Article Text

Abstract
Study objective: To estimate the relative health effects of the income and health insurance provisions of the Los Angeles City living wage ordinance.
Setting and participants: About 10 000 employees of city contractors are subject to the Los Angeles City living wage ordinance, which establishes an annually adjusted minimum wage ($7.99 per hour in July 2002) and requires employers to contribute $1.25 per hour worked towards employees’ health insurance, or, if health insurance is not provided, to add this amount to wages.
Design: As part of a comprehensive health impact assessment (HIA), we used estimates of the effects of health insurance and income on mortality from the published literature to construct a model to estimate and compare potential reductions in mortality attributable to the increases in wage and changes in health insurance status among workers covered by the Los Angeles City living wage ordinance.
Results: The model predicts that the ordinance currently reduces mortality by 1.4 deaths per year per 10 000 workers at a cost of $27.5 million per death prevented. If the ordinance were modified so that all uninsured workers received health insurance, mortality would be reduced by eight deaths per year per 10 000 workers at a cost of $3.4 million per death prevented.
Conclusions: The health insurance provisions of the ordinance have the potential to benefit the health of covered workers far more cost effectively than the wage provisions of the ordinance. This analytical model can be adapted and used in other health impact assessments of related policy actions that might affect either income or access to health insurance in the affected population.
- health impact assessment
- wage policy
- health insurance
Statistics from Altmetric.com
Since the mid-1990s, over 100 cities and counties in the USA have passed “living wage” ordinances.1 Living wage ordinances typically cover a defined group of workers, such as employees of firms that work on municipal contracts, lease municipal property, or receive grants from local government. An increasing number of living wage ordinances include provisions for health insurance coverage or additional monetary compensation in lieu of health insurance.
We sought to estimate potential reductions in mortality attributable to different combinations of wage and health insurance benefits for the City of Los Angeles’ living wage ordinance as part of a larger comprehensive health impact assessment (HIA) of this ordinance. While a number of studies have examined the economic effects of living wage laws,2–7 only two focused on the health related effects of these ordinances. Pourat and Wallace sought to identify rates of health insurance among workers covered by the Los Angeles City ordinance.8 Bhatia and Katz modelled changes in mortality risk attributable to wage increases for workers covered by San Francisco’s living wage ordinance.9 Neither study estimated changes in health outcomes or compared the two important types of benefits provided by living wage laws—increased income and health insurance coverage.
This quantitative approach to HIA, which applies risk estimates from the epidemiological literature to make predictive estimates of health outcomes, also stands apart from most examples of HIA. Over the past half decade interest has grown rapidly in HIA.10 Much progress has been made in outlining the general principles and protocols for HIA.10–15 While any HIA may use an assortment of approaches, most are descriptive and largely qualitative. Only a handful of examples9,16–21 use what Kemm describes as a “tight” approach to HIA11—the type of evidence based quantitative, predictive analysis that Mindell et al suggest is often particularly convincing to policy makers.22
Los Angeles City living wage ordinance
Approved by the Los Angeles City Council in 1997, the City of Los Angeles’ living wage ordinance sets an annually adjusted minimum wage that city contractors must pay employees working on city service contracts and economic development grants. As of July 2002, the ordinance mandated that employers pay covered workers at least $7.99 per hour and contribute at least $1.25 per hour worked toward health insurance premiums or, alternatively, increase direct pay an additional $1.25 per hour. Automatic annual cost of living increases are required for wages, but the $1.25 per hour for health insurance has been fixed since ordinance passage. The ordinance also requires employers to provide covered employees with at least 12 annual paid days off.
