Article Text

Abstract
Study objective: To analyse the association between perceived discrimination and refraining from seeking required medical treatment and the contribution of socioeconomic disadvantage.
Design and setting: Data from the Swedish National Survey of Public Health 2004 were used for analysis. Respondents were asked whether they had refrained from seeking required medical treatment during the past 3 months. Perceived discrimination was based on whether respondents reported that they had been treated in a way that made them feel humiliated (due to ethnicity/race, religion, gender, sexual orientation, age or disability). The Socioeconomic Disadvantage Index (SDI) was developed to measure economic deprivation (social welfare beneficiary, being unemployed, financial crisis and lack of cash reserves).
Participants: Swedish population-based survey of 14 736 men and 17 115 women.
Main results: Both perceived discrimination and socioeconomic disadvantage were independently associated with refraining from seeking medical treatment. Experiences of frequent discrimination even without any socioeconomic disadvantage were associated with three to nine-fold increased odds for refraining from seeking medical treatment. A combination of both frequent discrimination and severe SDI was associated with a multiplicative effect on refraining from seeking medical treatment, but this effect was statistically more conclusive among women (OR = 11.6, 95% CI 8.1 to 16.6; Synergy Index (SI) = 2.0 (95% CI 1.2 to 3.2)) than among men (OR = 12, 95% CI 7.7 to 18.7; SI = 1.6 (95% CI 1.3 to 2.1)).
Conclusions: The goal of equitable access to healthcare services cannot be achieved without public health strategies that confront and tackle discrimination in society and specifically in the healthcare setting.
- SDI, Socioeconomic Disadvantage Index
- SI, Synergy Index
Statistics from Altmetric.com
Access to healthcare services is an important determinant of health.1 However, access to healthcare services is conditioned by coverage2 and various factors including socioeconomic circumstances,1,3,4 care-seeking behaviours and the behaviours of healthcare providers.5–7 Previous studies from the US and UK have demonstrated ethnic discrimination can limit access to healthcare services among minority ethnic groups.7,8,9,10,11 However, there is a scarcity of studies on the effects of other forms of discrimination on access to healthcare services and other determinants of health. In Sweden12 and the US13 racial discrimination has been associated with limited participation in the labour market and unfavourable socioeconomic circumstances. However, the modifying effects of socioeconomic disadvantage on the association between discrimination and access to healthcare services have been analysed less often.7 Generally, public health research on the effects of perceived discrimination on health and its determinants, including access to healthcare services, is still in its infancy in many European countries, particularly in the Nordic countries.
In Sweden, the commonly discussed forms of discrimination have been gender and disability. Recently, discrimination due to ethnic background, sexual orientation or age has come up in political debates. Currently, there are legislations against institutional discrimination (because of sex, disability, ethnic background and sexual orientation); however, there are no systematic mechanisms to monitor the occurrence of discrimination.13 More so, the effects of discrimination on health and its determinants are not well documented.
Sweden’s public health policy is based on the principle of equality and care on equal terms for all irrespective of social position.14 In addition, Sweden has universal health insurance, where 94% of the healthcare system is publicly financed. The remaining 6% that is not publicly financed is related to non-traditional alternative medical treatments or plastic surgery unrelated to medical problems.
A fundamental principle is that the healthcare provision and financing for the entire population is the responsibility of the public sector. The 21 county councils have the primary responsibility of financing, administering and delivering healthcare services to inhabitants. Thus, it is assumed that all Swedish inhabitants should be able to access the care that they need, regardless of class, gender, ethnicity/race, religion or disability.
Over the past 20 years, Sweden has changed from a homogeneous to a multicultural society, with about 20% of the population now consisting of immigrants from other countries. There are contradicting results on whether individuals born outside Sweden overutilise or underutilise the healthcare services.15,16 It should be noted that healthcare utilisation may be different from seeking required medical care.
