Article Text

Abstract
Objective: To investigate the association between previous abortion and low birth weight (LBW) and preterm birth (PB).
Method: The study examined live, singleton births using data from the United States Collaborative Perinatal Project. Logistic regression was used to control for obstetric and medical history, and lifestyle and demographic factors.
Result: Compared with women with no history of abortion, women who had one, two and three or more previous abortions were 2.8 (95% CI 2.48 to 3.07), 4.6 (95% CI 3.94 to 5.46) and 9.5 (95% CI 7.72 to 11.67) times more likely to have LBW, respectively. The risk for PB was also 1.7 (95% CI 1.52 to 1.83), 2.0 (95% CI 1.73 to 2.37) and 3.0 (95% CI 2.47 to 3.70) times higher for women with a history of one, two and three or more previous abortions, respectively.
Conclusion: Previous abortion is a significant risk factor for LBW and PB, and the risk increases with the increasing number of previous abortions. Practitioners should consider previous abortion as a risk factor for LBW and PB.
Statistics from Altmetric.com
Low birth weight (LBW) is one of the most important contributing factors to neonatal mortality and morbidity.1 LBW accounts for approximately two-thirds of all perinatal and infant deaths.2 LBW results from either a short period of gestation and/or a slow rate of intrauterine growth, and is generally defined as a birth weight less than 2500 g.1 When gestational age is less than 37 weeks, the birth is defined as preterm or premature. Approximately half of LBW infants are preterm; the other half being small for gestational age, generally defined as below the tenth percentile of weight-for-dates.2 A subset of small for gestational age infants who are LBW at term or 37 weeks of gestation are referred to as “term low birth weight” (TLBW).3
Histories of previous abortion, both miscarriage and induced abortion, have been associated with LBW and preterm birth (PB). In a review of risk factors for LBW, Kramer1 identified 37 and 41 studies of the association of miscarriage and induced abortion, respectively, with LBW. Much of this early literature, especially that concerning the risks associated with induced abortion, suffered from poor control for confounding factors and being unable to ascertain previous abortions and the techniques employed to induce the abortions.4 Furthermore, studies from the 1970s and early 1980s found previous abortions had no increased risk,5–8 increased risk,9 10 and decreased risk11 for LBW and/or PB. Studies published since the 1980s that used logistic regression analysis controlling for numerous potentially confounding factors also continued to show inconsistent findings. This study was designed to examine the relationship between previous abortions and TLBW and PB using data from the United States Collaborative Perinatal Project (CPP).
MATERIALS AND METHODS
Data collected by the National Institute of Neurological and Communicative Disorders and Stroke was used to conduct this study. The CPP was established in 1959 to examine the relationships between prenatal factors, labour, delivery and child development to seven years of age.12 From 1959 to 1966, medical and demographic history, birth outcomes and follow-up examinations were performed on a population of women giving birth in over 55 000 pregnancies at 12 medical centres in the United States. The full dataset of births consists of 59 391 mother–child paired records, of which 45 617 live, singleton births were selected for this analysis. The authors of this study could not get any documentation of approval from any ethics committee. Studies from these data are still being published in respectable journals.
For the purpose of this study, the outcome variable LBW was defined as birth weight less than 2500 g and TLBW was defined as infants with birth weight of less than 2500 g at 37 or more weeks of gestation. PB was defined as births at less than 37 weeks’ gestation. Previous abortion, the main independent variable, was often based entirely on maternal report and the data did not differentiate miscarriages and induced abortions. Further use of the term “abortion” in the results of this study includes both miscarriages and induced abortions.
