Article Text

Abstract
OBJECTIVES Cognitive impairment is known to occur in schizophrenia, and may be marked in institutionalised patients. The aim of this study was to determine whether it ever warrants an additional diagnosis of dementia.
METHODS A population of chronic schizophrenic patients who were aged 65 or younger and showed no organic risk factors for dementia were screened for presence of disorientation. Any showing this underwent neuropsychological testing, physical investigations, and structural and functional neuroimaging. Information about day to day cognitive function was also obtained from carers.
RESULTS Eight patients aged 28 to 64 were identified who showed disorientation; in all cases this was accompanied by general intellectual impairment and objective evidence of a dementia syndrome. The patients' schizophrenic symptoms were unexceptional and did not seem sufficient to account for their cognitive impairment. Neuropsychological testing disclosed relative sparing of visual and visuospatial function and language syntax, but pervasive deficits in memory and executive function. Brain CT demonstrated only minor abnormalities but most of the patients showed frontal or temporal hypoperfusion on SPECT.
CONCLUSIONS Dementia in schizophrenia seems to be a real entity with a neuropsychological signature similar to that of frontotemporal dementia. Functional but not structural imaging abnormalities may also be characteristic.
- schizophrenia
- dementia
- cognition
Statistics from Altmetric.com
As a “functional” psychosis, schizophrenia has, from the beginning of the century, been distinguished from the “organic” psychoses of dementia and delirium by the absence of any compromise of intellectual function.1 2 For example, in one of the original descriptions of the disorder, Kraepelin3 stated that patients “remain surprisingly clear despite the most violent excitement” and “often know accurately to a day how how long they have been in the institution”. This distinction has stood the test of time to the extent that acutely psychotic schizophrenic patients do not typically show disorientation, memory impairment, or other evidence of cognitive failure, and were they to do so investigations would normally be undertaken to exclude underlying neurological disease. Nevertheless, over the past 20 years it has become clear that it is an oversimplification. Thus schizophrenic patients have been found to have a lower average IQ than the normal population,4 and to show wide ranging neuropsychological test impairments, prominent among which are deficits in memory and executive function.5 6These deficits have been found in drug free7 8 and never treated patients,9 and they are not easily attributable to poor motivation, attention, and cooperation.10-13
It is also well established that institutionalised schizophrenic patients, who have the most severe and chronic forms of illness, sometimes show more marked cognitive deficits which can be detected on the simple “bedside” tests of general knowledge, recall, copying, etc used to screen elderly patients for dementia.14-16 Up to 25% of such patients also show age disorientation, typically underestimating their age by a margin of 5 years or more.17 This phenomenon has been shown not to be a function of pre-existing learning disability, prior physical treatments, or institutionalisation, and it forms part of a wider pattern of cognitive impairment.18 19 Both global intellectual impairment and age disorientation increase in prevalence with advancing age in the population chronically in hospital and become commonplace over the age of 65.16 20
In 1976 Marsden21 argued for the logical extension of these findings, writing: “I have encountered a number of chronic schizophrenic patients in whom full investigation has revealed evidence of cognitive impairment and cerebral atrophy on air encephalography, whereas all other investigations for known causes of dementia have been negative.” Nevertheless, despite this and occasional similar statements,22 23 dementia is not normally considered to supervene in schizophrenia and is not clearly recognised as a complication of the disorder. Such a view also runs counter to the prevailing beliefs that schizophrenic cognitive impairment is present premorbidly,24 25 is neurodevelopmental in origin,26 and represents a “static encephalopathy”.27 Finally, little is known about the pattern of neuropsychological impairment in severely cognitively impaired schizophrenic patients and its correlates, if any, in structural and functional imaging.
Methods
Patients with a clinical diagnosis of schizophrenia in a large rehabilitation service catering mainly for chronic psychotic illness were informally questioned about orientation in time, place, or person. Any showing evidence of disorientation were administered a more detailed orientation questionnaire previously used in a study of institutionalised schizophrenic patients.18 This covers general orientation, age orientation, elementary general knowledge, and knowledge about daily (for example, ward) routine. Only patients up to the age of 65 were included, to avoid the prevalence of dementia due to organic disease above this age. Patients were excluded if they had a history of head injury, neurological disease, or any disease known to affect brain function, drug or alcohol misuse, or learning disability. History of known ischaemic heart disease, peripheral vascular disease, or hypertension were further exclusion criteria. Finally, any patients who gave absurd or delusional responses—for example, stating their age to be 200—were excluded from consideration.
