What do hospital consultants value about their jobs? A discrete choice experiment
BMJ 2003; 326 doi: https://doi.org/10.1136/bmj.326.7404.1432 (Published 26 June 2003) Cite this as: BMJ 2003;326:1432
- Cristina Ubach, research assistant1,
- Anthony Scott (a.scott{at}abdn.ac.uk), reader in health economics1,
- Fiona French, research and development officer2,
- Morag Awramenko, research fellow2,
- Gillian Needham, postgraduate dean2
- 1 Health Economics Research Unit, Institute of Applied Health Sciences, University of Aberdeen, Foresterhill, Aberdeen AB25 2ZD
- 2 NHS Education for Scotland, Forest Grove House, Aberdeen AB25 2ZP
- Correspondence to: A Scott
- Accepted 12 June 2003
Abstract
Objective To examine the strength of hospital consultants' preferences for various aspects of their work.
Design Questionnaire survey including a discrete choice experiment.
Setting NHS Scotland.
Participants 2923 hospital consultants in Scotland.
Main outcome measures Monetary valuations or prices for each job characteristic, based on consultants' willingness to pay and willingness to accept extra income for a change in each job characteristic, calculated from regression coefficients.
Results The response rate was 61% (1793 resspondents). Being on call was the most important attribute, as consultants would need to be compensated up to £18 000 (30% of their average net income) (P < 0.001) for a high on-call workload. Compensation of up to £9700 (16% of their net income) (P < 0.001) would be required for consultants to forgo opportunities to undertake non-NHS work. Consultants would be willing to accept £7000 (12% of net income) (P < 0.001) in compensation for fair rather than good working relationships with staff, and £6500 (11% of net income) (P < 0.001) to compensate them for a shortage of staff. The least important characteristic was hours of work, with £562 per year (0.9% of their net income) (P < 0.001) required to induce consultants to work one extra hour per week. These preferences also varied among specific subgroups of consultants.
Conclusions Important information on consultants' strength of preferences for characteristics of their job should be used to help to address recruitment and retention problems. Consultants would require increased payment to cover more intensive on-call commitments. Other aspects of working conditions would require smaller increases.
Introduction
Ambitious targets have been set for future consultant numbers, backed up by increases in medical school places and unprecedented increases in NHS expenditure. Consultants' workloads have increased as a consequence of the European Working Time Directive, the “new deal” for junior doctors, and more general trends such as the increasing proportion of female doctors and the expected impact of more flexible and family friendly working. Changes to the consultants' contract with the NHS are also likely to have major effects on recruitment, retention, morale, and productivity.1 2
Consultants' own preferences for aspects of work that they value have not been rigorously examined. This is crucial information if a new contract is to meet their objectives and those of the NHS. We examined the preferences of hospital consultants for several aspects of their jobs.
Methods
Discrete choice experiments
To quantify consultants' strength of preference for job characteristics we used a discrete choice experiment to derive the monetary value of each job characteristic, which can be interpreted as a “price.”3 4 Discrete choice experiments are being used within health economics (and in environmental and transport economics) as a method of establishing prices or valuations for goods and services that otherwise have no price because a market does not exist or function properly.5 The lack of prices is a problem as prices convey information about the strength of individuals' preferences for these goods and services. Although consultants do receive a price for their work in the form of a salary plus other payments, ongoing problems with recruitment and retention suggest that the current price does not reflect adequate compensation for several aspects of their job. This may also be because the current price is set nationally, with little local flexibility. The discrete choice experiment derives prices that reflect more closely the preferences of consultants for various aspects of their job.