Covariates examined included, race, age, parity, gravidity, prenatal visits, smoking, number of cigarettes smoked, and years smoked, weight (lbs), height (inches), body mass index (BMI), weight gain during pregnancy, IQ, socioeconomic index, occupation, alcohol dependence, illicit drug dependence, diabetes (yes/no), hypertension (yes/no), marital status, education, lowest haemoglobin, centre, infant gender, paternal race and education, infant birth weight and gestational age. Parity was categorised as zero, one to two, three to four and five or more pregnancies. For maternal occupation, the CPP grouped occupations according to “white collar”, “blue collar”, and “other”. The CPP identifications of “alcoholism” and “drug addiction” were renamed “alcohol dependence” and “drug dependence”, respectively, to reflect current terminology. For diabetes, the CPP coded mothers with diabetes before, during and after pregnancy. Mothers who had diabetes before and during pregnancy were coded as having diabetes. Hypertension occurring as a systolic blood pressure of greater than 160 mm Hg or a diastolic blood pressure greater than 110 mm Hg occurring between 24 weeks of gestation to labour was used as an approximation to preeclampsia, a variable the investigators did not identify in the data. Haemoglobin was provided by the CPP as gm/dl, and was recoded according to standard values for adult women.
Crude odds ratios along with 95% confidence intervals were calculated as the preliminary measures of association between previous abortion and TLBW and PB. Logistic regression modeling was used to estimate adjusted odds ratios and their 95% confidence intervals. Separate models were generated to include gravidity in place of parity and maternal IQ in place of maternal education (findings not included in the paper). The model with parity and maternal education was a better predictor and therefore the model with these variables was presented in this paper. Data on interpregnancy interval and previous stillbirths and PB were not available. Another set of logistic regression models was developed to estimate the strength of association between previous abortion and PB and TLBW as the outcome variable. The −2 log likelihood estimates were used to select the best predictor model.
RESULTS