In this study, we attempted to investigate the association between perceived discrimination and refraining from seeking required medical treatment. We hypothesised that perceived discrimination interacts with socioeconomic disadvantage to increase the odds of refraining from seeking medical treatment.
METHODS
Study population
Data from the Swedish National Survey of Public Health 2004 were used for analyses. This survey was carried out by Statistics Sweden in collaboration with a number of healthcare regions and county councils in Sweden, and with the coordination of the Swedish National Institute of Public Health, Stockholm, Sweden. The total study population comprised a randomly selected sample of 33 328 individuals (15 406 men and 17 922 women) aged 18–84 years. In Sweden healthcare fees are subsidised by the state, and are waived for people under 21 years. Therefore people under 21 years were not included in the analyses. In total, we investigated 14 736 men (mean (SD) age 52 (17) years) and 17 115 women (mean (SD) age 51 (17) years).
Collection of data
Data were collected within a 3-month period during spring 2004, and was based on a postal self-administered questionnaire linked to the registry data from Statistics Sweden. The response rate was 63%. Among those who did not respond, 1.9% of the questionnaires were returned due to wrong address or protected address, 0.7% could not participate because of various reasons, 1.1% declined, 0.6% returned empty (uncompleted) questionnaires, 0.5% of the questionnaires were completed by the wrong person and the rest did not respond at all.
The questionnaires were scanned and a dataset was established. Data from the completed questionnaire were further controlled for errors and inconsistencies using a well-established method developed by Statistics Sweden and tested against the official registry data.18 Missing data were completed by the use of weighting procedures based on related answers from other completed questions, and by the use of weighting procedures based on calibration method developed by Statistics Sweden.17 Respondents were informed about data linkage with the registry data. This study was approved by the Department of Data Inspection, the Research Ethical Committee at the Swedish National Board of Health and Welfare (20031208) and the ethical committee at Karolinska Institutet, Stockholm, Sweden (DNR 2005/1146-31). The committees conformed to the principles embodied in the Declaration of Helsinki.
Main outcome
Refraining from seeking medical treatment was based on the question “During the past three months have you considered yourself to be in need of medical treatment but refrained from seeking it?” Alternative answers were “yes” or “no”.
Main determinants
Perceived discrimination
The main determinant, perceived discrimination, was measured in the context of unfair treatment that results in feeling of humiliation or inferiority. This measure included frequency of and reasons for discrimination, which is a modified version of Williams et al.18 Frequency of perceived discrimination was based on the question “During the past 3 months have you been treated in a way that made you feel humiliated?” Alternative answers were “no” (none), “yes, once” (some) or “yes, several times (frequent)”. Participants who experienced any form of discrimination were also asked to give one or more reasons that was/were attributed to this perceived discrimination. Alternative choices were ethnic background, sex/gender, sexual orientation, age, disability, religion, other or don’t know.
In an attempt to measure structural discrimination in this survey, we asked respondents who had reported any form of discrimination to indicate where this occurred. Alternative choices included private setting, welfare institutions, police and healthcare setting. In this paper, we focus on the discrimination experienced in healthcare setting.
Socioeconomic disadvantage
We developed a Socioeconomic Disadvantage Index (SDI), which combines several indicators of economic deprivation to broadly describe the individual’s underlying socioeconomic conditions. SDI was based on four variables: (1) being on social welfare at the moment of the survey, (2) being currently unemployed, (3) having a financial crisis (difficulties paying ordinary bills such as food or rent for the past 12 months) or (4) lacking cash reserves (difficulty to get hands on 15 000 SEK (about US$ 1800) within a week if needed). All the four binary indicators were summed up, resulting in a range of 0–4 points. SDI was categorised as “none” (if the sum was equal to 0), “mild” (if the sum was 1) and “severe” (if the sum was between 2 and 4).
