Article Text

Abstract
OBJECTIVES To examine the relation between social deprivation and the prevalence of epilepsy and associated morbidity using hospital activity data as a proxy.
METHODS The study was conducted in the health district of South Glamorgan, United Kingdom (population 434 000). Routinely available hospital data (inpatient and outpatient), an epilepsy clinic database, and mortality data underwent a process of record linkage to identify records relating to the same patient and to identify patients with epilepsy. Each patient was allocated a Townsend index deprivation score on the basis of their ward of residence. Age standardised correlations were calculated between deprivation score and prevalence of epilepsy, inpatient admissions, and outpatient appointments. Standardised mortality ratios (SMR) were also calculated. All analyses were performed on two cohorts: (1) all patients with epilepsy and (2) those patients with epilepsy without any underlying psychiatric illness or learning disability.
RESULTS The prevalence of epilepsy ranged between 2.0 and 13.4 per 1000 with a median of 6.7. There were positive correlations between social deprivation and prevalence in both populations: (1) r=0.75 (p<0.001) and (2) r=0.70 (p<0.001). After standardising for underlying prevalence there were also correlations for mean inpatient admissions: (1) r=0.62 (p<0.001), (2) r=0.59, (p<0.001) and for outpatient appointments: (1) r=0.53, (p=0.001) and (2) r=0.51 (p=0.001). The SMR for those deprived was (1) 1.66 (95% confidence interval (95% CI) 1.27–2.05) and (2) 1.80 (95% CI 0.71–1.67). For the population as a whole (with and without epilepsy) the SMR was 1.25 (95% CI 1.27–2.32).
CONCLUSION This study shows a strong correlation between the prevalence of epilepsy and social deprivation and weaker correlations between social deprivation and mean hospital activity.
- epilepsy
- social deprivation
- Townsend index
- record linkage
Statistics from Altmetric.com
The relation between ill health and social deprivation has been well documented.1 2 Previous studies dating nearly 60 years have showed that this finding remains valid for psychiatric illness3 4 although there is debate as to the direction of causality5 and the relation is specific to diagnosis.6
There have been few studies of epilepsy and social deprivation7 with attention instead concentrated on the indirect issues of employment accessibility and social adjustment.8-10 Patients with epilepsy endure higher levels of unemployment than the general population11-13and it would be expected that this will impact on deprivation. Unemployment is regarded as a key variable in all deprivation indices14-16 and has been identified independently as a strong indicator of health need.4 17 Patients with epilepsy are also more likely to have unqualified jobs18and consequently to be of a lower social class.12 13
It is likely therefore that a positive association between epilepsy and social deprivation will exist which may be increased by the confounding effect of psychiatric illness and learning disability. Epilepsy is well documented as a comorbidity of both these conditions.19-24
Determining the association between epilepsy and social deprivation is of benefit in assessing the need for healthcare provision for patients living in deprived areas. In addition, if a correlation is found to exist this may inform both the management and aetiology of the disease. In this paper we explore the relation between social deprivation and epilepsy in terms of prevalence and associated morbidity using routine data sources which have undergone record linkage. In an attempt to allow for the major comorbidities of epilepsy, we consider these variables for all patients with epilepsy and also for those without either psychiatric illness or learning disability.
Methods
The study population comprised the resident population in the area that until April 1996 constituted South Glamorgan Health Authority (SGHA), a health district with a population of 434 000 (1996 estimate).25 The area served by SGHA was divided administratively into 47 district wards. Since April 1996, SGHA has been incorporated into Bro Taf Health Authority. South Glamorgan is a largely urban county centred on the City of Cardiff, the capital of Wales. The demography of South Glamorgan is very similar to that of the United Kingdom as a whole for age, social class, and ethnicity.
DATA SOURCES, RECORD LINKAGE, AND IDENTIFICATION OF PATIENTS
Data for all inpatient admissions (1991–7), outpatient appointments (1991–6), and mortality (1993–7) for the resident population of South Glamorgan were available. In addition epilepsy clinic and local social services community learning disability databases were used. Details of these datasets are shown in the appendix.
These data underwent a process of record linkage to identify those records relating to the same individual patient and to identify those patients with diagnoses of epilepsy. The principle and process of record linkage has been discussed previously26 and has been used in previous studies.27 Briefly, partial identifiers (names, sex, date of birth, postcode, and address), were combined and matched using probabilistic algorithms. The discriminating power of each item was calculated and weighted for whether the identifier was common or comparatively rare. A composite matching score was then calculated.