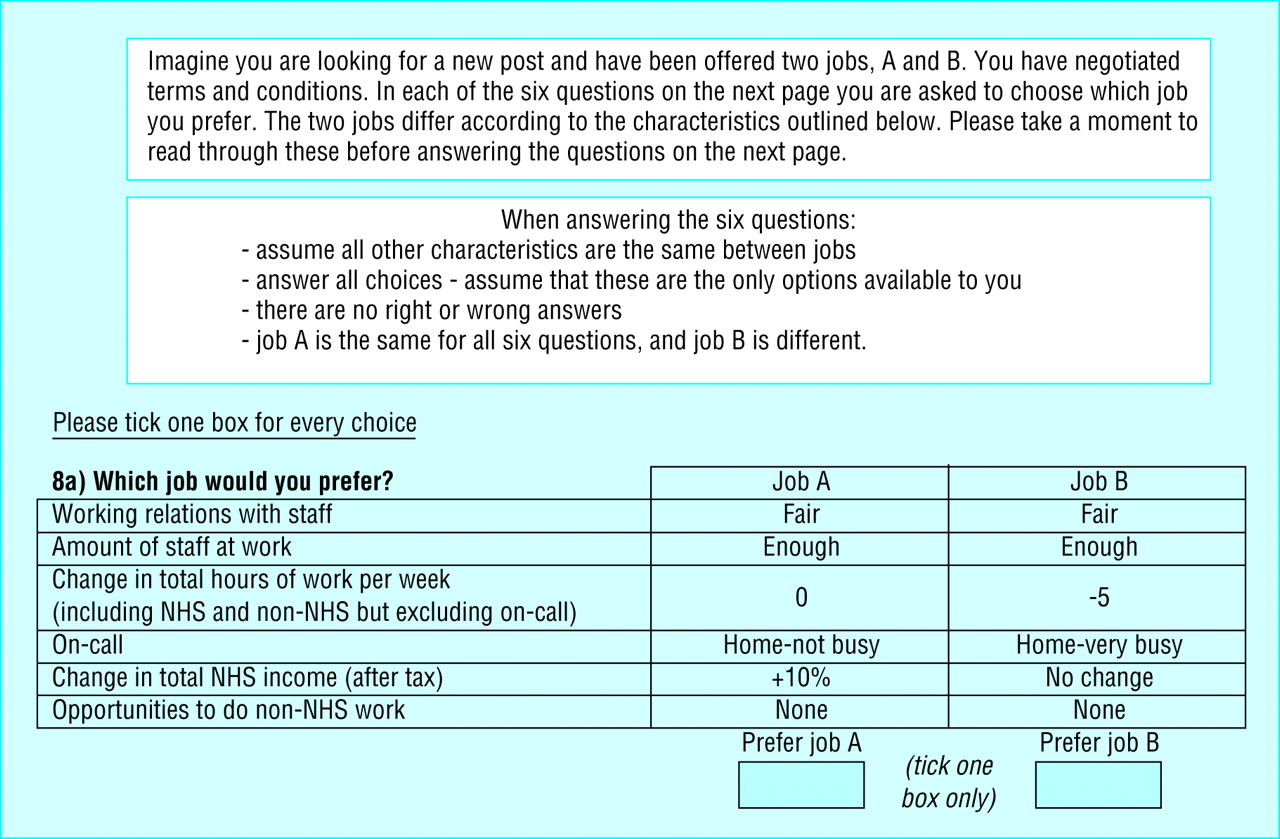
The discrete choice experiment was part of a larger questionnaire used in a study of flexible working in NHS Scotland, from the perspectives of non-training grade doctors. The experiment presented each respondent with several choices between different types of job (figure). We decided on the included job characteristics using data from existing literature, interviews with 14 consultants, and four focus groups with consultants (table 1). Realistic levels for each job characteristic were assigned to each attribute.6

{kind=link}
Attributes and levels used for questionnaire on consultants' preferences for work
Paired scenarios
The scenarios were organised into pairs (see figure for example). If all combinations of levels were used it would result in a full factorial design of 576 possible scenarios. We reduced this to a more manageable level of 16 scenarios by using a fractional factorial experimental design.7 These were placed in pairs by having the same scenario appear in each pair (a constant scenario) and pair this with every other scenario. With a high number of attributes this makes the choices easier to understand and also helps to maintain the statistical properties of the design.5
We undertook the pairing to ensure that the statistical properties were satisfied such that the results did not depend on the way scenarios were paired.8 9 We tested the face and content validity of the questionnaire in the first pilot survey that was sent to all consultants who participated in the interviews and focus groups. A second pilot questionnaire was sent to a random sample of 56 consultants. Fifteen choices may lead to respondent fatigue, so they were divided across three versions of the questionnaire such that all attribute levels occurred with approximate equal frequency in each version. An extra choice was added to each version of the questionnaire to test for internal consistency. This involved presenting a choice with levels such that everyone should choose the same job. Each questionnaire therefore contained six pairs of scenarios. The questionnaire also contained other questions on workload, contractual details, income, and family circumstances. We obtained standard demographic information from the data contained in the sampling frame.
Participants
The questionnaire was posted to all hospital consultants in Scotland, except for those who had completed the pilot questionnaire and those who were known to have retired or died. The sample was obtained from the Information and Statistics Division of the Scottish Executive Health Department. The three versions of the questionnaire were randomly allocated to consultants. The questionnaire was posted in July 2001, followed by one reminder.
