Article Text

Abstract
Background A wide variety of pharmacological agents are used in the management of neuropsychiatric symptoms, which are common in Alzheimer's disease (AD), but results from randomised controlled trials (RCTs) on the efficacy and safety of these agents are conflicting.
Objectives To quantify the efficacy and safety of pharmacological treatment on neuropsychiatric symptoms in AD patients.
Methods Systematic review and meta-analysis of RCTs comparing pharmacological agents with placebo on Neuropsychiatric Inventory (NPI) and safety outcomes in AD patients with neuropsychiatric symptoms.
Results Cholinesterase inhibitors (ChEIs) and atypical antipsychotics improved NPI total scores (ChEIs: standardised mean difference (SMD) −0.12; 95% CI −0.23 to −0.02; atypical antipsychotics: SMD −0.21; 95% CI −0.29 to −0.12), but antidepressants (95% CI −0.35 to 0.37) and memantine (95% CI −0.27 to 0.03) did not. However, ChEIs and atypical antipsychotics increased risk of dropouts due to adverse events (ChEIs: risk ratio (RR) 1.64; 95% CI 1.12 to 2.42; atypical antipsychotics: RR 2.24; 95% CI 1.53 to 3.26) and on incidence of adverse events (ChEIs: RR 1.08; 95% CI 1.01 to 1.17; atypical antipsychotics: RR 1.17; 95% CI 1.05 to 1.31). For typical antipsychotics, no study was included.
Conclusions ChEIs and atypical antipsychotics could improve neuropsychiatric symptoms in AD patients, but with bad safety outcomes.
- Alzheimer's Disease
- Meta-Analysis
- Systematic Reviews
- Neuropsychiatry
Statistics from Altmetric.com
Introduction
The global prevalence of dementia is as high as 24 million and has been predicted to quadruple by the year 2050. Alzheimer's disease (AD) is the most common form of dementia, accounting for an estimated 60%–80% of cases. In the USA alone, AD causes an estimated healthcare costs of $172 billion per year.1 It has been suggested that neuropsychiatric symptoms rather than cognitive dysfunction or functional impairment imposed the greatest burden on family caregivers, and predicted the caregivers’ decisions to institutionalise patients with dementia. Therefore, interventions aimed at improving neuropsychiatric symptoms could have a tremendous impact on patients, caregivers and society. There are multiple classes of pharmacological agents in use for neuropsychiatric symptoms, including, but not limited to, cholinesterase inhibitors (ChEIs), antipsychotics, antidepressants, mood stabilisers and N-methyl-D-aspartate–receptor modulators. Some clinical trials and meta-analyses2–7 have evaluated the efficacy and safety of these drugs on neuropsychiatric symptoms, but have had conflicting findings. Thus, we performed a systematic review and meta-analysis to quantify the efficacy and safety of pharmacological interventions for neuropsychiatric symptoms in AD patients.
Methods
Identification of trials
We systematically searched PubMed, EMBASE, the Cochrane Controlled Trials Register and the Cochrane Database of Systematic Reviews for reports published before December 2013. The search criteria combined three separate domains: condition (Alzheimer's disease or AD), intervention (cholinesterase inhibitors; donepezil; galantamine; rivastigmine; metrifonate; tacrine; antipsychotics; haloperidol; thioridazine; thiothixene; chlorpromazine; acetophenazine; clozapine; olanzapine; risperidone; quetiapine; aripiprazole; antidepressants; setraline; fluoxetine; citalopram; trazodone; mood stabilizers; valproate; carbamazepine; lithium; anticonvulsants; benzodiazepines; memantine; or psychotropic drugs) and symptoms (behavioral and psychological symptoms of dementia, BPSD, neuropsychiatric symptoms, behavior). Terms were searched in titles and abstracts. We retrieved English-language articles for review, and also collected additional references from bibliographies of reviews, original research articles and other articles of interest.
