Article Text

Abstract
Study objective: The UK government called for a 40% reduction in cardiovascular disease mortality in those aged under 75 by 2010. This paper examines the potential for cardiovascular risk factor changes to reduce coronary heart disease deaths in Scotland, and then extrapolates the findings to the UK population.
Design: Secondary analysis of published data using a previously validated mortality model. The model combines uptake and effectiveness of treatments with risk factor trends by sex and age group. It was used to estimate the expected reductions in coronary heart disease mortality: (a) if recent risk factor trends simply continued; (b) if additional risk factor reductions were achieved in line with Scandinavia and the United States. An “analysis of extremes” sensitivity analysis was then carried out.
Setting: Scotland and UK.
Participants: Projected Scottish population aged 45+ in 2010 (2.4 million) and UK population of 26.8 million.
Main results: Continuation of current trends would result in 2169 fewer coronary deaths in 2010 (minimum estimate 1191 from sensitivity analyses to maximum 3870). About 4749 fewer deaths (minimum 3085, maximum 7155) could be achieved by: (a) a reduction in smoking prevalence from 30% to 18% (about 1668 fewer deaths); (b) a mean population cholesterol reduction from 6.2 to 5.2 mmol/l (about 2167 fewer deaths); (c) a 3.7 mm Hg fall in diastolic blood pressure (about 914 fewer deaths). Extrapolation from the Scottish population to the UK suggests 24 000 fewer deaths in 2010 if current trends continue, or 53 000 fewer deaths with the additional reductions.
Conclusions: With additional interventions it would be possible to almost halve current UK coronary heart disease mortality. Even without gains from medical treatments, the UK government target of 28 000 fewer deaths in 2010 does not seem challenging.
- coronary heart disease
- epidemiological modelling
- risk factors
Statistics from Altmetric.com
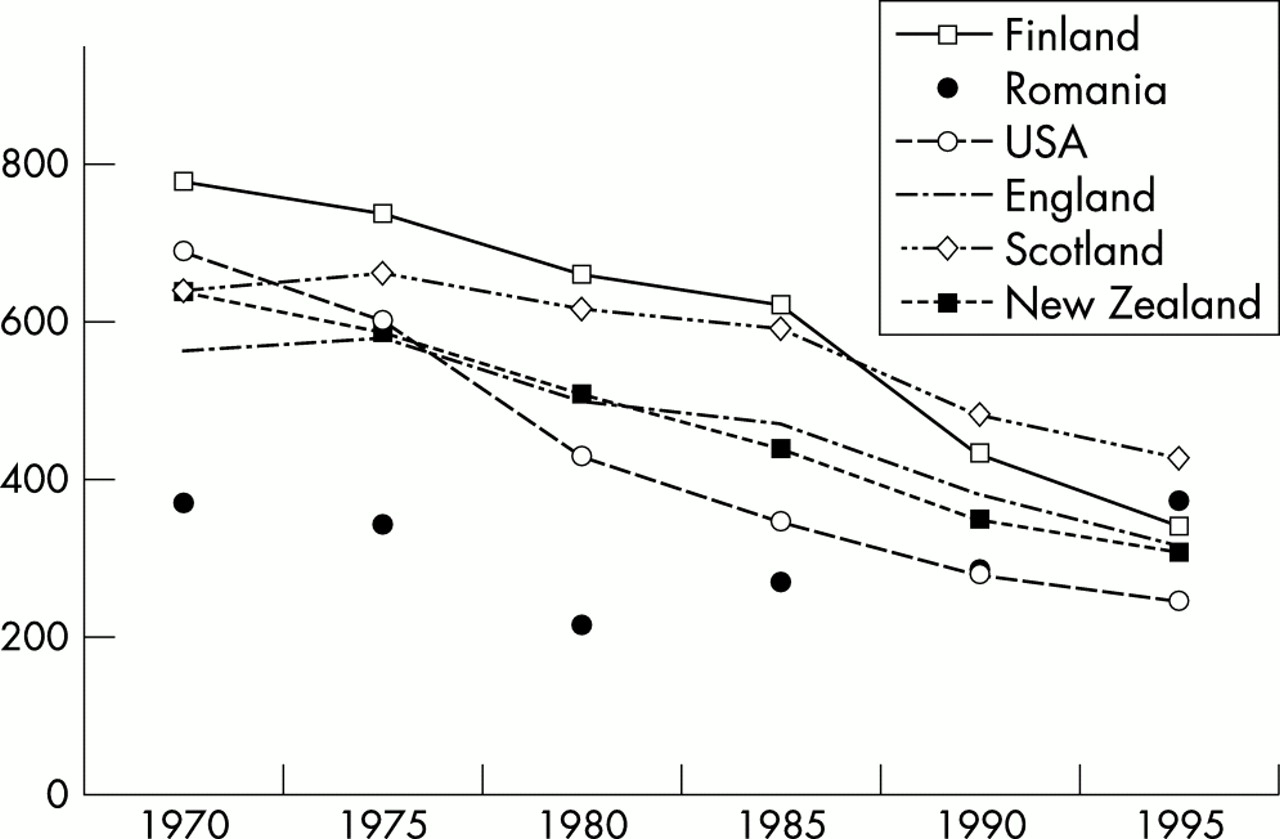
Coronary heart disease mortality rates have halved in most industrialised countries since the 1970s (fig 1). However, mortality has declined less in the UK, and coronary heart disease remains the single largest cause of death.1 The UK government recently endorsed cardiovascular disease as a top priority, and the Saving Lives white paper set the target of 200 000 fewer coronary heart disease deaths by 2010 (with 28 000 fewer in the year 2010).1
{kind=link}
International trends in age standardised coronary heart disease mortality in men aged 35–74 between 1979 and 1995 (WHO statistics, 1998).
