.5 kg/m2), normal weight (BMI>18.5 and BMI<25 kg/m2), overweight (BMI≥25 kg/m2 and BMI<30 kg/m2) and obese (BMI≥30 kg/m2).
Participants had to be seated for at least 30 min before the measurement of blood pressure. Diastolic (DBP) and systolic blood pressures (SBP) were recorded three times on the right arm using a standard mercury sphygmomanometer and appropriate cuff sizes. The first and fifth Korotkoff sounds were used as indicators of SBP and DBP, respectively. The average of the second and third measures was used to define hypertension following two sets of criteria to account for the change in the definition of hypertension between 1994 and 2003:
Old criteria: SBP≥160 mm Hg and/or DBP≥95 mm Hg, or use of blood pressure lowering drugs;
Recent criteria: SBP≥140 mm Hg and/or DBP≥90 mm Hg, or use of blood pressure lowering drugs.
Statistical analyses
STATA V.8.2 was used for statistical analyses, and statistical significance was set at p<0.05. Analyses were stratified by sex and site of study (urban and rural). The results are reported as percentages (95% confidence intervals (CIs)) and mean (SD). The prevalence of hypertension was age standardised according to the Cameroonian 2000 population distribution.15 Differences between means were compared using Student t tests, taking into account the inequality of variances when necessary, and χ2 tests were used to compare frequencies. Multiple logistic regression models were used to assess the association between hypertension across surveys and potential predictors including age groups (24–34, 35–44, 45–54 and ≥55 years), alcohol consumption, tobacco smoking, education level and categories of BMI. Because of the interactions of (1) sex and study period for the prevalence of hypertension (rural: 2.03, 1.04–3.95, p<0.03; urban: 0.69, 0.43–0.96, p<0.03) and (2) place of residence and study period for the prevalence of hypertension (women: 0.68, 0.42–1.13, p=0.1; men: 0.31, 0.19–0.53, p<0.001), the results are stratified on sex and place of residence.
Ethical issues
The Helsinki Declaration on medical ethics was respected in the surveys. Approvals were obtained from the National Ethical Committee and the Ministry of Health, and signed informed consent was obtained from all participants.
Results
General characteristics of the study population
The 1994 and the 2003 participants were relatively young, with no age difference between men and women within sites. The mean age of urban participants was significantly lower than that of rural participants (p<0.001) (table 1). Men had higher educational level and drank and smoked more often than women. Rural men and women had similar BMI, while urban women had a significantly higher BMI than urban men (p<0.001 for both surveys).
Characteristics (mean (SD) or percentages) of the study populations in 1994 and 2003, by sex and place of residence
Rural–urban and sex differences in blood pressure levels and prevalence of hypertension
Mean blood pressures levels were significantly higher in men compared with women across surveys and sites. Urban and rural participants in the 1994 survey had similar SBP, while DBP was statistically significantly lower in rural participants (p<0.001) in the same year. However, in 2003, SBP and DBP were all statistically significantly higher in rural participants (p<0.001), probably because they were older. Reported family history of hypertension was more frequent among urban participants across surveys (all p<0.05). In 1994, rural women had a slightly higher prevalence of hypertension than rural men (table 2). The opposite was observed in the urban population. In 2003, using the ≥140/90 mm Hg cut-off values, rural and urban men displayed higher prevalences of hypertension compared with women. Assuming the ≥160/90 mm Hg cut-offs, urban women had a slightly higher prevalence of hypertension than urban men.
Crude and age-standardised prevalences (percentages) of screened and known hypertension in 1994 and 2003, by sex and place of residence
Changes in risk factor levels and prevalence
The mean age slightly increased within sites between 1994 and 2003 in men and women. This change, however, reached statistical significance only for urban women (p<0.003). In the rural population, BMI significantly increased between surveys by 1.2 and 0.6 kg/m2 in women (p<0.01) and men (p<0.02); in the urban population, there was no significant increase. During the study interval, the prevalence of alcohol drinking increased in both sexes and across sites, while tobacco smoking decreased in men (table 1).