Study selection and data extraction
Two investigators independently reviewed all pertinent articles using predetermined inclusion criteria. Trials were selected for inclusion if they met all of the following criteria: (1) double-blind, placebo-controlled, randomised controlled trials (RCTs); (2) the design of the trial was either parallel or crossover; for a crossover trial, it had a washout period greater than 1 week; (3) patients enrolled were diagnosed as probable or possible AD according to the Diagnostic and Statistical Manual of Mental Disorders—Fourth Edition or the criteria of the National Institute of Neurological and Communicative Disorders and Stroke/Alzheimer's Disease and Related Disorders Association; (4) studies compared any medicine at any dose with placebo, with any treatment durations; and (5) neuropsychiatric outcomes were measured with the most common neuropsychiatric scales—Neuropsychiatric Inventory (NPI) (NPI-10 or NPI-12) or Neuropsychiatric Inventory-Nursing Home version (NPI-NH).
For each trial, two reviewers were blinded to the authors and journal, and independently abstracted data. The mean change of NPI total scores and SDs for the mean change were extracted. For SDs that were not reported directly, we sought them from the authors or calculated them from SEs, CIs or p values that relate to the difference between means in two groups according to the Cochrane Handbook for Systematic Reviews of Interventions. Studies were excluded if the mean change of NPI total scores were not available. Moreover, if there were duplicate publications from the same population, only one of the trials that reported the mean change of NPI total score and SD was included, others were excluded. Besides the sample size, mean age, sex, race, treatment regimen, discontinuations and adverse events were also collected. Wherever possible, outcomes from the intention-to-treat (ITT) population were used and, if not possible, observed case or per protocol outcomes were extracted. Discrepancies in the collected data were discussed and if consensus was not reached, a third reviewer was the final arbitrator.
Statistical analysis
Meta-analyses were performed using Review Manager V.5.2 software. Combining the NPI-10, NPI-12 and NPI-NH scales in an overall summary estimate, we calculated standardised mean differences (SMDs) and 95% CIs for changes from baseline for continuous data. For dichotomous dropouts and adverse events, we conducted an analysis of the risk ratio (RR), absolute risk differences with 95% CI and p values to assess the safety of the study drug. A random effect model was applied to assess the effect sizes for each treatment–placebo comparison in our study. In dose-ranging trials with multiple treatment groups, we combined treatment groups by weighting the effects for each subgroup by its sample size according to the Cochrane Handbook for Systematic Reviews of Interventions.
The degree of heterogeneity was assessed by visual inspection, and by a χ² test combined with the I² method. An α error p<0.20 and an I2>50% were regarded as indicators of heterogeneity of outcomes. To establish the robustness of the outcome, we excluded studies in which the SDs were absent or estimated, or ITT analysis was not used, to conduct sensitivity analyses. Subgroup analyses were performed based on different medicines if there were more than three trials for same one. We also assessed the risk of bias according to Cochrane criteria. Publication bias was evaluated using STATA12.0 software with Begg's test method and funnel plots were presented. In addition, we applied GRADE Profiler 3.6 to assess quality of the included trials according to the GRADE criteria. All analyses were two-tailed, with 5% risk of a type I error (α of 0.05).
Results
Literature search findings and characteristics of included trials
The results of the search process are depicted in the flow chart (figure 1). Of 2035 articles identified, 32 met all review criteria, including 15 ChEIs trials,8–22 six atypical antipsychotic trials,23–28 two antidepressant trials,29 ,30 one mood stabiliser trial31 and eight memantine trials.32–39 All studies were randomised, double-blind, placebo-controlled trials and were performed mainly in North American and European countries. Baseline characteristics were similar between intervention and placebo groups in all the trials. Among the 32 included studies, three was randomised crossover design trials, and the others were randomised parallel trials. In all, 16 trials compared with one fixed-dose of medicine and placebo, and 16 were dose ranging. Among these dose-ranging studies, five used more than one dose compared with a single placebo group.