It is thus vital to explain the observed declines in coronary mortality, and evaluate the potential for further reductions. Large long term cohorts, such as the Framingham study2 and the British Regional Heart Study3 have shown substantial reductions in coronary heart disease risk from changes in major risk factors, such as smoking, blood pressure, and cholesterol.
Attributing falls in mortality to specific risk factor changes or effective medical interventions such as aspirin,4 and β blockers,5 is difficult because favourable trends in both have occurred simultaneously. Furthermore, risk factor changes such as cholesterol lowering may be achieved through “lifestyle” change or pharmacologically.6 In 1996, Capewell et al developed and refined a Scottish coronary heart disease mortality model,7 which combined data from multiple sources on patient numbers, treatment effectiveness, and risk factor trends. Analysing the observed fall of 6747 deaths between 1975 and 1994, about 60% was attributed to changes in major risk factors and 40% to specific cardiological treatments. The estimates were validated against the actual mortality falls observed, and replicated, using independent data in New Zealand.8 Despite different settings, timescales, and methodologies, models suggest that reductions in major risk factors account for over half the observed mortality declines, and treatments just under half.9–11
This study builds on earlier work in Scotland. Having incorporated more recent and robust coefficients relating changes in population risk factor levels and coronary heart disease mortality rates,12 we now extend the model to estimate the number of deaths that could be prevented or postponed between 1994 and 2010. Initially, by simply assuming that risk factors continue to decline at their current rates, and then by assuming larger but feasible risk factor reductions. These results are then applied to the UK population to estimate the potential mortality reductions achievable.
METHODS
The model uses regression coefficients estimated from large cohort studies and MONICA analyses7,12–15 to describe the relation between population changes in specific cardiovascular risk factors, and population mortality rates from coronary heart disease. For each major risk factor, the subsequent reduction in deaths is estimated as the product of the specific regression coefficient, the relative risk factor reduction, and the number of coronary heart disease deaths observed at the beginning of the time period of interest. The coefficients were decreased for older age groups to reflect the epidemiological evidence suggesting that relative risk attenuates with age15,16 (appendices 1 and 2, see journal web site).
Extension of the model to 2010
The refined model was extended from 1975 through 1994 to the year 2010, using deaths and population size by sex and age group for Scotland annually from 1986 to 1998,17 and projected population estimates to 2010. The “baseline” deaths expected in 2010 were calculated by applying the age specific death rates in 1994 to the 2010 projected population. Projected death rates from coronary heart disease in 2010 were then estimated by extrapolating current trends to the year 2010 using five year rolling averages.
(1) Current trends in risk factors between 1994 and 2010
We firstly assumed that the average annual trends in total cholesterol and blood pressure observed in the Glasgow MONICA population12 between 1986 and 1995, continued until 2010 and extrapolated to the wider Scottish population. Trends in smoking prevalence were estimated using Scottish data from the General Household Survey.18,19 Only limited information was available for those aged over 65; where necessary it was assumed that risk factor reductions were only 50% of those seen in younger age groups.
(2) Additional reductions in risk factors between 1994 and 2010
The calculations were then repeated assuming greater risk factor reductions. Realistic and feasible risk reductions were chosen, based on data from comparable populations.