Table 1 shows the general characteristics of the study population. The proportion of white and black women is equally distributed at 46%. The study population tended to be between the ages of 20 and 29 years, high school graduates, married, with one to two children, non-smokers, and reported having had no abortions. Approximately 11%, 14% and 6% had LBW, PB and TLBW, respectively.
The prevalence of LBW, TLBW and PB was highest among black women, younger and older age groups, less educated, and not married women (table 2). In addition, the prevalence of PB was highest for women with fewer than 10 and more than 20 prenatal visits. The prevalence of LBW, TLBW and PB increased with the increasing number of previous abortions.
The crude analysis demonstrated significant association between LBW, TLBW and PB and maternal race, age, education, marital status, parity, number of cigarettes smoked per day, BMI, weight gain during pregnancy, prenatal visits and infant gender (results not presented in table). When adjusted, all variables that showed significance in the crude analysis maintained their significance with the exception of maternal marital status, drug dependence and diabetes. Furthermore, parity lost its significance in the adjusted model for PB.
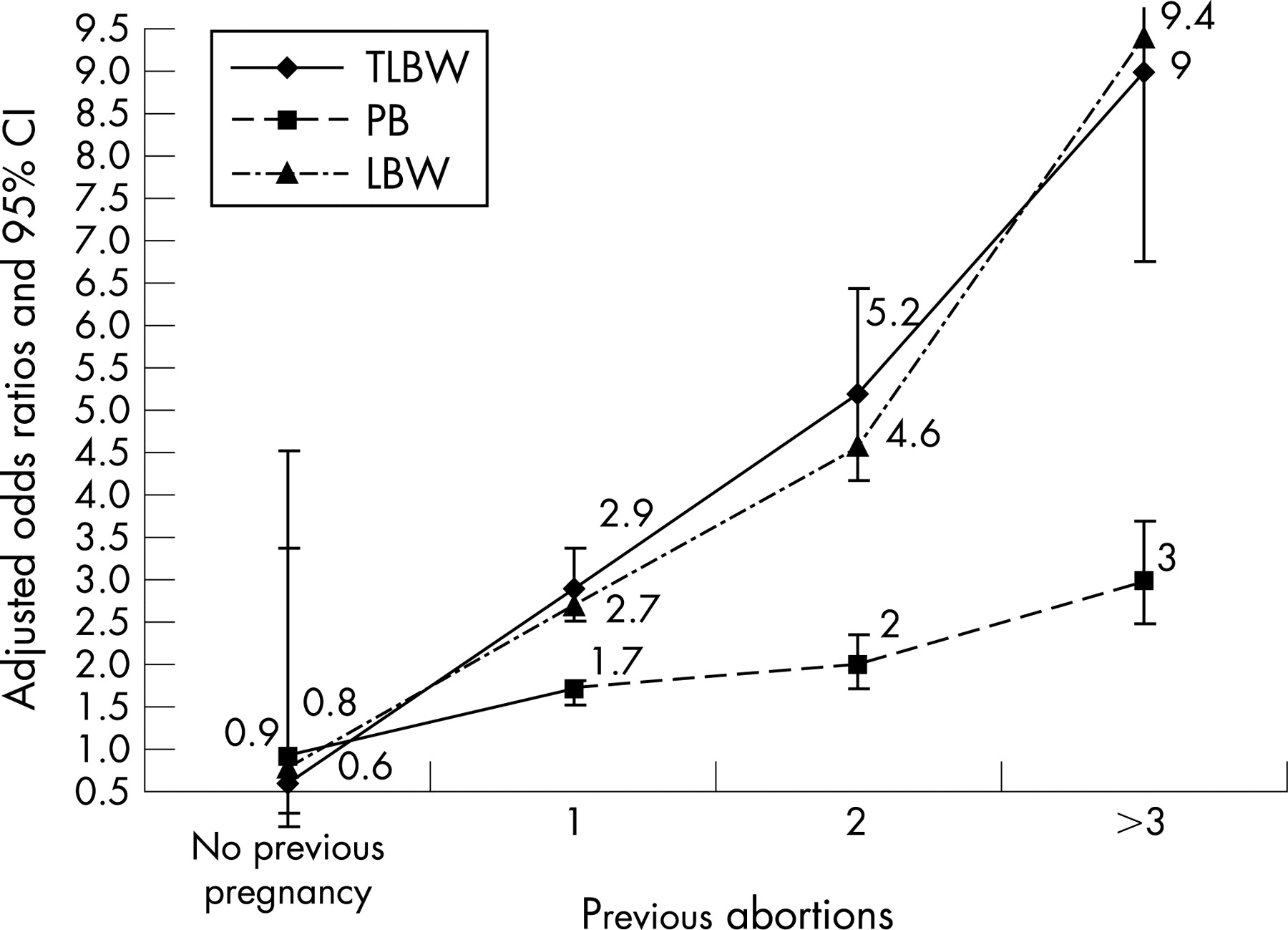
There was a strong statistical association between abortion and LBW, TLBW and PB after adjusting for race, age, maternal marital status and education, parity, smoking, alcohol and drug dependence, hypertension and diabetes during pregnancy, BMI, weight gain during pregnancy, number of prenatal visits, haemoglobin, infant gender and centre (table 3). Compared with women with no history of abortion, women who had had one, two and three or more previous abortions were 2.76 (95% CI 2.48 to 3.07), 4.64 (95% CI 3.94 to 5.46) and 9.49 (95% CI 7.72 to 11.67) times more likely to have LBW, respectively. Compared with women with no history of abortion, the risk of TLBW to women with one, two and three or more abortions was also nearly three, five and nine times higher, respectively (odds ratio (OR) 2.91, 95% CI 2.51 to 3.37; OR 5.10, 95% CI 4.10 to 6.34; and OR 9.07, 95% CI 6.84 to 12.02). When compared with women with no abortion, the risk of PB was 1.67 (95% CI 1.52 to 1.83), 2.03 (95% CI 1.73 to 2.37) and 3.03 (95% CI 2.47 to 3.70) times higher among women with one, two, and three or more abortions, respectively. As shown in fig 1, the risk of LBW, TLBW and PB increased with the increasing number of abortions, confirming a dose–response relationship.