Flowchart of randomised controlled trials (RCTs) included and excluded in the meta-analysis. NPI, Neuropsychiatric Inventory; VD, vascular dementia.
The 32 trials included 6812 patients in medicine treatment group and 4844 participants in placebo treatment group. The mean ages of patients in medicine treatment groups ranged from 73.3 to 85.6 years. The mean baseline MMSE scores ranged from 4.5 to 21.2. The detail characteristics of these studies and populations were listed in online supplementary table S1.
Bias risk assessment
Although all included trials were randomised, double-blinded and placebo-controlled, specification of randomisation and allocation concealment methods were different from each other. The randomisation was conducted according to a computerised randomisation schedule among nine trials, 11 reports specified the varied methods of randomisation and the other 12 reports did not give detail information, although they were noted randomisation. Twenty-one studies explicitly mentioned use of placebo and drug tablets or capsules that were visually identical for allocation concealment; no adequate details were provided in the others. Moreover, in most (28) trials, efficacy outcomes were analysed by ITT data with the last observation carried forward methods for minimising effects of attrition bias. Finally, small sample size, crossover and multi-arm studies may produce other bias. Begg's test indicated that there was no significant publication bias, and funnel plots were presented in online supplementary figure S1. The quality of reports of all included studies was appraised with GRADE, and the outcome was listed in online supplementary table S2.
Efficacy
Cholinesterase inhibitors
Fifteen RCTs of various ChEIs (eight for donepezil, four for galantamine and three for metrifonate) with neuropsychiatric symptom outcomes have been selected, with seven of the 15 studies reporting statistically significant benefit. Twelve trials reported data from the ITT analysis, with three trials reporting data only from the completed subjects analysis. For two trials,17 ,22 the SDs for the mean change of NPI total scores were not available, but the results still suggested that ChEIs significantly benefited behavioural disturbances of AD patients compared with placebo (p<0.05). We conducted meta-analyses with the other 13 trials. The summary meta-analysis also indicated that ChEIs improved neuropsychiatric symptoms on NPI scale compared with placebo (SMD −0.12; 95% CI −0.23 to −0.02) (figure 2). Here, we detected a substantial heterogeneity (I2=67%), which may be explained by the different subtype of medicine, characteristics of populations, such as the mean age, race, baseline MMSE, and so on, and the treatment duration. In sensitivity analyses excluding studies that did not use ITT analysis method (SMD −0.14; 95% CI −0.25 to −0.03) or the only one long-term trial (SMD −0.15; 95% CI −0.24 to −0.06), we could still observe the improvement effect. However, when excluding studies that used estimated SDs, the significant benefit disappeared (95% CI −0.23 to 0.02). No significant publication bias was detected (continuity corrected z=0.62, Pr>|z|=0.537) (see online supplementary figure S1A).

Forest plot of efficacy of various drugs on the Neuropsychiatric Inventory scale in Alzheimer's disease patients. Data type: continuous; effect measure: standardised mean difference; analysis model: random effects; statistical method: inverse variance.
In donepezil subgroup, we did not detected significant effects on neuropsychiatric symptoms (95% CI −0.27 to 0.08) (heterogeneity: I2=76%). While in galantamine subgroup, our meta-analysis result indicated that galantamine could significantly improve behavioural disturbances of AD patients (SMD −0.13; 95% CI −0.22 to −0.03) (heterogeneity: I2=0%) (figure 3).

Forest plot of efficacy of donepezil and galantamine on the Neuropsychiatric Inventory scale in Alzheimer's disease patients in subgroup analyses. Data type: continuous; effect measure: standardised mean difference; analysis model: random effects; statistical method: inverse variance.