PATHWAYS OF POTENTIAL HEALTH EFFECTS—INCOME AND HEALTH INSURANCE
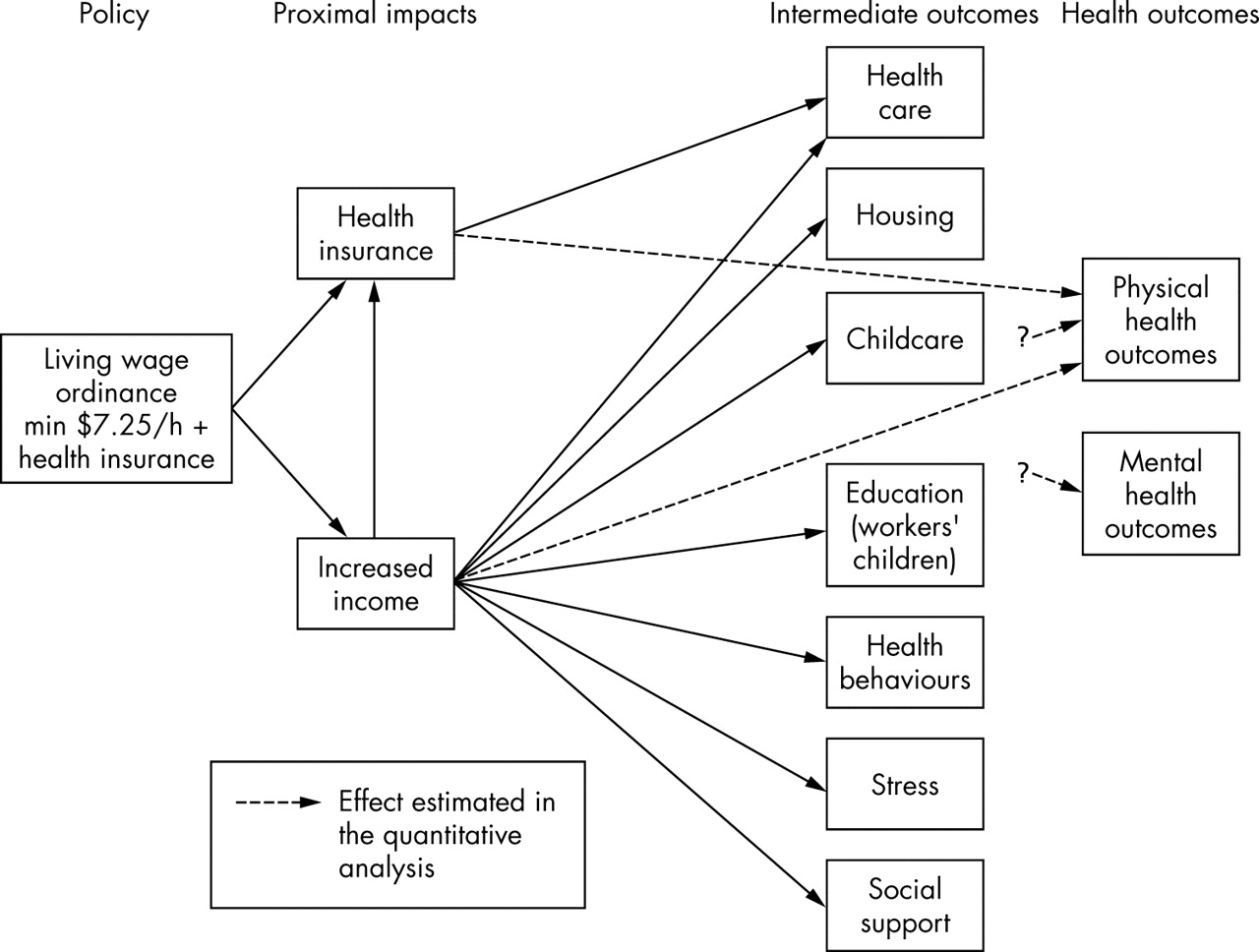
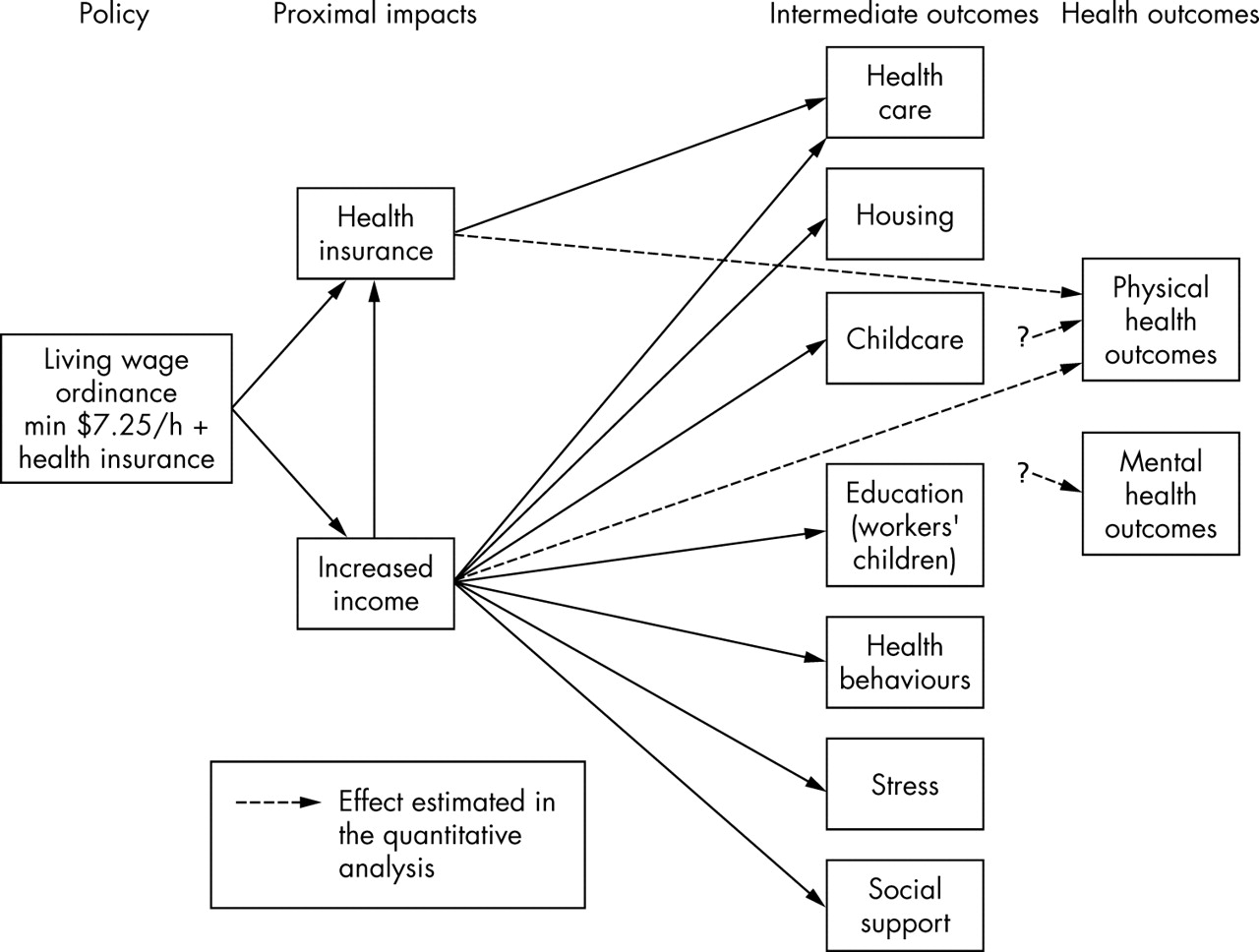
We diagrammed the putative causal relations suggested by the relevant economic and health research to form a logic framework for the analysis (see fig 1), much as that done by Joffe and Mindell23 and Anderson et al.24 While the comprehensive HIA, which included both quantitative and qualitative analyses, investigated each of the pathways and effects on such determinants of health as health care, housing, and childcare, the quantitative analysis presented here did not specify the specific pathways through which income and health insurance benefits affected mortality.