Patients who made five or more errors on the orientation questionnaire were studied further to establish whether they met diagnostic criteria for dementia. According to ICD 10 and DSM-IV, this requires evidence of memory impairment as well as multiple additional cognitive impairments (for example, aphasia, apraxia, agnosia, poor executive function) which impair social or occupational functioning. There must also be evidence for a decline in cognition. Other CNS conditions have to be excluded.
Current intellectual level was assessed using the Wechsler adult intelligence scale (WAIS) to measure IQ, plus the mini mental state examination (MMSE),28 a clinically oriented cognitive screening test where a score of 23/24 out of 30 has become widely used as a cut off for dementia.29 To assess premorbid IQ, educational achievement was determined, and the national adult reading test (NART)30 was administered. This gives an estimate of best level of IQ functioning based on ability to pronounce irregular English words, and is relatively resistant to the effects of adult onset dementing illness. A difference in WAIS IQ compared with NART estimated IQ of more than 15 points is widely used as a cut off for significant IQ decline.31 Specific neuropsychological tests covered standard areas of visual perception (subtests of the visual object and space perception battery (VOSP)32 and Rey figure copying33), language (the graded naming test34 35 and the modified token test36), memory (the doors and people test37), and executive function (the modified Wisconsin card sorting test (WCST38), verbal fluency (number of animals generated over 1 minute) and the cognitive estimates test39). Carers of the patients were interviewed and completed a questionnaire covering objective signs of dementia.40 Neuropsychological testing was carried out with ethics committee permission, and patients (and where possible their relatives) gave consent for this and further investigations.
To exclude other CNS conditions, patients underwent physical and neurological examination. Routine haematology and biochemistry and chest radiography were performed, plus standard screening investigations for dementia, including thyroid function tests, red cell and serum B12 and folate, and syphilis serology. Patients over 40 also had ECG. Further investigations included autoimmune screen and white cell enzyme assay for metachromatic leukodystrophy. Brain imaging included CT in all cases, and MRI where indicated on the basis of questionable CT findings. Tc 99m HMPAO single photon emission computed tomography (SPECT) was carried out on seven patients (one patient refused consent for this procedure).
DSM-IV criteria for dementia additionally require that the disturbance in cognitive function cannot be better accounted for by another disorder such as schizophrenia. This requirement may partly be in recognition of the fact that cognitive impairment is now accepted in schizophrenia, but it also reflects a longstanding belief that such impairment may sometimes be more apparent than real because of the distracting effects of symptoms, poor cooperation, or lack of motivation on performance. To examine this issue, the patients' symptoms were rated using the positive and negative syndrome scale (PANSS),41 a 30 item rating scale designed to assess the full range of psychopathology in schizophrenia; the scale also contains an item rating disorientation.
Results
Eleven patients were identified who failed five or more items on the orientation questionnaire but of these, only eight were cooperative enough to permit further investigation. Ages ranged from 27 to 64. All patients met DSM-IV criteria for schizophrenia, based on detailed clinical assessment and review of case notes. All but one patient (see below) had unexceptional presentations of severe, chronic illness. The duration of illness was generally long, ranging from 9 to 30 years. Four of the patients were chronically in hospital, with the remainder being cared for at home by relatives (one), living in sheltered accommodation (two), or being treated on an acute psychiatric ward having lived at home before admission (one). All patients were taking neuroleptic medication, but only one (patient 5) was taking anticholinergic medication at the time of testing. One (patient 8) had had electroconvulsive therapy, but not in the preceding 12 months. None of the patients had been treated in the past with insulin coma therapy.