Atypical antipsychotics
Atypical antipsychotics, also known as second-generation antipsychotics, include clozapine, olanzapine, risperidone, quetiapine, ziprasidone and aripiprazole. Six RCTs completely met our inclusion criteria and were selected in our meta-analysis. Of these, one study23 used three different drugs and compared them with placebo respectively. Thus, we extracted data from it three times, forming eight comparisons. Five comparisons reported positive results. With these trials, our summary meta-analysis showed significant improvement on NPI total score in patients treated with atypical antipsychotics compared with placebo (SMD −0.21; 95% CI −0.29 to −0.12). The heterogeneity among the pooled study was mild (I2=0%). The improvement on NPI scale was also significant in sensitivity analysis excluding studies that used estimated SDs (SMD −0.26; 95% CI −0.39 to −0.13). Begg's test did not detect significant publication bias (continuity corrected z=0.62, Pr>|z|=0.536) (see online supplementary figure S1B).
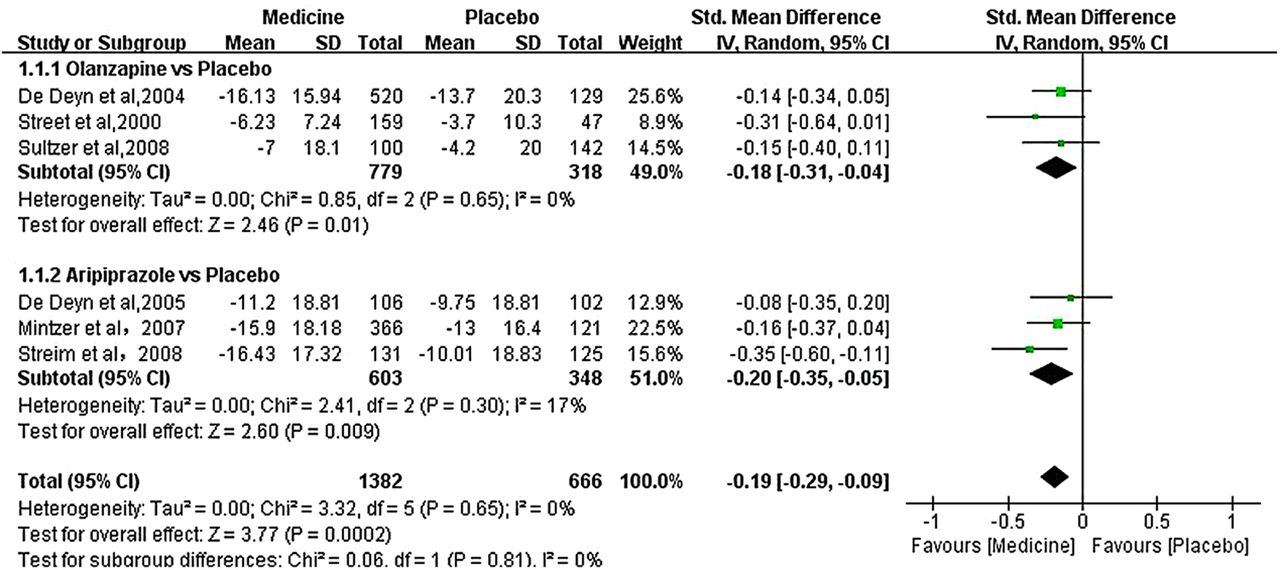
In subgroup analyses, the results suggested that olanzapine significantly benefited on behaviour symptoms of AD patients (SMD −0.18; 95% CI −0.31 to −0.04) (heterogeneity: I2=0%). In aripiprazole subgroup, we also detected significant improvement on NPI scale (SMD −0.20; 95% CI −0.35 to −0.05) (heterogeneity: I2=17%) (figure 4).

Forest plot of efficacy of olanzapine and aripiprazole on the Neuropsychiatric Inventory scale in Alzheimer's disease patients in subgroup analyses. Data type: continuous; effect measure: standardised mean difference; analysis model: random effects; statistical method: inverse variance.