We used STATA 7.0 with a probit regression model to analyse the data as the dependent variable was binary (0,1)—that is, whether the respondent chose job A or job B.10 Explanatory variables were the differences between the levels of each job characteristic. A random effects probit model was used to account for the potential correlation in responses between the six choices completed by each respondent. Three separate regression models were estimated. The first included the six main job characteristics only. The second model examined how preferences varied according to respondents' demographic and family characteristics, and the third model examined how preferences varied across specialties and location. The second and third models included the six main attributes and several interaction term variables that multiplied each job characteristic with each variable of interest (such as hours worked x sex). This measures the extent to which the preference for hours of work (for instance, the regression coefficient in the first model) depends on sex. For the second and third models we used a backward stepwise approach and variables with the highest P values (P > 0.1) were excluded from the model, one at a time.
The monetary valuation of each attribute or price is given by the trade-offs between income and each job characteristic that are implicit when respondents make choices. If consultants had several job offers, or even one job offer where they are making comparisons with their current post, they would be willing to forgo an amount of one characteristic in one job offer to have more of another characteristic in another job. The discrete choice experiment is designed to replicate partly the decision making process when consultants actually choose a job. The trade-offs are quantified by dividing each regression coefficient by the regression coefficient for income. This gives the equivalent amounts of income respondents are prepared to give up or accept for a change in the level of another characteristic.
Results
Respondents
The final response rate was 61% (1793/2923). We excluded the 38 respondents who did not answer the discrete choice experiment questions. Of the 1755 remaining questionnaires, there were 105 inconsistent responses (5.9%), which is relatively low compared with data from previous studies. This left a final sample for analysis of 1650 consultants. These were evenly distributed across each version of questionnaire and were broadly representative (tables 2 and 3).
Descriptive statistics of consultants in study. Figures are numbers (percentage) of consultant unless stated otherwise
Income of NHS consultants in Scotland. Figures are numbers (percentages)of consultants
Table 4 shows the results of the regression analysis. The significant value of the regression coefficient (r=0.38, SD 0.023) suggests that a random effects specification was appropriate and that the six responses from individual consultants were correlated (log likelihood −3110; 22% of 1s and 97% of 0s predicted correctly, pseudo R2=0.19). Consultants prefer a job with fewer hours at work, good rather than fair relations with staff, enough staff rather than a shortage, high increase in annual income, and opportunities to do non-NHS work. These broadly confirm the theoretical validity of the technique. For on-call commitment for the same location consultants prefer “not busy” to “very busy,” and for the same amount of work they prefer to be at home rather than in hospital.
Main effects model, indicating consultants' strength of preference for job from 1650 consultants and 8199 observations‡
Priorities
The most important characteristic was on-call. If consultants' on-call changed from “home-not busy” to “residential-very busy,” they would need to be compensated by the equivalent of £18 000 a year or 30% of their current NHS income. For a change from “home-not busy” to “home-very busy,” they would require remuneration of about £13 400 or 22% of their income. A move from “home-not busy” to “residential not busy” was valued at £12 150 or 20% of their current income.
The next most important characteristic was the opportunity to undertake non-NHS work. Consultants would need to be compensated £7300-9700 (12-16% of their current average net income) if they could no longer do non-NHS work. Having good relationships with staff and enough staff at work were also important, with consultants willing to accept £7000 (11.7% of their income) to compensate them for fair rather than good working relations and £6500 (10.8%) to compensate them for a shortage of staff rather enough staff.
Consultants would require an extra £562 a year (0.9% of their current net income) or £11.70 a week to compensate them for working one extra hour a week, indicating that working extra hours is less important than the other characteristics. However, the importance depends on the number of extra hours worked. For hours worked to become more important than the amount of staff at work, consultants would need to work an extra 11 hours a week (£6520/£562).
Effect of personal circumstances
Preferences (and prices) for these characteristics differed depending on consultants' own circumstances, such as sex, age, health, whether they work part time, family circumstances, specialty, income, and location. Table 5 shows the regression results for the interactions with the consultants' personal characteristics (r=0.39, P < 0.0001; log likelihood −2739; 20.9% of 1s and 92.2% of 0s predicted correctly, pseudo R2 (% fall in log likelihood compared with random effects model with consistent term only)=0.21). The specialty interactions are available from the authors.