Changes in blood pressure levels and prevalence of hypertension between surveys
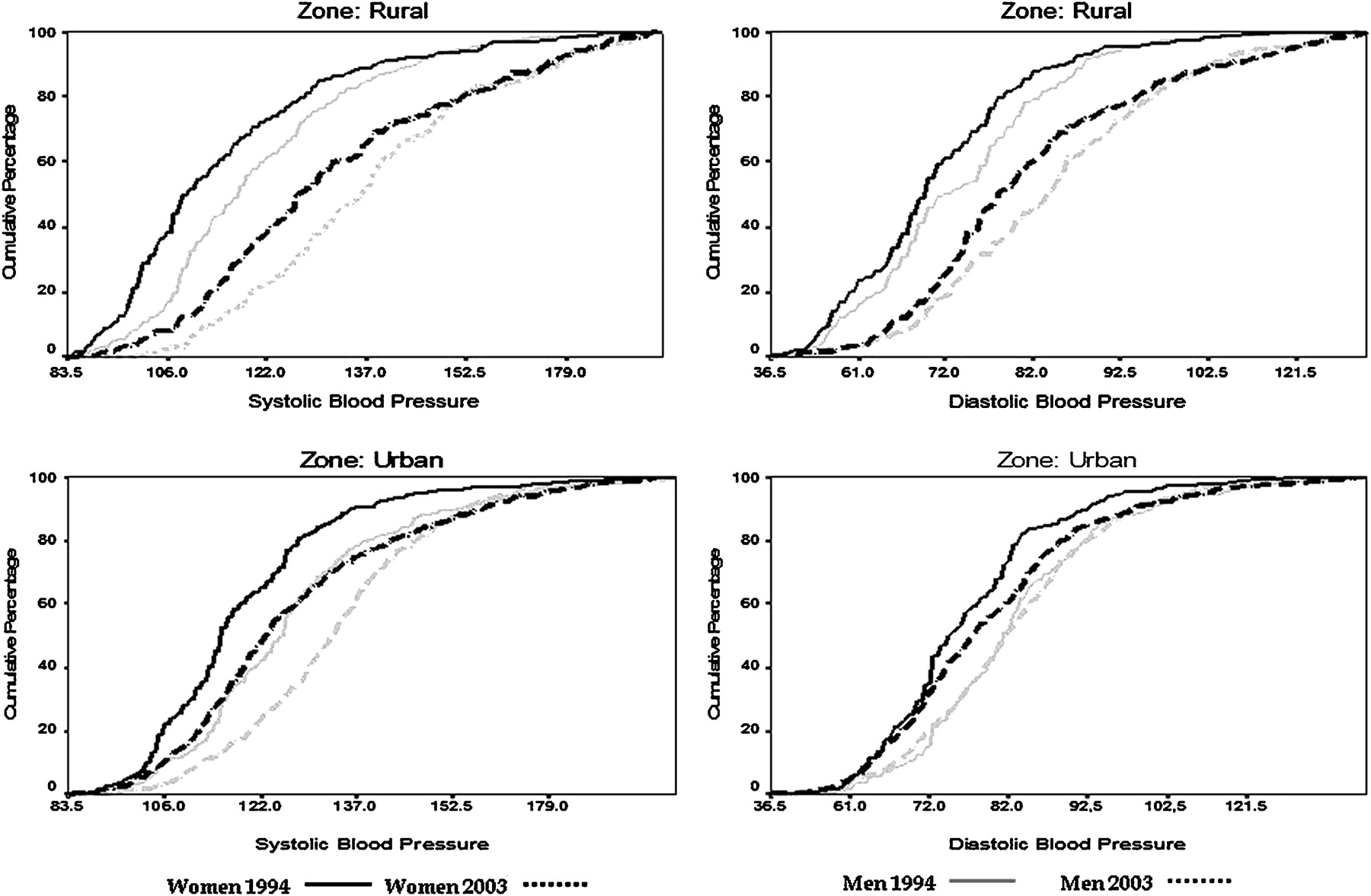
Across sites and in men and women, there was a systematic and significant increase in mean levels of SBP and DBP. As depicted in figure 1, the cumulative distribution curves of blood pressures shifted to the right in 2003 in comparison to 1994. This trend was more pronounced in rural participants. The prevalence of hypertension, crude and age adjusted, for the cut-off values ≥140/90 and ≥160/95 mm Hg, significantly increased by twofold to fivefold in rural and urban men and women over the 10-year period (table 2). These prevalences increased more in rural men and women than in their urban counterparts. Taken separately, the crude prevalences of both newly diagnosed and known hypertension increased between the two surveys. After taking into account age groups, BMI, education level, alcohol consumption and tobacco smoking, the prevalence of hypertension (BP≥140/90 mm Hg and/or treatment) in 2003 in comparison to 1994 increased significantly in both sexes in both rural (women: odds ratio (OR), 3.6, 95% CI 2.2 to 5.9; men: OR, 5.3, 95% CI 3.2 to 8.9) and urban (women: OR, 2.7, 95% CI 1.9 to 3.8; men: OR, 1.5, 95% CI 1.1 to 2.2) areas (table 3).