Figure 1 shows the eight patients' orientation scores in comparison with a sample of 120 other rehabilitation patients with a clinical diagnosis of schizophrenia who met the same inclusion and exclusion criteria. This sample was a subset of the patients in the service and was designed to encompass the range of severity encountered in chronic schizophrenia. It was made up of all those who were chronically in hospital or living in 24 hour staffed hostel accommodation (n=63), plus a similar number of patients who were able to live partially or fully independently (n=57). The vast majority of patients made at most two errors, and the eight disoriented patients were at the tail of a distribution that was markedly skewed to the left (the three further patients with orientation scores of 15 or less were those mentioned above who were not compliant enough to be tested). There were significantly more women in the disoriented patients than the comparison sample (men:women 3:5 v 60:30; p=0.035), but the two groups did not differ significantly in age (mean 46.6 v 43.5; NS) or years of education (mean 11.6 v 11.8; NS).

Orientation scores for a sample of 128 chronic schizophrenic patients.
The eight patients' educational backgrounds and cognitive status findings are summarised in table 1. All had received primary and secondary education at normal schools; two had O levels and one had a university degree plus a PhD. Two of the patients had become ill before leaving school; the rest had worked in normal adult occupations. All patients showed multiple orientation failures coupled with evidence of global intellectual impairment. This was indicated either by MMSE scores below the cut off for dementia of 23/24 (six patients), or by estimated premorbid current IQ discrepancies of greater than 15 points (six patients), or both (four patients). Carer ratings showed evidence of daily living skill failures typical of dementia in all patients; it is noteworthy that four patients were incontinent.
Background information and general intellectual measures in the patients
Six of the eight patients were age disoriented, four underestimating their age by 4–8 years, one overestimating it by 13 years, and one giving a “don't know” response. Some of these patients underestimated the current year (four patients) and the duration of their hospital stay (four patients), but there was never a clear pattern where temporal orientation errors were in keeping with the patient's subjective concept of his or her own age. All the age disoriented patients also failed non-temporal orientation items. There was thus only limited support for the view that schizophrenic disorientation has its core in temporal disorientation or that “time stands still” for such patients, as has been suggested.42 43
The patients' PANSS ratings for positive symptoms (delusions, hallucinations, and incoherence of speech), negative symptoms (lack of volition, poverty of speech, and flattening of affect), and general psychopathology (depression, anxiety, catatonic symptoms, miscellaneous psychotic symptoms, etc) are shown in figure 2, where they are compared with those of a large sample of 201 chronic schizophrenic patients collected by one of us.44 As expected, the eight patients had disorientation ratings which were at or above the upper limit of those for the sample as a whole. However, it is clear that these high disorientation scores were not associated with corresponding high levels of symptoms: positive symptoms and general psychopathology scores were unexceptional, and negative symptoms, although somewhat more marked, were not extreme.

Patients' scores on PANSS positive, negative, and general psychopathology scales in comparison with a sample of 201 chronic schizophrenic patients.
Neuropsychological testing was carried out on seven patients (the first language of patient 6 was not English, which would have affected his performance on many of the tests). The findings are shown in table 2. There was a pattern of scattered impairment on the tests of visual and visuospatial function, with the patients collectively failing nine of 35 tests. Impairment was most frequent on tests requiring planning (copying a complex figure) or higher order visual processing (silhouette identification). Performance on the language tests was patchy: there was relative preservation of syntax (two of seven patients failing the modified token test) coupled with more evidence of impairment in semantics (four of seven patients failing the graded naming test).
Patients' neuropsychological test scores
By contrast, the patients failed almost all the memory and executive tasks. Collectively, there were failures on 30 out of 34 of these tests. In many cases performance was drastically impaired, as indicated by scores below the 1st percentile or outside the normal range altogether.
The duration of the patients' cognitive impairment was not usually easy to determine. Onset of intellectual decline could be reasonably accurately dated in the one patient who did not have severe, chronic illness (patient 8). She was a 64 year old married woman who had had episodes of psychosis from the age of 34, but who showed good recovery between episodes to the extent that she lived at home and carried out some household duties. Two years before examination she underwent a severe worsening, with auditory hallucinations and catatonic symptoms which proved resistant to all treatment; during the course of this, disorientation became evident for the first time. Severe intellectual impairment had been present for at least 10 years in three patients (patients 3, 4, and 7). Although patients 3 and 4 showed a decline in IQ compared with premorbid estimates, they showed no obvious progressive change in cognitive status over this period. However, patient 7 had taken part in neuropsychological studies 6 years previously. Her previous and current scores are shown in table 3: initially, her MMSE score was 26, in the normal range, but this fell to 22, in the demented range. Memory and executive performance also showed deterioration over the same period: having initially been impaired on only one of four memory tests and none of three executive tests, she became impaired on all memory tests and and two out of three executive tests. Nevertheless, her WAIS IQ did not change over the period.