Antidepressants
Antidepressants include, but not limited to, sertraline, fluoxetine, citalopram and trazodone. Only two RCTs on sertraline were selected in our study. Both of them were randomised, placebo-controlled, parallel, 12-week, flexible-dose clinical trials. One study included 24 AD patients in sertraline group and 20 AD patients in placebo group. The other study enrolled 124 patients and 120 patients in drug and placebo groups, respectively. Neither of the two trials found significant differences in NPI total scores between sertraline and placebo groups over time. In consistent, the result of our meta-analysis did not detect significant differences on changes of NPI scales between the two groups (95% CI −0.35 to 0.37) (heterogeneity: I2=35%).
Mood stabilisers
Only one eligible RCT was included in our study. It was a randomised, double-blind, placebo-controlled, crossover trial of valproate in institutionalised AD patients. The trial only included 14 patients in valproate group and 13 patients in placebo group. Treatment duration lasted 6 weeks, with a 2-week washout period. The result did not find significant differences on the changes of NPI total scores between valproate and placebo groups (p=0.075), but it suggested a trend that valproate treatment might worsen the NPI total score compared with placebo. The small sample size limited the credibility of the result.
Other drugs
Memantine, an N-methyl-D-aspartate receptor antagonist, has been approved in the USA for the treatment of moderate to severe AD. Eight RCTs including 1496 patients in memantine group and 1333 patients in placebo group reported NPI measures. No significant behavioural benefit was observed on NPI total score in our meta-analysis (95% CI −0.27 to 0.03). There was large heterogeneity among pooled memantine studies (I2=75%). Although all trials were RCTs and treated patients with memantine 20 mg daily, the characteristics of populations differed from each other, such as the mean age, race, baseline MMSE and so on. Besides, the treatment duration ranged from 12 to 28 weeks. These discrepancies may explain the large heterogeneity. No significant publication bias was observed in Begg's test (continuity corrected z=1.36, Pr>|z|=0.174) (see online supplementary figure S1C). In sensitivity analyses, we still did not find significant benefit of memantine on neuropsychiatric symptoms after excluding studies that used estimated SDs (95% CI −0.27 to 0.01) or did not use ITT analysis method (95% CI −0.31 to 0.00).
For typical antipsychotics, benzodiazepines and other drugs, we did not search any study that met our inclusion criteria completely.
In addition, we conducted a meta-analysis to assess the efficacy of pharmacological treatment on neuropsychiatric symptoms in patients with any diagnosis of dementia. We also broadened the neuropsychiatric outcomes to include either NPI or the Behavioural Pathology in Alzheimer's Disease (BEHAVE-AD) rating scale. The characteristics of additional studies in this part of meta-analysis were listed in online supplementary table S3. Our results showed that ChEIs and atypical antipsychotics significantly improved neuropsychiatric symptoms compared with placebo (ChEIs, SMD −0.11; 95% CI −0.20 to −0.01; atypical antipsychotics, SMD -0.18; 95% CI −0.27 to −0.09), while antidepressants and memantine did not (antidepressants, 95% CI −0.35 to 0.37; memantine, 95% CI −0.27 to 0.01) (see online supplementary figure S2). More detailed information is available in online supplementary appendix 1.
Safety
All-cause dropouts
In overall meta-analyses on safety, there were no significant differences in the number of dropouts caused by any reason between any medicine treatment group and placebo treatment group (ChEIs: 95% CI 0.98 to 1.55; atypical antipsychotics: 95% CI 0.89 to 1.00; antidepressants: 95% CI 0.52 to 1.38; memantine: 95% CI 0.73 to 1.08) (figure 5). In donepezil and metrifonate subgroups, we observed similar results (donepeil: 95% CI 0.74 to 1.32; metrifonate: 95% CI 0.87 to 2.32). However, in the galantamine subgroup, the number of all-caused dropouts was significantly higher in galantamine treated group than in placebo treated group (RR 1.75; 95% CI 1.10 to 2.76) (figure 6).