(a) Smoking
The UK target to reduce smoking prevalence to 24% among adults by 2010 does not seem challenging,20 and may be achieved simply on the basis of current trends. In contrast, the US Healthy People 2010 smoking prevalence target of 12% by 201021 seems demanding, and for Scotland between 1994 and 2010 would require a 60% relative reduction in smoking prevalence. A more realistic compromise, smoking prevalence of 18% in 2010 in all ages under 75, was therefore chosen. Smoking prevalences are already lower than 18% among people aged over 65 in the UK.22
(b) Cholesterol
Reductions in population mean cholesterol levels have been modest in Scotland; less than 5% in men and women aged 45–64 between 1985–94.12 The annual relative falls of 1% in men and 1.4% in women observed in Gothenberg, Sweden12 (another Northern Europe population) were therefore applied to the Scottish population (target levels for 2010 would then resemble those observed in the 1990s in populations such as Gothenberg, Stanford, USA and Perth, Australia12).
(c) Blood pressure
Finally, an additional 3.7 mm Hg decrease in population mean diastolic blood pressure between 1994 and 2010 was tested. Such falls have been observed in several countries within the MONICA study.12
Sensitivity analysis
Because of the uncertainties surrounding some values, an analysis of extremes23,24 sensitivity analysis was performed.24 Estimated mortality reductions were generated using minimum and maximum plausible values for the main parameters8 (appendix 2).
RESULTS
Trends observed in Scotland, 1986–1998
Overall annual declines in coronary heart disease mortality rates were 2.6% in men, and 2.2% in women, ranging from 5% in the younger age groups to 1% in women aged over 85.
Estimated changes in coronary heart disease mortality in Scotland between 1994 and 2010
Assuming that current trends in age specific death rates continued to 2010, 11 287 deaths would be expected in 2010 (6048 among men, 5239 in women, overall reductions of 39% and 32% respectively from 1994). The estimated age specific percentage declines between 1998 (the most recent year for which data were available) and 2010 in those aged 45–54, 55–64 and 65–74 would be 46%, 42%, and 36% in men and 45%, 40%, and 32% in women respectively.
Cardiovascular risk factor changes
(a) Based on current trends only
Projections of current risk factor trends suggest that 2169 deaths would be prevented or postponed in 2010 as a result of the reductions since 1994 (minimum estimate from sensitivity analyses 1191, maximum 3870, table 1). These 2169 fewer deaths would result from 937 attributable to falling trends in smoking (from a population prevalence of 30% to 21%), 774 attributable to a reduction in cholesterol (from 6.3 mmol/l to 5.8 mmol/l among under 65s), and 459 attributable to falls in population diastolic blood pressure (from 76 mm Hg to 73 mm Hg among under 65s, tables 1 and 2).
Contribution of changes in population risk factors to the projected fall in coronary heart disease mortality in Scotland between 1994 and 2010. (1) Current trend assuming that risk factors continue to fall at same relative rates, (2) assuming additional reductions
Risk factor levels at 1994 baseline and projections to 2010, for men and women aged 45–65 years
(b) Additional reductions in major risk factors (tables 1 and 2)
A total of about 4749 deaths (minimum 3085, maximum 7155) could be prevented or postponed by additional but feasible reductions in the major cardiovascular risk factors.
1668 fewer deaths assuming that smoking prevalence fell to 18%;
2167 fewer deaths assuming that population mean cholesterol levels declined as in Gothenburg, Sweden (by 2010 reaching 5.2 mmol/l among men, and 5.1 mmol/l among women under 65);
914 fewer deaths assuming an average further decrease in mean diastolic blood pressure of 3.7 mm Hg across all age and sex groups (from 76 mm Hg to 69 mm Hg among those aged under 65).
The number of deaths prevented or postponed in 2010 due to these additional risk factor changes could thus be increased more than twofold from 2169 if current trends continue, to 4749 (table 1). The absolute risk factor levels that would be achieved in 2010 are detailed in table 2.
In women, much of the benefit would occur among older age groups, whereas in men benefits would be more evenly distributed (table 3).