{kind=link}
The logic framework for the analysis of the health impacts of the Los Angeles City living wage ordinance
Health effects related to paid leave, another employment benefit mandated by the ordinance, were not considered in the analysis because of a lack of information about current time off benefits and ambiguity about the number of workers covered by this part of the ordinance. Also excluded from the analysis were macroeconomic effects, such as unemployment, inflation, or collateral wage increases, and secondary effects on city agencies or employers, such as changes in rates of municipal outsourcing. Although such effects could occur and affect health, economic analyses of this and similar living wage ordinances show that these effects are likely to be small,2,6 primarily because of the narrow targeting of most living wage ordinances—workers subject to the Los Angeles ordinance comprise just over two tenths of one per cent of the estimated 4.7 million jobs in Los Angeles County.25 Furthermore, affected employers seem to pass on additional labour costs to the city.26
METHODS
To compare the health impact, defined as changes in mortality, stemming from the ordinance’s changes in wage and health insurance benefits, we generated a series of scenarios of different combinations of wage and health insurance benefits, for which effect estimates from the literature were used to estimate mortality changes in a hypothetical cohort of targeted workers. The cost effectiveness of each scenario was subsequently calculated based on the impact on mortality and associated costs.
Mortality as outcome of interest
We focused our analysis on mortality because mortality is an objective measure that can easily be compared between studies and populations, and data were available that permitted the quantification of linkages between the policy and mortality. Comparisons in our analysis were facilitated by the fact that two key studies, one examining the association between income and mortality27 and the other examining the association between health insurance and mortality28 used the same dataset—the national longitudinal mortality study (NLMS), a long term prospective study of mortality in the USA from 1979 to 1989 among 1.3 million persons ages 25 to 64 years.25
Other benefit scenarios were also considered, including the proportion of uninsured to be insured and increased health insurance compensation to bring it more in line with the actual cost of health insurance, an average of $1.59 per hour for single coverage.32
Effect estimation
To estimate the effects of income on mortality, we used Backlund et al’s findings from their analysis of NLMS data—a 1.21 relative mortality risk for each decrease of $21 832 in income below a threshold of $49 096 (2002 dollars).27 For income above this threshold, Backlund et al estimated a much weaker effect (relative risk of 1.07 for each decrease of $21 832 in income). Assuming covered Los Angeles worker’s incomes are similar to workers in neighbouring Santa Monica studied by Pollin and Brenner,5 their average gross household income was about $28 000 per year.
Two similar estimates of the effect of health insurance on mortality were identified. Franks et al30 estimated a mortality hazard (rate) ratio of 1.25 for uninsured compared with insured adults over age 25 in the national health and nutrition examination survey (NHANES) I cohort, controlling for health status at baseline, socioeconomic status (SES), and a variety of demographic factors. Sorlie et al,28 who like Backlund et al analysed NLMS data,27 reported relative risks of mortality of 1.2 to 1.3, depending on race and sex, for the uninsured compared with those with employer provided insurance, controlling for age and income. As NLMS study participants were all working and under age 65 at baseline, this study population is more similar to the cohort of living wage workers than the NHANES sample,30 which included both employed and unemployed persons.. As most living wage workers are male,5 we used the relative risk estimate Sorlie et al reported for white men—1.3, for the entire population.26
Defining the target population and baseline assumptions
About 10 000 workers are covered by either the wage or health insurance provisions of the ordinance.7 Additional workers may be indirectly affected by the ordinance, but previous economic analyses of the ordinance suggest their numbers are small.2,6
We assumed a wage distribution at baseline similar to findings of Pollin and Brenner’s analysis of data from the current population survey (CPS) for low income workers in Los Angeles.5 They found that in 2000 58% of workers earned the prevailing state minimum wage, 25% earned on average one dollar per hour over the minimum wage, and 17% earned on average two dollars per hour over the minimum wage. Adjusting for a subsequent increase in the state minimum wage yields the wage distribution shown in table 1: 58% of living wage workers earning an average of $6.75 per hour, 25% earning an average of $7.75 per hour, and 17% earning an average of $8.75 per hour.
Assumed distribution of wages and health insurance at baseline for the estimated 10000 workers subject to the Los Angeles living wage ordinance
Studies using different methods2,7,8 have estimated that 40% of affected workers already had employer provided health insurance. Data from the California health interview survey suggest that the two dollar per hour wage gap within segments of this study population is unlikely to be associated with significant differences in heath insurance coverage.31 We therefore assumed uniform insurance coverage rates for all three wage groups.