Forest plot of safety of various drugs on all-caused dropouts in Alzheimer's disease patients. Data type: dichotomous; effect measure: risk ratio; analysis model: random effects; statistical method: Mantel–Haenszel.

Forest plot of safety of donepezil, galantamine and metrifonate on all-caused dropouts in Alzheimer's disease patients in subgroup analyses. Data type: dichotomous; effect measure: risk ratio; analysis model: random effects; statistical method: Mantel–Haenszel.
Adverse events-caused dropouts
In ChEIs treated group, the number of withdrawals due to adverse events was significantly higher than in placebo treated group (RR 1.64; 95% CI 1.12 to 2.42) (figure 7). In atypical antipsychotics group, the number of adverse events caused dropouts was also higher (RR 2.24; 95% CI 1.53 to 3.26). But for antidepressants and memantine, we did not observe significant differences in the number of dropouts due to adverse events (antidepressants: 95% CI 0.52 to 1.94; memantine: 95% CI 0.71 to 1.38).

Forest plot of safety of various drugs on adverse events-caused dropouts in Alzheimer's disease patients. Data type: dichotomous; effect measure: risk ratio; analysis model: random effects; statistical method: Mantel–Haenszel.
Adverse events
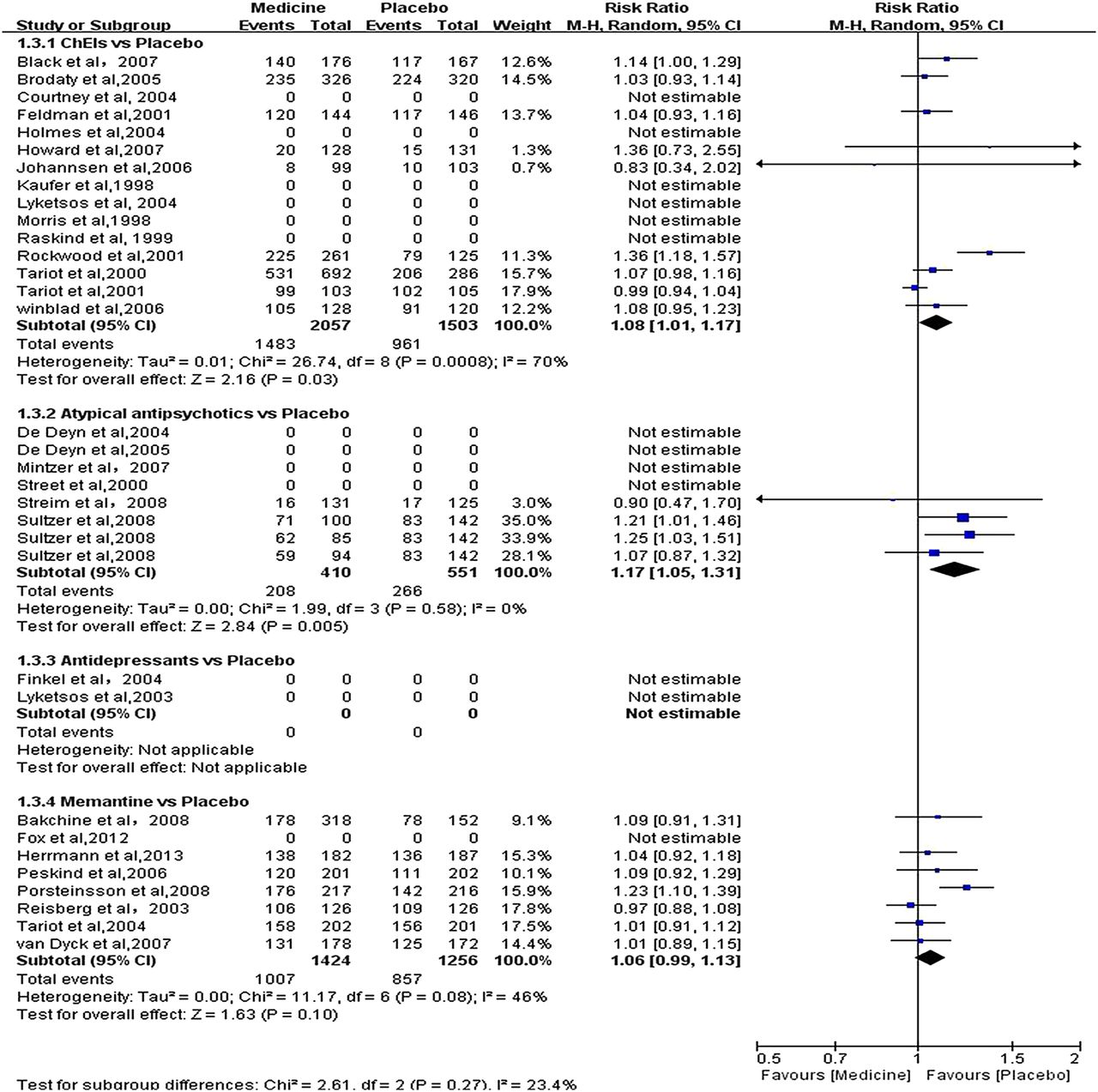
Adverse events were inconsistently mentioned in all trials. The common adverse events included but not limited to gastrointestinal symptoms (nausea, vomiting, diarrhoea, anorexia, etc), dizziness, headache, agitation, respiratory tract infection, asthenia, urinary tract infection and so on.
Patients in ChEIs and atypical antipsychotics groups experienced more adverse events than in placebo group (ChEIs: RR 1.08; 95% CI 1.01 to 1.17; atypical antipsychotics: RR 1.17; 95% CI 1.05 to 1.31) (figure 8). For memantine, no significant difference was detected in adverse events between memantine and placebo groups (95% CI 0.99 to 1.13).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of safety of various drugs on adverse events in Alzheimer's disease patients. Data type: dichotomous; effect measure: risk ratio; analysis model: random effects; statistical method: Mantel–Haenszel.