{kind=link}
Cumulative distributions of systolic and diastolic blood pressures in 1994 and 2003 by sex and place of residence in Cameroonians aged 24–74 years.
ORs and 95% CIs from multiple logistic regression analyses for hypertension (blood pressure>140/90 mm Hg and or treatment) with year of study, socioeconomic status and body mass index
Changes in the prevalence of hypertension and predictors
Irrespective of sex and place of residence, the prevalence of hypertension significantly increased with age and BMI groups (table 3). The highest odds of having hypertension, after adjusting for all other risk factors, were seen in the oldest subjects, aged 55–74 years. Classes of BMI were tightly associated with hypertension in men than women. Using the normal weight group as reference, being overweight was associated with significantly increased risk of hypertension in urban participants, but not in the rural ones. There was a different association of hypertension with alcohol consumption across sites, with a positive association in the rural area (significant only in men) and a negative association in the urban area (significant only in women). Education level was inversely associated with hypertension in women, although significant only in the urban area (table 3).
Discussion
This is the first study describing the temporal changes in blood pressure levels and prevalence of hypertension in black Africans, either in the context of its natural history or as an evaluation of control and prevention strategies. Average blood pressure levels in these populations significantly increased over the 10-year interval across sites in both men and women. The resulting increase in the prevalence of hypertension was higher in rural participants, reducing the rural–urban gradient previously observed. Age was a major predictor of the increasing prevalence of hypertension, while different associations were observed with BMI, education levels, alcohol consumption and smoking. One positive finding of this study was the increase in absolute prevalence of known hypertension across sites between the two surveys, mostly noted in rural men.
We carried out the two cross-sectional surveys on the same sites using similar methodology and included individuals in the same age range. We were therefore able to minimise the impact of unknown confounders. Our sample size was large enough to provide stable estimates across sites and study groups, as shown by the narrow CIs for most of our estimates. High DBP has been shown to regress by close to 5 mm Hg and SBP by as much as 10 mm Hg in untreated patients over 8 weeks.16 This raises the possibility of an overestimation of untreated hypertension in our population. However, SBPs above 160 mm Hg have been shown to remain elevated in more than 85% of subjects after three reviews.17
There was a general rightward shift of blood pressure with time, of up to 2 and 1 mm Hg per year on a linear scale for SBP and DBP, respectively (more pronounced in the rural area). This is mainly attributable to the increase in adiposity of Cameroonians between 1994 and 2003. Age was the main risk factor associated with hypertension in our study, followed by BMI. They are both established risks factors of hypertension. The prevalence of alcohol consumption increased between the two study periods, irrespective of place of residence and sex. It is positively related with hypertension. A decrease in physical activity levels, not documented in these surveys, particularly in the rural area, is another possible explanation for the trends found in our study. Between the two surveys, a highway was created, linking Evodoula to Yaoundé, the capital city of Cameroon, creating more opportunities for sedentary-prone occupations. During the same period, with more electrification of Evodoula, more people probably acquired TV sets and cars, and these would incur less leisure-time physical activity. This added to unhealthy eating habits and may explain the increase in weight and BMI noted between 1994 and 2003. The rapid urbanisation of Evodoula could explain why the changes in blood pressure levels were more pronounced in the rural area. Rapid urbanisation, in fact, is said to be the main driving force of the increasing prevalence of hypertension and NCDs in developing countries.18 Some other factors, such as the lower level of blood pressures in 1994 and the more rapid increase in educational level and alcohol consumption, may also have contributed to the increase. Furthermore, before 2003, there were no public health prevention programmes in Cameroon warning the population about the health effects of weight gain and sedentary lifestyle. Neither physical activity levels nor dietary intakes were taken into account when adjusting for confounding variables in the present study. They are both related to hypertension and could have reduced the ORs found in multivariate analysis between 2003 and 1994.