{kind=link}
Compared with white women, black women were 1.74 (95% CI 1.50 to 2.03), 1.78 (95% CI 1.45 to 2.18) and 1.76 (95% CI 1.54 to 2.01) times more likely to have LBW, TLBW and PB, respectively (table 3). The risk of LBW, TLBW and PB increased with increasing age after the age of 30 years. Women with college education have the lowest risk. Inadequate prenatal visits (<10 visits) and number of visits more than 20 times during the pregnancy were significant risk factors for LBW, TLBW and PB. The risk of LBW and TLBW increased with increased smoking; however, the same trend was not observed for PB. Weight loss and lack of adequate weight gain are significant risk factors for LBW, TLBW and PB. Women with a BMI of less than 25.0 were at great risk of LBW, TLBW and PB.
DISCUSSION
This study identified previous abortion as a significant risk factor for LBW, TLBW and PB, and the risk increased with the increasing number of abortions. Only a few studies have tried to examine the association between TLBW and previous abortion. None of those studies found a statistically significant association after controlling for demographic and some obstetric factors.3 12 The only other study that found a modest association was a crude analysis conducted in Australia (OR 1.17, 95% CI 1.07 to 1.23).13 The reason for the inconsistent finding is not clear. In contrast, several studies found a strong association between miscarriages and induced abortions and PB12–18 and LBW.16 19 20 Table 4 shows a summary of the findings from selected studies that examined the association between abortion and LBW, TLBW and PB. The majority of those studies examining abortion and birth weight were conducted outside of the United States. The Boston study is the only study conducted within the United States, which showed no association between abortion and LBW. The study also showed no association between TLBW and abortion. A statistically significant association was, however, observed between abortion and PB, which is consistent with the finding in this study. Although the reason for the inconsistency between our findings and the study in Boston is unclear, other reviewers have also noted similar inconsistencies.21 Nevertheless, one should take into consideration the age of these data. The data for the current study were collected over 50 years ago, at which time the abortion laws, health and socioeconomic status of women were different from the current situation. If these variables were captured and controlled for in this analysis, the magnitude of the association between abortion and TLBW and PB could have been weaker as a result of the underreporting of abortions. Women in the late 1950s and early 1960s may not have reported previous abortions of any type, especially induced abortions that were illegal at the time, as openly as they might now report abortions. It is, however, essential to note in regard to the applicability of the study to modern women that many women in less developed countries live in a similar social context to the women of the United States 50 years ago.
Biological mechanisms that may be responsible for the association of previous abortions with TLBW appear to differ according to whether the previous abortions were miscarriages or induced abortions. For induced abortions, at least two major mechanisms have been identified: cervical insufficiency from dilatation and curettage and cervical and uterine adhesions as a result of post-abortion complications.22 In these instances, previous induced abortions would result in LBW through shortened gestation rather than through intrauterine growth retardation. Similar mechanisms may also underlie reported risks associated with other methods of induced abortion, such as vacuum aspirations or complications resulting from abortions, although the literature remains in conflict.5 19 22–24 Miscarriages, on the other hand, may not only cause cervical incompetence, but also may be associated with genetic, immunological, infectious or uterine abnormalities.25 These events could impact both gestational age and intrauterine growth. Unfortunately the CPP did not differentiate between previous miscarriages and induced abortions (whether therapeutically or illegally induced abortions) to clarify the causal mechanism.