In the additional meta-analysis of safety of pharmacological treatment in patients with any type of dementia, ChEIs increased the risk of all-caused dropouts (RR 1.34; 95% CI 1.14 to 1.58) (see online supplementary figure S3) and adverse events (RR 1.10; 95% CI 1.04 to 1.18) (see online supplementary figure S4); both ChEIs (RR 1.74; 95% CI 1.33 to 2.27) and atypical antipsychotics (RR 1.99; 95% CI 1.50 to 2.63) increased risk of dropouts due to adverse events (see online supplementary figure S5). For memantine, we did not detect any significant bad safety outcomes.
Discussion
Among the various drugs in use for the treatment of neuropsychiatric symptoms, we found that ChEIs and atypical antipsychotics have convincing evidence of benefit for neuropsychiatric symptoms, but with certain adverse effects. For antidepressants and memantine, we did not observe significant benefit for neuropsychiatric symptoms, even though without significant adverse effects.
So far, two meta-analyses2 ,3 have demonstrated that ChEIs show benefit for neuropsychiatric symptoms, which is consistent with the results of our study. For memantine, one meta-analysis4 found that it improved behaviour symptoms while two4 ,6 did not demonstrate that. In addition, donepezil,4 galantamine5 and metrifonate7 were all proved to have significant effect on neuropsychiatric symptoms in early studies. However, in current meta-analysis, only galantamine was verified beneficial for neuropsychiatric symptoms. For atypical antipsychotics and antidepressants, no other meta-analyses have been published. The inclusion criteria for different studies are not completely identical; therefore, the results are different. For example, in study of Gauthier et al,6 they enrolled patients with moderate to severe AD, while in our study, we enrolled patients with any severity of AD. Moreover, our meta-analysis excluded trials in which data of the mean change of NPI scores from baseline in drug and placebo groups were not available, and included studies published in recent years. All these may impact the results of the study.