Changes in cognitive performance of patient 7 over 6 years
None of the patients showed abnormalities on any of the laboratory investigations listed above, with the exception of positive antinuclear antibodies in two patients. DNA binding was normal in both these patients. No clinical evidence of arteriopathy was present in any of the patients and only one patient showed ECG abnormalities, which consisted of minor ST changes only.
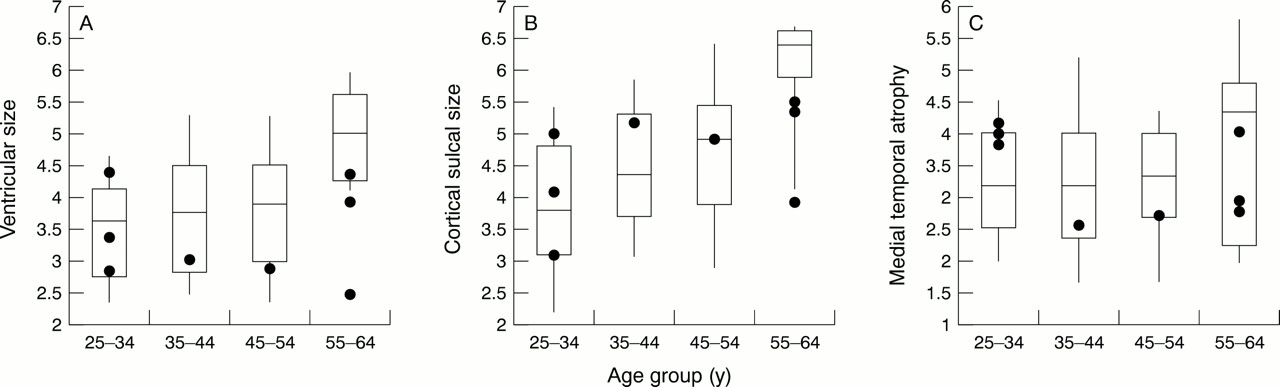
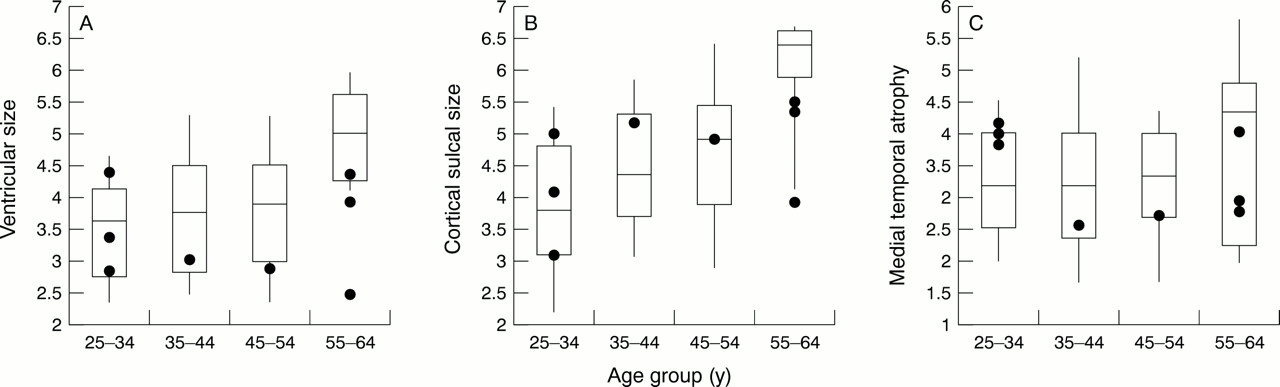
Brain CT scans were reviewed with a neuroradiologist and the findings are summarised in table 4. Clinically, the scans were reported as normal or showed only minor abnormalities, which would not be expected to affect cognitive status—for example, cavum septum pellucidum. Further analysis was undertaken by two independent raters using the CT rating scale for schizophrenia (CTRSS), an instrument designed to quantify sulcal widening and ventricular enlargement using a 1–7 scale for 11 separate regional measures.45 This scoring system is reliable, minimally affected by variability in scanning procedures, and gives accurate estimates of sulcal and ventricular sizes based on the ranges found in a large database of normal people and schizophrenic patients. The approach is similar to the CERAD neuroimaging protocol for dementia46; however, the range of reference photographs in the CTRSS is scaled for a wider range of age, but a narrower range of atrophy. Scores of 1 represent appearances in young normal control subjects, scores of 7 represent those for elderly schizophrenic patients.