Selection of alternative scenarios
We compared the effects of five alternative scenarios based on different combinations of wage and health insurance benefits (table 2). Scenario 3 represents the current ordinance. While compensation in scenario 4 exceeds the minimum required by the ordinance, it reduces potential distortion of wage structures between the insured and uninsured.
Wage and health insurance benefit scenarios
Calculations
The net effect of each scenario on mortality was estimated by summing stratum specific effect estimates for different combinations of wage and insurance benefits for the six groups defined by baseline wage (three categories: $6.75/h, $7.75/h, $8.75/h) and insurance status (two categories: insured, uninsured) shown in table 4. With three categories of possible benefits—additional wages, health insurance, and monetary compensation in lieu of health insurance—this yielded 18 possible strata. As two strata had zero persons, only the remaining 16 strata are shown in table 4. The stratum specific changes in mortality were derived by applying stratum specific effect estimates generated for each combination of benefits using the published findings for income26 and health insurance.28 Details beyond the general procedure outlined below are available at the UCLA School of Public Health web site (http://www.ph.ucla.edu/hs/health-impact). Cost effectiveness ratios (cost of each intervention scenario per death prevented) were based on the estimates of effect on mortality and associated costs of increasing wage and affording health insurance benefits to workers under the ordinance.
RESULTS: COMPARISON OF ESTIMATED EFFECTS
The effect of increased wages (income)
Establishing a minimum wage of $7.99 for covered workers would increase workers’ average wage earnings by $1403 per year, assuming 1800 hours of work annually, and would lead to a reduction of 0.68 deaths per year (scenario 1). Monetary compensation in lieu of health insurance would effectively increase the hourly wage by an additional $1.25 per hour, yielding a reduction of 1.4 deaths per 10 000 workers per year if additional compensation is paid only to workers who remain uninsured (scenario 3), or 1.65 deaths per year if the additional $1.25 per hour is paid to all workers (scenario 4).
The effect of additional health insurance coverage
Although the ordinance has not led to increased health insurance coverage, we estimated the effect of hypothetical coverage increases. Providing insurance to 25% of uninsured workers leads to a reduction of 1.91 deaths per 10 000 workers per year (table 3). Increasing coverage to 50% of the uninsured leads to 3.81 fewer annual deaths. Providing health insurance to all of the uninsured (scenario 2) reduces deaths by 7.63 per year—a decrease 11 times greater than the decrease attributable to the ordinance’s wage provisions alone (scenario 1). Wages would have to be increased to $15.97 per hour to produce this same reduction in mortality.
Estimated lives saved per year among 10000 workers under three levels of additional health insurance coverage
Cost effectiveness
Providing health insurance is also more cost effective than providing monetary benefits (table 4). If all uninsured workers received health insurance under the ordinance (scenario 5), the ordinance would save an additional 6.65 lives per 10 000 workers per year for no additional costs compared with the current ordinance (scenario 3). While prevention of one death under the current ordinance (scenario 3) costs about $19.7 million in direct costs, providing health insurance to all of the uninsured (scenario 5) costs $3.4 million per death prevented.
Cost effectiveness of alternative benefit scenarios
Policy implications
Despite the limitations, this study offers good evidence for the large potential of health insurance to benefit the health of living wage workers, and health benefits are more cost effective than equivalent wage increments.
Sensitivity analysis
While the two studies from which the effect estimates are derived are methodologically sound, the absence of confirmatory studies limits confidence in these estimates. Furthermore, the income effect may be overestimated as Sorlie et al’s study on the effect of health insurance controlled for income,28 but Backlund et al’s study on the effect of income did not control for health insurance status.27
For a sensitivity analysis of these two effect estimates used in the model, we examined alternative values that would produce equivalent reductions in mortality. Even if the true value of the effect of income was as high as 1.5 and the effect of insurance was as low as 1.1, providing health insurance would still produce a greater reduction in mortality than additional income.