The strengths of this study include the inclusion of the lately published trials, which were not (or not entirely) included in previous reviews. Moreover, we applied widely used meta-analytic techniques to calculate the non-reported data such as SDs, thus, minimising missing data. Furthermore, we assessed the quality of the included trials, and presented a summary table of the outcomes. Finally, we analysed the effect and safety of almost all common drugs that were clinically used to treat neuropsychiatric symptoms. Our findings of the significant improvement in neuropsychiatric scales in AD patients treated with ChEIs, atypical antipsychotics are important, because neuropsychiatric problems are common in AD, and are major contributors to loss of autonomy, morbidity and need for nursing home placement.
Several limitations to our meta-analysis restrict the interpretation of our results. First, the NPI seems to be the most comprehensive scale and is thought to be more sensitive to change than some other scales; therefore, it has been widely used to appraise the neuropsychiatric symptoms. However, there are still some studies that did not apply it, especially studies performed before the generation of the NPI scale. This causes some trials to be excluded from our study. Second, some of our included trials excluded participants receiving psychotropic medicines, while some trials allowed, and even demanded, the use of medicines such as ChEIs and other drugs in their study. The use of such medicines may have an impact on our results. In addition, as mentioned above, AD is progressive, and patients declined at progressive different stages of severity, which may also influence our results when pooling data. Finally, very few trials were included for typical antipsychotics, antidepressants and mood stabilisers. Therefore, no convincing conclusions can be drawn regarding the efficacy of these drugs for neuropsychiatric symptoms.
Despite some limitations, we believe that our results are the first attempt to quantitatively synthesise the efficacy and safety of various of medicines for neuropsychiatric symptoms of AD patients, suggesting a mild to moderate benefit in neuropsychiatric outcomes from ChEIs and antipsychotics. Our meta-analysis results indicate that for AD patients who have neuropsychiatric disturbances, ChEIs and atypical antipsychotics may be considered as a therapeutic option. However, it is notable that the decision to use these medicines needs to be considered in light of the adverse effects, cost and feasibility. As recommended,40 for AD patients with neuropsychiatric symptoms, excluding the medical and environmental factors, non-pharmacological interventions should be attempted before moving to drug therapy. If non-pharmacological interventions do not work, drug therapy should be used to manage neuropsychiatric symptoms. For patients with symptoms of depression or anxiety, selective serotonin reuptake inhibitors, such as antidepressants, are advised for treating the symptoms patients exhibit. For patients without symptoms of depression or anxiety, combining with the goal of minimising adverse effects, ChEIs are first recommended for well tolerated, and then atypical antipsychotics. Typical antipsychotics are not recommended because there is less evidence of benefit and more adverse effects compared with atypical antipsychotics.
Overall, our meta-analysis results indicate a benefit in neuropsychiatric symptoms for AD patients from ChEIs and atypical antipsychotics. Future researches should focus more on neuropsychiatric outcomes. It is important to continue efforts to perform high-quality trials of non-pharmacological treatments in combination with drug therapy, and the safety evaluation of the drugs cannot be ignored.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors JTY and LT designed the analysis. JW, HFW, XFM, CW and CCT collected and abstracted the data. JW and HFW carried out the statistical analysis. JW and JTY drafted the manuscript. All authors analysed and interpreted the data and critically revised the manuscript for important intellectual content. The contents of this study are solely the responsibility of the authors and do not necessarily represent the official view of their institutions or any other party. JTY and LT have full access to all of the data and take full responsibility for the data, analyses and interpretation. All authors reviewed and approved the final report.
-
Competing interests None.
-
Ethics approval In accordance with NRES and MRC guidance, this study does not require ethics approval as it does not directly involve human participants. The data used in the systematic review and meta-analysis have come from studies which have previously satisfied regulatory requirements and been peer reviewed.
-
Provenance and peer review Not commissioned; externally peer reviewed.