The relative magnitudes of risk associated with the outcomes might offer clues as to the causal mechanism(s). Although this study showed that women with three or more abortions were three times more likely to have PB, the relative magnitude of having LBW or TLBW was nine times higher than those with no abortion. Had the study instead found higher risk associated with PB compared with LBW/TLBW, one might conclude that previous abortion caused cervical incompetence that resulted in PB and, to a lesser degree, LBW/TLBW. Because the reverse was found, PB resulting from cervical incompetence may not be the likely cause of this finding. Cervical incompetence might also be ruled out as the major determining factor for birth weight by the study’s finding that the adjusted odds ratios for LBW and TLBW did not differ greatly. A higher odds ratio for LBW than TLBW might be expected if cervical incompetence was the major limiting factor for birth weight. One must either consider the possibility that separate causative mechanisms influenced LBW and TLBW, respectively, or that causative mechanisms associated with intrauterine growth retardation such as uterine adhesions or infections influenced both outcomes.
What this paper adds
Studies published since the 1980s controlling for numerous potentially confounding factors continue to show inconsistent findings. Although few studies have shown significant association between abortion and LBW and PB, none of the studies utilised large population-based datasets. Unlike other studies, this study identified previous abortion as a significant risk factor for LBW, TLBW and PB, and the risk increased with the increasing number of abortions.
Policy implications
In conclusion, studies published since the 1980s controlling for numerous potentially confounding factors continue to show inconsistent findings. Unlike many smaller studies, but similar to a few studies comparable to or larger in size than the current study, this study identified previous abortion as a significant risk factor for LBW, TLBW and PB, and the risk increased with the increasing number of abortions. Women and healthcare professionals should be informed of this potential risk.
The current study found a higher risk of LBW, TLBW and PB than observed in most studies. One cross-sectional study, of smaller size than the current study, found not only a dose–response but a higher degree of risk from previous abortions for LBW than usually reported, especially in smaller studies. That study found a relative risk for four or more abortions (OR 4.16, 2.05 to 8.44)20 compared with the current study’s finding of an odds ratio of 9.49 (7.62 to 11.67). The reasons for the higher risks in the current study are not clear, but could be related to more than one issue. First, the current study could not differentiate between miscarriages and induced abortions. Second, this study did not control for urogenital infection histories and interpregnancy interval,16 which might have contributed to the higher risk observed in this study. Finally, a recent review of the literature also indicated an association between PB and induced abortions.21 The review cited two large Australian studies (n = 121 305 and n = 243 679, respectively), which found a large degree of risk from previous abortions for PB. The larger of the two studies found that women with four or more induced abortions had nine times the risk of extremely early PB than primigravidas.21
Another important finding in the current study was the lack of association between PB and smoking. This is particularly interesting because smoking demonstrated a strong association with LBW and TLBW. This finding indicates that smoking affects intrauterine growth but does not contribute to premature births. The literature on the impact of smoking on PB is inconsistent and needs further investigation.12 13 26–30
One of the major limitations of this study is its inability to differentiate induced abortions and miscarriages. As a result, comparing this study with other studies that differentiated miscarriages and induced abortions should be undertaken with caution. The authors have not found recent, controlled studies that examined the risks of TLBW from miscarriages and induced abortions combined. Some studies did examine the risks for LBW and PB, but the relative risks were not as high as those reported in the current study.14 15 31 Another limitation of this study is the age of the data, which may not reflect either the current causes of abortion, especially miscarriages or current estimates for abortion, PB, LBW or TLBW. Nevertheless, this study is the largest in the United States, and it provides the opportunity to examine and control for more confounding variables than most studies in the United States and elsewhere. Furthermore, findings from this study could be utilised by less developed countries where women face medical risks, including risks associated with illegal abortions, such as those of mid-20th century American women.
In conclusion, studies published since the 1980s controlling for numerous potentially confounding factors continue to show inconsistent findings. Unlike many smaller studies, but similar to a few studies comparable to or larger in size than the current study, this study identified previous abortion as a significant risk factor for LBW, TLBW and PB, and the risk increased with the increasing number of abortions. Women and healthcare professionals should be informed of this potential risk. Future research may wish to revisit the question of whether previous abortions can impact intrauterine fetal growth independent of prematurity. The controversy regarding the effect of previous abortion on TLBW appears suitable for future analysis using current data.
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- In this issue