Confounding factors
Age, living alone and educational level were analysed as confounding factors because these factors have been associated with perceived discrimination13 and not seeking medical treatment when needed.1
Living alone was based on family characteristics of being a lone adult in a household. Low education was defined as less than high school education (9 years of schooling). Living alone and education were potential confounders, as these were associated with both SDI and refraining from seeking medical treatment. Long-term illness was based on whether the respondent had any long-term illness, after-effects from an accident or other ailments. Long-term illness was also associated with discrimination, SDI and refraining from seeking medical treatment, thus being a potential confounder.
Statistical methods
Multilevel regression analysis
Analyses were performed using STATA V.9. We conducted three multiple logistic regression analyses to estimate the association between perceived discrimination and refraining from seeking medical treatment. In the first model we adjusted for age and in the second model we further adjusted for long-term illness, education and living alone. In these two models, perceived discrimination and SDI were entered separately. In the final model, we adjusted for variables as in model 2 and simultaneously included perceived discrimination and SDI, in order to analyse their independent effects (table 2). In the logistic regression analysis, we used the regression coefficients (standard errors) to obtain OR (95% CI).
We further quantified a possible interaction of effects between SDI and perceived discrimination by calculating the Synergy Index (SI). Calculation of SI has been recommended while studying interactions in social epidemiology.19,20 We assessed the interactions on the basis of departures from additive rates or risks, and the use of SI allowed studying interaction based on ORs from logistic models.21,22 Thus, we calculated SI and the 95% CIs using an excel sheet (available on request) developed by Hans Stenlund at the Department of Epidemiology, Umeå University, Umeå, Sweden.
RESULTS
Table 1 shows the distributions of study variables among men and women. In all, 15% of women and 13% of men reported refraining from seeking required medical treatment. Perceived discrimination was more common among women (30%) than among men (22%; table 1). Women were more likely to report gender/sex (11% vs 2%) as the main reason for perceived discrimination, whereas men were more likely to report ethnic background (6% vs 4%) and religion (2% vs 1%) as the main reasons (table 1). Women were also more likely to give unspecified reasons, whereas men were more likely not to know the reasons for discrimination.
Distributions of study variables among men and women
A dose–response association between the frequency of perceived discrimination in general and refraining from seeking medical treatment was observed among both men and women (table 2). After adjustment for age, long-term illness, education and living alone, some perceived discrimination was associated with a twofold increased odds for refraining from seeking medical treatment (OR (men) = 2.2, 95% CI 1.9 to 2.5, and OR (women) = 2.0, 95% CI 1.8 to 2.3), while frequent discrimination was associated with an over fourfold increased odds (OR (men) = 4.6, 95% CI 3.7 to 5.7, and OR (women) = 4.2, 95% CI 3.5 to 5.0; table 2). Further adjustment for SDI only reduced these odds ratios marginally (table 2).
Odds ratios (95% CI) for refraining from seeking required medical treatment in relation to perceived discrimination and socioeconomic disadvantage
A similar association was observed between SDI and refraining from seeking medical treatment (table 2). Perceived discrimination and SDI had independent associations with refraining from seeking medical treatment (table 2).
Discrimination specific to the healthcare setting was associated with increased odds for refraining from seeking medical treatment (OR (men) = 2.8, 95% CI 2.2 to 3.4 and OR (women) = 2.1, 95% CI 1.8 to 2.4). These associations remained statistically significant after further adjustment for long-term illness, educational level and living alone (table 2).
Further adjustment for country of birth minimally reduced the magnitude of the associations observed above.