Structural and functional imaging findings
The CTRSS measures for lateral ventricular size and cortical sulcal widening are shown in figure 3, where they are plotted against a database of 251 schizophrenic patients with a similar age range.45 It is evident that the changes fall well within the range seen in schizophrenia as a whole. Pairedt tests also failed to show significant laterality differences in the patients' sulcal or ventricular ratings. Atrophy of medial temporal structures has been found to provide a sensitive marker of Alzheimer's disease.47-49 Figure 3therefore also shows ratings for the medial temporal lobe size (calculated as the mean of ratings for temporal horn, suprasellar cistern, and temporal midbrain cistern); once again the eight patients' scores are unremarkable compared with the sample as a whole.
{kind=link}
{kind=link}
{kind=link}
Patients' lateral ventricular, sulcal, and medial temporal measures in relation to a sample of 251 schizophrenic patients.
Brain SPECT was available for six patients (scanning was unsatisfactory due to movement artefact in patient 2 and patient 7 did not consent to this procedure). As shown in table 4, the scans were reported clinically as abnormal in five, with frontal hypoperfusion or patchy perfusion, plus parietal hypoperfusion in two patients. To examine these findings further, the SPECT scans, together with scans of patients with Alzheimer's disease and healthy people, were reviewed blind by one of the authors (PMK) who is a consultant in nuclear medicine. Abnormalities were rated on a five point scale from normal (1) to unequivocally abnormal (5). Regions where there was probable (rating of 4) or definite (rating of 5) abnormality are indicated in table 4. There was a pattern of hypoperfusion which was variable across the sample, but which most often involved frontal and temporal regions.
Discussion
The patients in this case series not only had schizophrenia, but also showed disorientation, poor intellectual performance, and daily living skill failures up to and including incontinence, features which would normally point to an additional diagnosis of dementia. More rigorous diagnostic requirements for dementia were also met. The patients all had memory impairment plus deficits in other areas of cognitive function. They were all educationally normal before the onset of schizophrenia and most had worked as adults in jobs which required normal intelligence. They all showed evidence of intellectual decline from normal estimated IQ levels to low or even mentally handicapped levels of current IQ functioning. The only seeming difference from the more familiar forms of dementia was the lack of a progressive downhill course terminating in death. However, progression is not intrinsically necessary to the definition of dementia.50 Some dementias—for example, those after head injury or encephalitis—are static, and others may show only slow or imperceptible progression—for example, those complicating multiple sclerosis and epilepsy.
It seems unlikely that the patients in this study had known forms of dementia superimposed on schizophrenia. Tests for dementing illnesses diagnosable in life were all negative. These included metachromatic leukodystrophy which can sometimes present in late life.51The long duration of psychotic symptoms (9 to 30 years) also seems to preclude misdiagnosis of some other neurological diseases which can initially masquerade as schizophrenia but ultimately declare themselves with appearance of progressive dementia and neurological signs. The coincidental development of Alzheimer's disease, multi-infarct dementia, or cortical Lewy body disease in some of the older patients is difficult to exclude with certainty during life, and CT appearances may be deceptively normal in Alzheimer's disease.52However, there are reasons for doubting that the patients had any of these disorders: (a) Alzheimer's disease is rare in the presenile period; (b) medial temporal lobe atrophy was no greater in this series of patients than in schizophrenia as a whole; (c) multi-infarct dementia would be unusual in the absence of other evidence of vascular disease; and (d) all three dementias would be likely to progress rather than remain static over periods of observation ranging from 2 to 10 years. One further dementia, frontotemporal dementia, remains a realistic differential diagnosis: this commonly presents in the presenile period, may progress only slowly, and may show functional imaging abnormalities coupled with structural imaging appearances which remain normal for a long time.53-55 A counter argument, however, is that, on current evidence, psychotic symptoms are uncommon in frontotemporal dementia.55
It is also unlikely that the eight patients' disorientation and other signs of cognitive impairment could be attributed to distraction by psychotic symptoms, lack of motivation, poor cooperation, etc. In general, such factors are no longer regarded as credible explanations of cognitive impairment in schizophrenia.5 6 Positive symptoms were not present in severe form in the patients, and whereas they did show relatively high levels of negative symptoms, it would be difficult to argue that poor motivation could cause them to make errors on simple questions about orientation, or give rise to a pattern of preserved performance on some tests but impairment on others. Institutionalisation is also discredited as a cause of the severe cognitive deficits seen in schizophrenic patients chronically in hospital18 56 and in any case cannot account for the findings of this study, as only half of the patients were in long stay hospital care.