DISCUSSION
The mandated wage level of $7.99 per hour plus another $1.25 per hour in lieu of health insurance yields only $4482 in increased annual gross income—about $2947 after taxes. This additional income from the ordinance yields 1.4 fewer deaths per year among the 10 000 covered workers. Limited data availability and project resources limited our quantitative analysis to mortality effects. Additional income could affect not only mortality, but physical and mental morbidity, hospitalisation, sick days, and quality of life. Insuring the 60% of workers subject to the ordinance but currently uninsured (scenario 5) would produce a reduction in mortality nearly six times larger than the effect of additional income from the ordinance (scenario 3) at no additional cost. Providing health insurance to all the workers covered by the ordinance costs about $3.4 million per death averted—on the same order as the value of $3 million per statistical life found by Viscusi in his review of “willingness to pay” in the early 1990s.33
What this paper adds
We believe this paper represents an important contribution to the understanding of how government policies outside the purview of health departments may influence the public’s health, and serves as an example of how existing epidemiological evidence can be used in quantitative, predictive models for health impact assessment.
Limitations
The estimated reductions in mortality attributed to expanded health insurance coverage and income gains are expected to occur over many years. Short term health and quality of life benefits are also likely, but difficult to estimate from available data. Our estimates do not take into account impacts on workers’ spouses and children. With a mean family size of 3.8 in the target population,5 family health insurance coverage could magnify estimated benefits; however, the ordinance mandated health insurance benefit of $1.25 per hour is insufficient, even to cover health insurance premium costs for an individual policy. Also the ordinance will have limited impact on child dependants, most of who probably qualify for California’s state subsidised insurance programme for low income families.
In the absence of findings from well designed intervention trials, we extrapolated from the results of observational studies, the results of which may be distorted by selection bias, confounding, misclassification bias, and reverse causality.34–36 Also, comparisons between categories in observational studies may capture fundamentally different phenomena than intervention induced changes. For example, low income households may use an additional amount of income differently than middle income households. Another limitation is that we were not able to take into consideration the cumulative effects of changing income or insurance coverage over long periods and how such effects are modified by previous periods of deprivation.37–39
In addition to assumptions about the effect estimates used, the model rests on two additional assumptions. Firstly, the effects of health insurance and income are assumed to be multiplicative—that is health insurance and income have the same effect across different levels of income, and that income has the same effect for both the insured and uninsured. Secondly, changes in income and health insurance are assumed to be permanent.
Conclusion
Despite the limitations, this study offers good evidence for the large potential of health insurance to benefit the health of living wage workers, and that health benefits are more cost effective than equivalent wage increments. Although the health of workers and their families is not the only goal of the ordinance, it is an important consideration. Study results strongly suggest that raising health insurance coverage rates through the living wage ordinance can be a crucial step towards achieving this goal. However, coverage rates have remained at about 40% from just before ordinance passage in 1997 to mid-2003. Increasing the required level of health insurance premium payments, unchanged since 1997, creating health insurance purchasing pools, increasing the mandated level of cash in lieu of insurance payments to relate to actual increases in health insurance costs, or mandating health insurance coverage could improve the health protection benefits of the ordinance.
The study methods provide a valuable tool for other health impact assessments. While our analysis excludes a number of health effects, evidence based, quantitative projections such as the ones generated here can be a valuable part of a comprehensive HIA. Furthermore, our analytical model can be adapted to examine the effects of a wide array of policy actions that might affect either income or access to health insurance in the affected population, such as wage policies, tax reform, siting of new centres of employment, and health insurance coverage requirements. As data become available, the model can also be expanded beyond mortality to include other health outcomes such as functional status and quality of life.
Acknowledgments
Our thanks to Ms Rachel Golick for assistance in document preparation.
REFERENCES
Supplementary materials
The appendix is available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [view PDF] - Appendix 1: Calculating reductions in mortality attributable to the Los Angeles City Living Wage Ordinance.
Footnotes
-
Funding: this study was supported by a contract with the Washington DC based Partnership for Prevention with funding from the Robert Wood Johnson Foundation.
-
Conflicts of interest: none declared.
-
Ethics approval: this study relied exclusively on previously published data. Human subjects research approval by the institutional review board was not necessary, as no human subjects were contacted, nor were any individual level data with potential identifiers used in the analysis.
Linked Articles
- In this issue