Interaction effects between discrimination and socioeconomic disadvantage
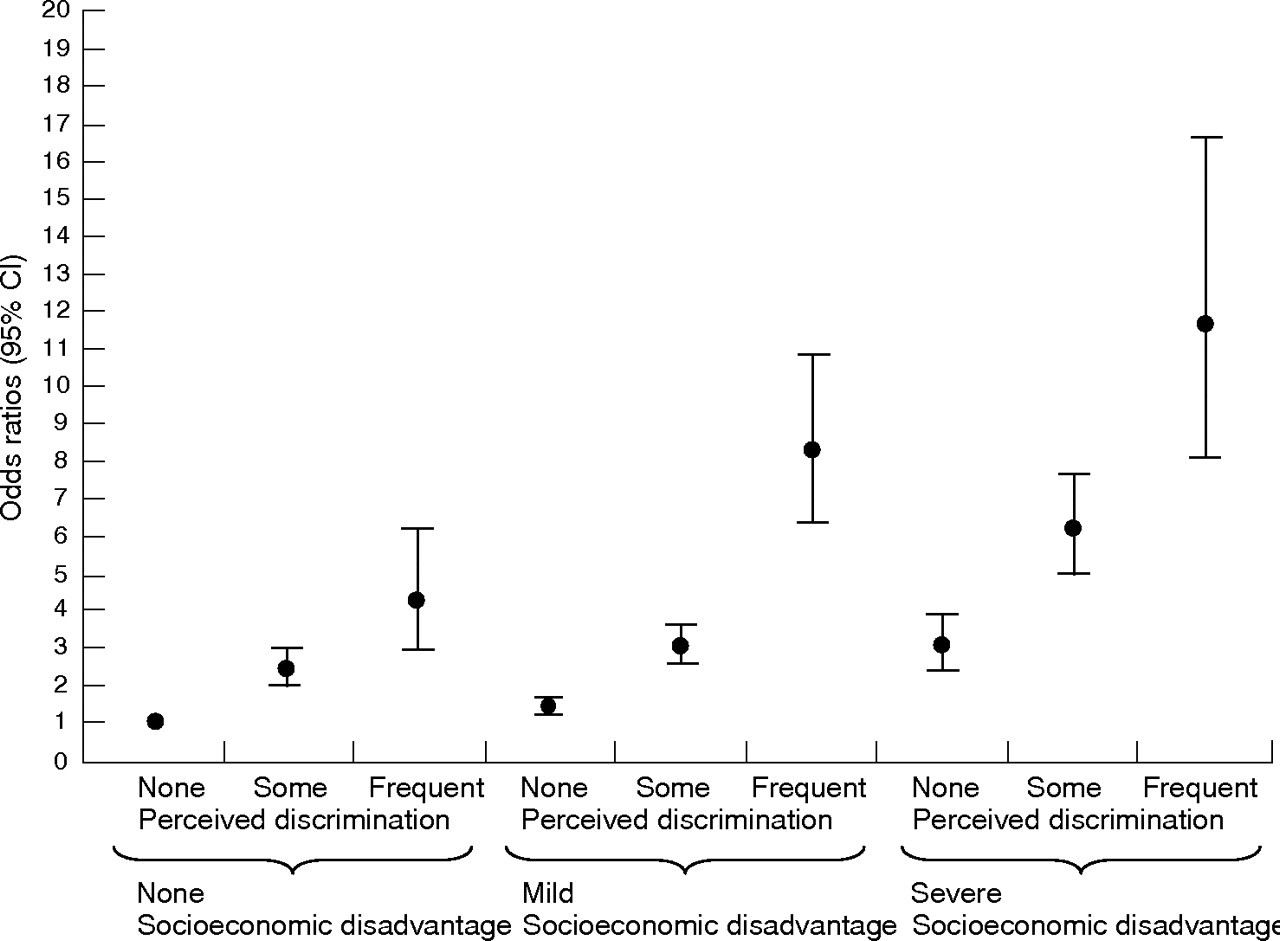
The interaction effects between perceived discrimination and SDI on refraining from seeking medical treatment, after adjustment for age, are presented in figs 1 and 2.

Interaction effects between perceived discrimination and socioeconomic disadvantage on refraining from seeking medical treatment for men (synergy index = 1.64 (95% CI 1.25 to 2.14)).

{kind=link}
{kind=link}
Interaction effects between perceived discrimination and socioeconomic disadvantage on refraining from seeking medical treatment for women (synergy index = 2.01 (95% CI 1.24 to 3.23)).