Neuroleptic medication, which all the patients had received for long periods, requires more serious consideration as a cause of their cognitive impairment. There is a consensus from many studies that neuroleptic drugs have at most minor deleterious effects on neuropsychological test performance in normal volunteers, and if anything they tend to improve performance in schizophrenic patients.57 58 The possibility that long exposure to these drugs could have a cumulative toxic effect on intellectual function has also been investigated: Owens and Johnstone14reconstructed the treatment records of 510 patients chronically in hospital and found no relation between intellectual test scores and lifetime neuroleptic exposure (or exposure to all other physical treatments except insulin coma). It can also be pointed out that age disorientation in schizophrenia was first documented in the late 1950s, when neuroleptic treatment had not become widespread or prolonged.17 42
Stevens et al 17 identified correlates of age disorientation in schizophrenia, including young age of onset, long duration of illness, and protracted inpatient stay. To some extent the patients in this study conformed to this pattern: they all had severe, intractable illnesses, most had a long duration, and some had become ill at a young or very young age. A further unexpected finding was an apparent excess of female patients. Nevertheless, the present study can do no more than hint at clinical and demographic features associated with dementia in schizophrenia, as the study was small and did not employ a formal case-control design. For the same reasons, it is not possible to be specific about the frequency of dementia in schizophrenia. Although eight patients (plus up to three more who were not investigated) could be found in a service containing about 200 chronic schizophrenic patients, such rates cannot be used to generate a prevalence figure without much more information about what leads patients to enter rehabilitation services and how typical these patients were.
The fact that the patients in this series showed severe intellectual deficits in the setting of unremarkable levels of psychotic symptoms, whereas other patients may show more severe symptoms without orientation being affected, suggests that schizophrenic cognitive impairment is an independent dimension of pathology within the disorder. This is in keeping with the conclusion of several correlational and factor analytical studies of schizophrenia. These have found only weak associations between neuropsychological test performance and overall psychopathology,59 little or no association with delusions and hallucinations, some degree of association with “disorganisation” symptoms (formal thought disorder and inappropriate affect), but a consistent association with negative symptoms.60-63 These last correlations, although statistically significant, are typically relatively low (of the order of 0.2–0.5), and it is clear that there is no one to one correspondence between presence of negative symptoms and presence of cognitive impairment.
The finding of levels of intellectual impairment amounting to dementia in schizophrenia does not in any way contradict the evidence that poor cognitive performance is a feature of the disorder which is sometimes present at onset9 64 and may be detectable before this.24 25 It merely suggests that in addition to such a “neurodevelopmental” pathology, there is a postmorbid decline. Where our findings are at odds with the rest of the literature is that most studies have failed to show that schizophrenic cognitive impairment progresses from first onset of illness, at least over the short term64 or medium term.65 The evidence on long term decline, however, is conflicting: for example, Hydeet al 66 found no progressive decline of MMSE scores across a group of schizophrenic patients divided into different age bands, but in a similar study Davidsonet al 16 found a linear decrease in MMSE scores with increasing age.