Identification of patients with epilepsy
Patients with epilepsy were identified from four sources: (1) inclusion on the epilepsy clinic database, (2) an inpatient admission coded for epileptic seizure (ICD-9 345, ICD-10 G40) on routine inpatient data, (3) a diagnosis recorded on the learning disabilities hospital database, or (4) inclusion of epilepsy (ICD-9 345) as a primary or underlying cause of death on the mortality dataset.
By identifying unique patients with epilepsy, we were able to estimate the prevalence of epilepsy in each district ward based on 1996 population estimates derived from the 1991 census. We also generated the age standardised mean number of inpatient admissions per patient with epilepsy by district ward for all admissions, for admissions with a primary diagnosis of epilepsy, and for admissions with either a primary or subsidiary diagnosis of epilepsy. The mean number of all outpatient appointments was also calculated. All of these indices were standardised by age and correlated with the mean Townsend index of material deprivation per ward using Pearson's correlation coefficient.
The Townsend index has four key variables: (1) proportion of population of working age unemployed, (2) proportion of households without a car, (3) proportion of households overcrowded (defined as household with more occupants than rooms), and (4) proportion of households not owner occupied. A Townsend score of zero reflects the average for the United Kingdom. A positive Townsend score indicates material deprivation with a higher score representing a higher degree of deprivation. A negative Townsend score represents comparative affluence.
In addition we calculated the prevalence rate ratio of epilepsy for patients from socially deprived wards using the 10 wards with the highest Townsend scores and those with the lowest (the most affluent) as the reference population.
To analyse mortality we calculated the standardised mortality ratio for patients classified as deprived (positive Townsend score) compared with those who were not (negative Townsend score) using mortality data for 1996. This was cross referenced to our epilepsy dataset using a unique identifier generated by the record linkage process. Patients who had migrated from South Glamorgan during the year and died were not included.
To remove the confounding effect of psychiatric illness which, as mentioned above, has been shown to be a strong correlate of deprivation, all analyses were performed twice. We firstly considered all patients with epilepsy excluding those living in long term mental handicap hospitals and secondly a subset of this population excluding those known to have either coexisting psychiatric illness or learning disability. This was deduced from either (1) inclusion on a local authority learning disability database, (2) any inpatient admission or outpatient appointment coded in the mental handicap or psychiatric specialties, (3) an inpatient diagnosis of either mental handicap or psychiatric illness (ICD9 295–319, ICD-10 F00-F99), or (4) an underlying cause of death coded for mental handicap or psychiatric illness (ICD9 295–319).
Results
THE SAMPLE
For 1996, we identified a period prevalent population of 2943, a prevalence of 6.8 per 1000 population. After excluding those patients resident in the long term mental handicap hospital 2809 patients remained for population 1. After further excluding those with coexisting psychiatric illness or learning disability and those whose postcode could not be traced (fig 1), 2028 patients remained in population 2.