In many developed countries, studies have reported a reduction in the community level of blood pressure over time, mostly as a result of control programmes.5 Despite these achievements, the prevalence of hypertension tended to increase with time in these countries. This highlights the fact that the reported reduction in the absolute level of blood pressure probably occurred as a result of active management of cases through widespread use of drug treatment. In fact, the downward trends of blood pressure as a consequence of community prevention programmes have been reported by a few studies, including the North Karelia study7 and the Mauritian non-communicable prevention programme.19 Countries that have reported improvements in the community level of blood pressure over time have had effective prevention and control programmes.20 NCDs were only recognised as a health priority in Cameroon in 2006, and prevention and control strategies are still at an embryonic stage. Communicable diseases, dominated by malaria and HIV/AIDS, and financial constraints are likely to limit the government's efforts.
One positive finding of this study is the increased absolute prevalence of known hypertension across sites between the two surveys, mostly noted in rural men. This can be explained by the increased prevalence of hypertension in the community. It is also likely the result of the efforts of the population and healthcare providers to diagnose hypertension, as well as the lowering of diagnostic criteria for hypertension between the two surveys. However, the ratio of known to undiagnosed hypertension has worsened. Our study confirms the persistently high rate of undiagnosed hypertension in both surveys, as previously reported in Cameroon.9
This report shows an increasing prevalence of hypertension in the studied populations over time. The results of this study confirm the rapid epidemiological transitional process underway in sub-Saharan Africa. Part of the observed changes can be explained by the adverse profile of other risk factors, notably obesity. The absence of concerted prevention and control efforts is another explanation, as shown by the high proportion of undiagnosed cases. Other factors not readily apparent in this study may have also contributed to the changes. The exploration of all these contributing factors should lay the foundation of any strategy aimed at reversing the observed trend. A plea is made for much greater epidemiological research with regular monitoring of trends of hypertension and other cardiovascular risk factors. This is necessary in order to obtain reliable figures for the prevalence of disease, to determine the best ways of applying current knowledge with existing and future resources, and to obtain information regarding the determinants of these changing trends and their impact on the incidence of attendant CVDs.
What is already known on this topic
Hypertension is a major health problem in sub-Saharan Africa.
There is a rural–urban gradient in the prevalence of hypertension in this part of the World.
What this study adds
Blood pressure distribution curves of this population have shifted to the right with time.
The resulting increase in the prevalence of hypertension has affected the rural population more than the urban one and has therefore significantly narrowed the previously described rural–urban gradient.
Acknowledgments
We thank Dr Richard Edwards for carefully reviewing the manuscript. We also thank a number of collaborators on these two surveys, particularly Dr Felix Assah, who monitored data collection in the field in 2003.
References
Footnotes
Funding European Union for the 1994 survey and the French Institute for Research and Development (IRD) through Aire Developpement for 2003 surveys. The funding bodies were not involved in the study design, data collection, analysis, interpretation or writing of the article. They had no control or influence over the decision to submit the manuscript for publication.
Competing interest None.
Ethics approval This study was conducted with the approval of the Cameroon.
Provenance and peer review Not commissioned; externally peer reviewed.