At present there is no obvious way of reconciling these contradictory findings; the paradox remains that some chronic schizophrenic patients show severe cognitive impairment which seems inherently unlikely to have been present throughout life, but direct evidence of deterioration during the acute or subacute stages of the disorder is lacking. It may be that cognitive impairment in schizophrenia needs to be understood as following neither a strict neurodevelopmental trajectory—as seen for example in autism—nor the simple neurodegenerative course of a progressive dementia. In this vein, Dwork et al 67 have speculated that a subtle neuronal pathology in schizophrenia reduces the normal “cognitive reserve” which protects against dementia and lowers the threshold for the appearance of clinical cognitive impairment. Such a process could be either neurodevelopmental, in which case it would interact with the normal age related brain degenerative changes to produce dementia at a higher rate than seen in the normal elderly population; or alternatively it might be slowly progressive and eventually give rise to dementia by itself in a few cases.
Neuropsychological testing of our severely cognitively impaired patients showed a pattern of predominant impairment in memory and executive function coupled with relative sparing of visual and visuospatial function. When impairment was found on these tests, it clustered in silhouette identification (which is sensitive to high level, semantic difficulties) and copying of a complex figure (which may also be impaired in patients with frontal lobe lesions, thought to reflect poor planning). Language was affected, where there were indications of impairment in semantics coupled with relative preservation of syntax. The overall pattern was similar to that seen in schizophrenia generally5 6 and is indicative of predominant frontal and temporal lobe dysfunction.68
In this patient group clinical signs of dementia were not accompanied by any marked structural brain abnormality. Clinical reports suggested cortical atrophy only in three patients, where it was mild, and comparison against a database of schizophrenic CT scans indicated that all the patients fell within the range of modest lateral ventricular enlargement and cortical sulcal widening seen in the disorder as a whole.69 70 In general, CT70 and MRI71 studies have not yielded consistent evidence for a relation between cognitive impairment and structural abnormality in schizophrenia. One study72 found that age disoriented patients had lateral ventricles which were significantly larger than those who were age oriented. However, another study22 73found no correlation between lateral ventricular size and either age disorientation or poor cognitive test performance. In our patients there was also little to suggest progression of CT abnormalities over periods of time up to 10 years, further arguing against any direct relation between cognitive decline and progressive loss of brain tissue. This is also in keeping with evidence from CT and MRI studies, which suggest that ventricular enlargement in schizophrenia is present early in the course of illness and does not progress, or at any rate not to an easily detectable degree.74
The leading candidate for functional imaging abnormality in schizophrenia, hypofrontality, has been found in only a minority of studies under resting conditions.71 75 Although the evidence is stronger for an association between hypofrontality and certain aspects of the schizophrenic clinical picture, such as negative symptoms and chronicity, the findings for neuropsychological deficits are limited and conflicting.71 The present study suggests that severe cognitive impairment in schizophrenia is accompanied by resting functional imaging abnormalities in the form of perfusion deficits affecting the frontal, temporal, and to a lesser extent parietal regions. These findings are preliminary and limited by small numbers and lack of control data, but even so the rate of abnormality seems to be higher than that usually found in schizophrenia—for example, in a study using SPECT and clinical ratings of perfusion deficits, Paulman et al 76 found frontal hypoperfusion in 38% and 33% (left and right), and temporal hypoperfusion in 33% and 43%.
The state of severe cognitive impairment evidenced by the patients in this study is clearly uncommon. However, such states seem to become frequent among elderly institutionalised schizophrenic patients, where up to two thirds have been found to have MMSE scores in the demented range.16 77 Postmortem studies on such patients have shown that Alzheimer's disease is diagnosable in less than 10%, and that there is no excess of multi-infarct dementia, Lewy body disease, Pick's pathology, or markers for brain injury.67 78-81These and other findings led Harrison82 to state that elderly schizophrenic patients with unequivocal, prospectively assessed dementia show no evidence of any known neurodegenerative disorder. Clearly, dementia in schizophrenia requires a novel neuropathological explanation. Further studies to determine its demographic and clinical correlates would also be desirable, and it would be interesting to explore its apparent similarities to frontotemporal dementia.
Acknowledgments
WGH was supported by a Vancouver Hospital Scientist Award. Dr J S Lapointe provided valuable consultation on structural imaging. The authors thank Mr A Healy for his assistance with white cell enzyme assays.