Derivation of epilepsy population.
PREVALENCE
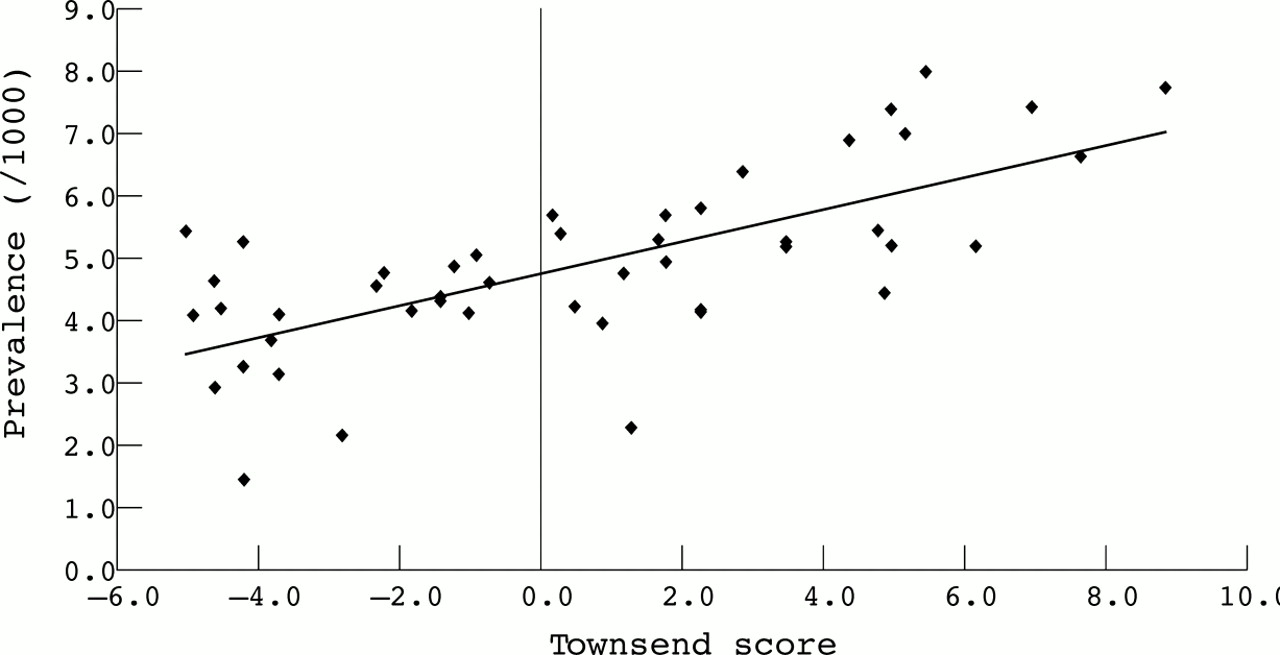
The age standardised prevalence of epilepsy by district ward ranged from 2.0 to 13.4 per 1000 population with a median value of 6.7. The correlation coefficient (r) between the assigned Townsend score and prevalence of epilepsy was 0.75 (p<0.001) for population 1 (fig 2) and 0.70 (p<0.001) for population 2 (fig 3).

Prevalence of epilepsy by deprivation of district ward (population 1).

{kind=link}
{kind=link}
{kind=link}
Prevalence of epilepsy by deprivation of electoral ward (population 2).
Positive correlations were also found within three broad age bands, less than 20 years of age (r=0.53, p<0.001) between 20–54 (r=0.66, p<0.001) and over 55 (r=0.43, p=0.002) for population 1 andr=0.45, (p =0.001),r=0.61 (p<0.001),r=0.19 (p=0.2) respectively for population 2.
The prevalence rate ratio of epilepsy (95% confidence interval (95% CI)) for those most deprived was 1.86 (1.29–2.67) for those less than 20 years of age, 2.04 (1.72–2.43) for those aged 20–54, and 1.41 (1.09–1.73) for those 55 and over. For patients without coexisting morbidity (population 2) the respective prevalence rate ratios (95% CI) were 1.76 (1.17–2.63), 1.86 (1.52–2.26), and 1.37 (1.09–1.73).
HOSPITAL ACTIVITY
There was also a positive correlation between hospital activity and social deprivation for patients with epilepsy after standardising for the underlying prevalence in each district ward. The rate of inpatient admissions for population 1 had the strongest correlation (r=0.62, p<0.001) with weaker correlations for those admissions with a primary diagnosis of epilepsy (r=0.39, p=0.007) or any diagnosis of epilepsy (r=0.43, p=0.002). These patterns were slightly weaker for population 2:r=0.59, (p<0.001) for all admissions,r=0.35 (p=0.016) for admissions with a primary diagnosis of epilepsy, and r=0.41, (p=0.004) for admissions with any epilepsy diagnosis. For outpatient appointments there were positive correlations for population 1 (r=0.53, p=0.001) and (0.51, p=0.001) for population 2.
MORTALITY
In 1996 there were 109 deaths for patients with epilepsy (population 1) and 62 for those patients who constituted population 2. The SMR for those patients classified as deprived compared with those classified as affluent was 1.66 (95% CI 1.27–2.05) and 1.80 (95% CI 1.27–2.32) for populations 1 and 2 respectively. For the population as a whole (those deceased with and without epilepsy) the SMR was 1.25 (1.20–1.30) comparing the deprived with the affluent district wards.
Discussion
This study indicates a strong correlation between the prevalence of epilepsy and material deprivation which seems largely independent of the presence of psychiatric comorbidity. In addition, there may be an association between social deprivation and hospital activity. Whereas these correlations were weaker, we standardised our admissions to ward prevalence. Studies using similar methods to consider psychiatric admissions have produced far stronger correlations but have used psychiatric admissions as the numerator and the total area population (psychiatric and non-psychiatric) as the denominator.4 6In these studies it is not clear, therefore, whether the observed relation with deprivation is between prevalence or excess mean admissions per psychiatric patient.