Frequent experiences of discrimination were strongly associated with refraining from seeking required medical treatment even in the absence of SDI (OR (men) = 5.6, 95% CI 3.4 to 9.1 and OR (women) = 4.2, 95% CI 2.9 to 6.1). However, experiencing both frequent discrimination and severe SDI showed a clear interactive effect on refraining from seeking medical treatment (OR (men) = 12, 95% CI 7.7 to 18.7 and OR (women) = 11.6, 95% CI 8.1 to 16.6). The SI for the interaction effects was clear in both sexes, but especially in women (SI = 2.0 (95% CI 1.2 to 3.2; fig 2)) than among men (SI = 1.6 (95% CI 1.3 to 2.1; fig 1)).
Reasons for discrimination and refraining from seeking medical treatment
Among the attributes (reasons) for perceived discrimination, we found discrimination because of ethnic/racial background (OR (men) = 2.5, 95% CI 1.8 to 3.5 and OR (women) = 2.4, 95% CI 1.7 to 3.3), age (OR (men) = 1.7, 95% CI 1.2 to 2.2 and OR (women) = 1.4, 95% CI 1.1 to 1.7), gender/sex (OR (men) = 2.4, 95% CI 1.4 to 4.2 and OR (women) = 1.6, 95% CI 1.3 to 2.0), and religion (OR (men) = 3.3, 95% CI 1.9 to 5.7 and OR (women) = 2.2, 95% CI 1.2 to 4.1) to be associated with refraining from seeking medical treatment, after adjusting for age, education, living alone and long-term illness. Further adjustment for SDI attenuated this association only marginally. Discrimination due to disability showed significant associations with refraining from seeking medical treatment among women (OR = 1.6, 95% 1.2 to 2.2), but not among men. We did not find any statistical support for the associations of discrimination due to sexual orientation or non-specified attributes with refraining from seeking medical treatment.
There were statistically significant correlations between different reasons for discrimination, but these varied with gender. Among men, discrimination because of gender was associated with that due to religion (r = 0.12), sexual orientation (r = 0.15) and age (r = 0.12), whereas discrimination because of religion was associated with ethnic discrimination (r = 0.20). Among women, age was correlated with gender discrimination (r = 0.26), whereas ethnic discrimination was correlated with religion-based discrimination (r = 0.12). We found that 16% of men and 19% of women reported at least one of these six reasons (gender, ethnic background, religion, age, disability or sexual orientation) for discrimination, whereas 3% of men and 5% of women reported two or more reasons. In relation to refraining from seeking medical treatment, we found a dose–response association with a high number of reported reasons for discrimination. Reporting one reason for discrimination was associated with OR (men) = 1.7, (95% CI 1.4 to 2.1 and OR (women) = 1.6, 95% CI 1.4 to 1.9, whereas reporting two or more reasons was associated with OR (men) = 3.2, 95% CI 2.1 to 4.7 and OR (women) = 2.3, 95% CI 1.8 to 3.0 increased odds for refraining from seeking medical treatment.
DISCUSSION
Perceived discrimination was associated with refraining from seeking medical treatment independently of age, long-term illness, low education and living alone. Perceived discrimination even in the absence of socioeconomic disadvantage was associated with threefold to ninefold increased odds for refraining from seeking medical treatment. The significant synergy effect of frequent discrimination and severe socioeconomic disadvantage on refraining from seeking medical treatment was more statistically consistent among women than among men. Perceived discrimination due to ethnicity/race, age, gender and religion was associated with refraining from seeking medical treatment. Perceived discrimination without any specified reasons was not associated with refraining from seeking medical treatment.