Reduction in CHD mortality achievable in 2010 with (1) current risk factor trends and (2) additional risk factor reductions: distribution by age and sex
Comparison with UK targets and extrapolation to the UK population
The UK target calls for a 40% reduction in coronary mortality, with 28 000 lives to be saved in 2010.1 Simple extrapolation from the Scottish model estimates (4749 lives saved with additional risk factor interventions in a population of 2.4 million) to the UK population of 26.8 million suggests that 53 000 lives could be saved in the year 2010. Conservatively assuming that 60% of these (32 000) are in the target age groups (<75), it seems that the 28 000 target could be met entirely through risk factor changes. Furthermore, substantial improvements in treatment efficacy and uptake are also expected.25
DISCUSSION
Over 50 000 coronary deaths could be prevented or postponed in 2010 in the UK with the additional risk factor reductions. This would represent almost half the 110 000 current annual cardiac deaths in the UK.26 Over 60% of the reduction would occur in the premature deaths aged under 75 specified in government targets. Most of the reduction would be seen among men, because of the lower mortality rates among younger women. Simple extrapolation of current mortality trends suggests that the UK target is not testing.27
To date, the biggest mortality benefits have come from reductions in smoking,7 as elsewhere in Europe, the US, and New Zealand.7–11,16 However, reductions in cholesterol seem to have even greater potential to further reduce coronary heart disease mortality rates in the UK and elsewhere. Past falls have been modest, and cholesterol levels in Britain remain higher than most other Western countries. Importantly, population coronary heart disease mortality is reduced more by a 1% relative reduction in cholesterol than by a 1% relative reduction in population mean blood pressure or smoking prevalence8,12,28–30 (appendix 2). The need for more effective dietary interventions is clear.
Key points
-
We examined the potential for cardiovascular risk factor reductions to reduce coronary deaths in Scotland and the UK by 2010.
-
Our cell based IMPACT CHD model combines information on patient numbers, treatment uptake and effectiveness, risk factor trends, and mortality benefits.
-
If major risk factors continued to reduce at current rates, 2169 fewer coronary deaths would be observed in Scotland in 2010.
-
Over 4000 deaths could be prevented if greater risk reductions, observed in other populations, were achieved for smoking, cholesterol, and blood pressure.
-
Extrapolation to the UK population suggests that UK coronary heart disease mortality could be almost halved.
As with all models, this analysis contains a number of limitations (see appendices 1 and 2). Firstly, it considers only mortality, and not years of life lost or morbidity. Our estimates of deaths prevented or postponed would translate into substantial numbers of life years gained.31 Secondly, the model is cell based and comparatively simple.7,8 The results should be replicated in a more complex simulation model, to explicitly consider lag times and interactions between various interventions.7,8,11,32 We considered only deaths from coronary heart disease, and it is possible that some increase in death rates from other “competing causes”33 may be observed. However, reductions in risk factors such as smoking would decrease deaths from other causes such as lung cancer.34
A number of further assumptions have been made. For example, whether mortality and risk factors will continue to decline at the same rate until 2010. It has also been assumed that the estimates obtained from Scotland can be extrapolated to the entire UK. Although socioeconomic factors may differ, this assumption seems justifiable as population distributions, life expectancy, and CHD risk factors are reasonably similar. Extensive sensitivity analyses were performed to consider higher or lower values for each regression coefficient.23,24 These influenced the number of deaths postponed or prevented, but did not change the relative contribution of each risk factor. International comparisons also suggest that much lower coronary death rates might well be achievable. Overall, the observed reduction between 1994 and 1998 has been slightly higher than expected from extrapolation. Our estimated reductions in 2010 may prove to be conservative. Furthermore, the recent National Service Framework for coronary heart disease treatment targets will probably also achieve substantial reductions.25,35
Existing UK government Saving Lives targets1 therefore seem achievable. However, continuation of the current trends cannot be assumed, given the “levelling off” in coronary heart disease mortality recently seen in the US.36 Britain lags behind many other countries and coronary heart disease will remain the biggest cause of death for the foreseeable future. Fresh initiatives to reduce major cardiovascular risk factors could produce further substantial reductions in mortality.28
Acknowledgments
We are extremely grateful to colleagues for constructive comments and further data including: Belgin Aslan, James Boyd, Vicky Grossmith, Barbara Hanratty, George Hart, Fiona Lampe, the Registrar General for Scotland, UK Data Archive.
REFERENCES
Supplementary materials
. Web-Only Appendices
Appendices 1 and 2 are provided here as a PDF (printer friendly file)
Appendix 1 Example of mortality fall due to reduction in smoking in men aged 45-54
Appendix 2 Methodological Issues: b coefficients and interactions between risk factors and treatmentsFiles in this Data Supplement:
Footnotes
-
Funding: JC and SC are both employed by the University of Liverpool, with funding from HEFCE.
-
Conflicts of interest: none.
Linked Articles
- In this issue