The excess use of hospital services by those from deprived areas may represent greater severity of morbidity but it might also indicate relatively worse control of epilepsy. However, the relation is stronger for all admissions rather than those with either a primary or underlying diagnosis of epilepsy. This may indicate that epilepsy related morbidity is less associated with social deprivation than other conditions. The relation between non-attendance at outpatient clinic and deprivation (table 1) may indicate a greater level of non-compliance with management regimes.
Correlations
By using record linkage techniques we have estimated a prevalent population. Due to the difficulties with diagnosing epilepsy, it is widely acknowledged that case ascertainment is problematic with the potential to both underestimate and overestimate cases.28 29 Patients may be unaware or unconcerned by minor seizures or may deliberately conceal seizures due to fear of stigmatisation. Cases may also be misdiagnosed30 resulting in both false negative and false positive diagnoses. In addition, not all patients will be seen in hospital. Recent studies31 32 have indicated that over 80% of patients are seen as outpatients at some time during their history and that over 25% are seen in any given year. Our outpatient data extends for 6 years and in addition inpatient data was also used. It is likely, however, that our data will be biased towards recently diagnosed cases and those requiring continuing, hospital based management.
As most of our data sources for patients with epilepsy are hospital based we may have discriminated towards those whose demand for hospital services is greater. If, as we have indicated, higher levels of service utilisation occur among those most deprived then it is possible that this may have led to greater non-identification of patients in the affluent wards and consequently a lesser overall correlation between prevalence of epilepsy and deprivation than we have reported. Conversely the relation between mean hospital activity and deprivation would be strengthened.
In addition there may be questions concerning the reliability of routinely generated data.
A recent study of acute cerebrovascular events, however, has shown that routine data is of equal sensitivity as a prospective disease register compiled using exhaustive methods although its positive predictability was lower.33 False positive cases of epilepsy may have occurred, especially from those cases identified through routine inpatient data, which has traditionally been regarded with suspicion. This, however, may be unjustified34 and, since the introduction of contracting into the United Kingdom health service, the quality of coding has improved considerably. We accept that some cases may have become quiescent, and as such our quoted figure which represents 1 year period prevalence will be a slight overestimate.
One factor which might skew our analyses is the provision of private health care which, it seems reasonable to assume, will have increased uptake among the most affluent wards. Data for these contacts were not available.
As we have defined epilepsy by prevalence rather than incidence it is accepted that this might overrepresent those cases which are current and which may therefore be a reflection of severity or non-compliance associated with social deprivation rather than the underlying incidence of the condition. Without data relating to incidence we were also not able to derive relative risks and thus within this paper we present relative prevalence ratios. It was not possible with the data available to comment on seizure type or severity and association with social deprivation.
The relation between prevalence and deprivation by age is surprising as it shows a positive relation with all ages. Although in adulthood it may be accepted that epilepsy impacts upon the patients' employment opportunities and causes them to drift down the social scale the same factors do not apply to those under 20 years of age. This is instructive in determining the direction of causality and may indicate that the aetiology of the disease is affected by factors related to material deprivation within the younger age groups.
The weaker correlations for patients in the older age group may reflect the diminishing effect of epilepsy as a predictor of social deprivation as many people in this age group will have retired and therefore not be susceptible to the social drift caused by enforced unemployment. Although in this age group epilepsy may present secondary to other conditions which may in themselves be positively related to social deprivation, the overall effect is ambiguous. Cerebrovascular disease, for example, has been shown to be related to social deprivation35 but this relation is stronger in the younger age groups and may be reversed in elderly people.36
In all age groups the relation between epilepsy and psychiatric illness is well documented. In population 2, however we excluded patients with coexisting psychiatric illness or learning disability. This not only avoided potential confounding but also removed the clustering of patients in small residential carer units. As we have assigned deprivation scores on the basis of residence this would have artificially skewed our analyses. Overall, however, we found little difference between the two populations with the exception of all cause inpatient admissions.
As with all studies in which a deprivation score is applied on a residential area basis it is necessary to be aware of the “ecological fallacy”, the incorrect assumption that all residents within a particular area will exhibit the aggregated characteristics of that area. None the less this study indicates that there is a relation between social deprivation with both the prevalence of epilepsy and excess morbidity and mortality for those patients with epilepsy. Further work is required to determine the direction of causality and in particular to determine which factors associated with deprivation are relevant.
Appendix 1: Datasets used for identification of patients with epilepsy
Acknowledgments
We thank Bro Taf Health Authority for providing routine data and Mr Leicester Gill (Unit of Health Care Sciences, University of Oxford) for help with the record linkage. CLIM was funded by a grant from Glaxo-Wellcome.