Results of this study support previous US findings on the association between racial discrimination and access to healthcare services.1,8,9,10,11
The fact that individuals who experienced discrimination even in a situation of favourable socioeconomic circumstances refrained from seeking medical treatment supports Sen’s23 observation that “it is not so much what one has that is important but rather what one can do with what one has”. Individuals who refrained from seeking medical treatment owing to perceived discrimination reported financial limitations and also other factors such as negative experiences in the health sector as the reason for not seeking medical treatment. We found that individuals who reported frequent discrimination were more likely to report previous negative experiences (38% vs 25% among women and 43% vs 20% among men, p<0.001) than those who did not report any discrimination.
It is worthwhile highlighting the gender differences observed in this study. Discrimination because of ethnicity/race, religion, age and gender was relevant for both men and women in relation to not seeking required medical treatment. However, discrimination because of disability was relevant only for women. This supports the recent Swedish report which demonstrated a larger number of women than men with disabilities who experienced discrimination in relation to social services.24 Additionally, the statistically significant effects of discrimination and SDI on refraining from seeking medical treatment among women (and not clearly among men), highlight the vulnerable exposures of gendered discrimination in relation to social divisions premised on power and authority.25,26 We also found that women were more likely to report discrimination because of gender (11% vs 2%) and age (10% vs 8%) than men, indicating discrimination among women based on multiple reasons. These results indicate that the predominant types of adverse discrimination based on race/ethnicity, gender and age are relevant even in egalitarian societies such as that of Sweden.
The results of this study should be interpreted in consideration of its limitations and strengths. First, the cross-sectional design of the study makes it difficult to draw conclusions on causal relationships. Second, the outcome measure (refraining from seeking required treatment) is general and examines a broad group of people, but this measure may not be equated to the professional definition of needed care. Nevertheless, we found significant associations of poor self-rated health and long-term illness with refraining from seeking required medical treatment (p<0.001). Additionally, subgroup analyses showed that the association between frequent discrimination and refraining from seeking medical treatment did not differ among healthcare users for the past 3 months (OR (men) = 5.8, 95% CI 4.4 to 7.6 and OR (women) = 5.1, 95% CI 4.1 to 6.3) compared with non-users (OR (men) = 5.8, 95% CI 4.2 to 78.0 and OR (women) = 5.5, 95% CI 4.2 to 7.4). This finding supports previously documented associations between discrimination and treatment delays after being in contact with a doctor.27 Third, the measure of discrimination based on “treatment that makes people feel humiliated” may not capture “discrimination” as a concept.28 However, we found that individuals who did not indicate any specified reasons for discrimination based on defined social constructs of ethnicity/race, religion, age, gender or disability were not more likely to refrain from seeking medical treatment than those who did not report any discrimination. We found statistically significant correlations between different reasons (types) for discrimination and a dose–response association between increasing number of reported reasons and refraining from seeking medical treatment. These findings indicate clustering of multiple types of discrimination in some individuals that may influence their decisions of seeking medical treatment. In fact, we observed that individuals who indicated unspecified reasons gave examples such as their looks, style or attitude as reasons for discrimination. We also found that socioeconomic disadvantage was not associated with indicating “other” unspecified reasons (p = 0.10) or not knowing the reason(s) for discrimination (p = 0.55). Fourth, the non-response rate was 37% and included a large proportion of men, socially disadvantaged individuals and inhabitants in metropolitan areas. Thus, results presented here are probably an underestimation of the magnitude of true effects between discrimination and refraining from seeking medical treatment.
Fifth, because healthcare management and administration takes place at county council level, hypothetically this level may affect the individual probability of refraining from seeking medical treatment. However, we also ran multilevel logistic regression analysis29 with individuals at the first level, municipalities at the second level and counties at the third level, and found that the municipality-level and especially the county-level components of variance were very small (ie, very close to 0) in both men and women. The ORs for the associations between the individual variables and refraining from seeking medical treatment from multilevel regression analyses were almost identical to those obtained by single-level logistic regression that did not consider the county and municipality levels (table available from authors on request).
The strengths of this study include the use of a large dataset that represents the normal population, and a generic measure of perceived discrimination addressing all groups in Swedish society. In addition, as recommended previously,18 the major social constructs, race/ethnicity, religion, gender/sex, disability, age and sexual orientation were specifically addressed as reasons for perceived discrimination. According to our knowledge, this is the first European study where the association between perceived discrimination and refraining from seeking required medical treatment are analysed simultaneously with socioeconomic disadvantage in a large population-based sample.
We developed the SDI that includes economic hardships, position in the labour market and being unable to economically support oneself, which reflects both material standards and a broad perspective on socioeconomic circumstances. We have validated the SDI measure and found moderate internal reliability.30 We also found consistently significant associations between SDI and lack of access to dental care services independent of educational and occupational status. Thus, this index seems to indicate substantial policy implications and reflects a broader understanding of one’s socioeconomic circumstances than using single measures of socioeconomic position, which has recently been criticised in health research.31,32
The fact that individuals who experienced both discrimination and socioeconomic disadvantage had the largest odds for refraining from seeking required medical treatment raises key equity issues in health policies in Sweden.33 This is because the Swedish healthcare system is almost entirely publicly financed and delivered on the basis of equity principles of “care on equal terms”.34 Findings on statistically significant associations between general perceived discrimination and discrimination specific to healthcare setting and refraining from seeking required medical treatment have implications on policies and strategies geared towards minimising discrimination. Results suggest that discrimination occurring at micro and macro levels in the Swedish society seem to influence people’s choices for seeking medical treatment, which may cause worsen health in the long run. As demonstrated previously, discrimination is associated with choices regarding seeking care and also with treatment delays, partly due to the lack of trust in healthcare.27
The findings in this study call for a public health strategy that highlights and tackles perceived discrimination in order to enhance equitable access to medical treatment and other healthcare services.4,6,35,36 Thus, society-wide interventions to counteract bias, prejudice and unfair treatment in society are needed. In addition, healthcare-specific interventions such as training of healthcare providers and inclusion of ethics training focusing on social justice and human rights in medical and nursing training curriculum would be useful.27,36–39
What is already known
-
Access to healthcare services, including access to medical treatment, has been documented to vary according to socioeconomic position, gender and race/ethnicity.
-
The interaction between perceived discrimination and socioeconomic disadvantages have not been investigated.
What this paper adds
-
This is the first national population-based study to show associations of both perceived discrimination and socioeconomic disadvantage with refraining from seeking medical treatment.
-
Perceived discrimination even in the absence of socioeconomic disadvantage was associated with refraining from seeking required medical treatment.
-
Particularly for women, the combination of both discrimination and socioeconomic disadvantage resulted in a much stronger effect on refraining from seeking medical treatment than the simple sum of their independent effects.
Policy implications
-
Strategies to counteract bias, prejudice and unfair treatment in society, in particular within the healthcare setting, are needed.
-
The goal towards equitable access to healthcare services cannot be achieved without specific public health strategies that confront and tackle discrimination, particularly in the healthcare setting.
In conclusion, perceived discrimination is associated with refraining from seeking required medical treatment independent of socioeconomic resources. The goal towards “care on equal terms” cannot be achieved without specific public health strategies that confront and tackle discrimination in society and specifically in a healthcare setting.
Acknowledgments
We thank Karin Nykvist for her excellent assistance with the administration of the survey and data collection, and Dr Lars Sundman, Samhällsmedicin Gävleborg, for his expertise with the instrument to measure access to healthcare services. We also thank the county councils of Gävleborg, Dalarna, Kronoberg, Kalmar, Blekinge, Jönköping, Halland, the region of Västra Götaland and the municipality of Gotland for making this survey possible. We are indebted to Dr Gunnar Ågren, the National Institute of Public Health and Statistics Sweden, for carrying out this survey. We are grateful to the reviewers (Dr Courtney Harold Van Houtven and anonymous) for their excellent review that improved the paper substantially.
REFERENCES
Footnotes
-
Competing interests: None.
Linked Articles
- In this issue