Main effects plus interactions with age, sex, household income, health, and no partner no children model*, with monetary valuations‡in 1497§consultants and 7447 observations
The preferences of consultants who had partners and children were no different from those of consultants who did not have partners or children, indicating that having a family does not influence the relative importance of job characteristics. Thus the value of working an extra hour (or giving up an hour of leisure time) was the same for consultants with families as it was for those without. Younger consultants were less likely to prefer on-call commitments than older consultants, particularly for “home-very busy” and “residential-not busy.” This implies that the price for younger consultants for on-call would be higher than for older consultants. Younger consultants were more likely to value an increase in annual income compared with older consultants. Consultants who reported better health placed a higher valuation on good relations with staff. Those who reported poorer health were likely to prefer working fewer hours a week and placed a lower weight on unlimited opportunities to do non-NHS work.
Female consultants placed more weight than male consultants on having good relations with staff and having enough staff. Women preferred to work fewer hours a week and so would need to be compensated more to work extra hours than their male colleagues. Women were less likely to want to undertake non-NHS medical work, preferred less on-call, and placed less weight on opportunities to do non-NHS work. These results were independent of the effect of having to care for children and imply that as the proportion of female consultants increases in the future it will be more difficult to maintain the current level of hours worked and on-call commitments without increases in remuneration.
Consultants who preferred to work longer hours had higher household incomes, as did those who preferred “very busy” residential on-call and those who preferred to undertake non-NHS work. This implies that some consultants prefer to work hard and have higher incomes.
Consultants' work circumstances
The weight placed on attributes, and their prices, also differed across specialties. Compared with those working in general medicine, surgeons placed more importance on opportunities to undertake non-NHS work, whereas paediatricians placed less importance on such opportunities. Compared with consultants in general medicine consultants in surgery, anaesthetics, obstetrics and gynaecology, oral medicine, and emergency medicine also thought that “very busy” and residential on-call was more important. This suggests that these consultants view a high and residential on-call workload as an important part of their jobs. Compared with consultants in general medicine consultants working in anaesthetics, obstetrics and gynaecology, oral medicine, and emergency medicine have stronger preferences for an increase in income. Those working in anaesthetics also place a lower weight on having good relations with staff. The importance of having enough staff did not differ across specialties.
There were no differences in the strength of preferences for job characteristics between urban and rural areas. Compared with consultants working in major cities, consultants working in towns placed less weight on having good relations with staff and preferred to work fewer hours a week. This is likely to reflect the preferences of consultants working in teaching and non-teaching hospitals. Finally, consultants' current income did not influence the monetary valuations of job characteristics.
Discussion
Consultants have the strongest preferences for being on call. The value of a high on-call workload was £18 000, interpreted as the extra amount they would need to be paid. Compensation of up to £9700 would be required to forgo opportunities to undertake non-NHS work. Consultants would be willing to accept £7000 in compensation for fair rather than good working relationships with staff and £6500 to compensate them for a shortage of staff. The least important characteristic was hours of work, with £562 a year required to induce consultants to work one extra hour per week.
Given a priori expectations, the results are plausible and support the theoretical validity of the technique. Discrete choice experiments have generally been shown to be reliable and valid, although this does depend on the context.5 However, the choices presented to the consultants were hypothetical, and further research needs to compare these results with results based on actual behaviour. Nevertheless, the hypothetical nature of the exercise has its advantages over using actual data as the researcher has complete control over the experimental design and this ensures statistical robustness. Discrete choice experiments also allow the inclusion of characteristics that do not exist yet, such as having no opportunities to do non-NHS work and residential on-call. Two studies have suggested that monetary values from discrete choice experiments are sensitive to the range of monetary attributes included in the choices.12 13 Other studies have suggested that respondents may not trade-off attributes but use more simple decision heuristics.14 15
These are important topics of ongoing research. The money values should therefore be interpreted with these issues in mind.
Implications of results
The questionnaire was designed before detailed proposals for the new consultant contract were published. However, the results still have important implications for the remuneration of consultants. From the first ballot of consultants across the Uited Kingdom about the new contract it was evident that English consultants were more concerned with the implication that managers would ask them to work extra antisocial hours. Working an extra hour a week was the least important characteristic for Scottish consultants, although the importance changed as the number of extra hours increased. However, the discrete choice experiment did not examine the importance of working additional antisocial hours.
The contract proposals also outlined several measures that will help to ensure that NHS work will be given priority over non-NHS work. Our results show that any reductions in opportunities to undertake non-NHS work would require consultants to be compensated by up to 16% of their net income. Scottish consultants undertake less private work than English consultants, and so this value may be comparatively low. However, they may still value the option to undertake such work in so far as it reflects professional autonomy.
On-call is the attribute that consultants value most highly. It is difficult to measure the burden of on-call because it is necessary to account for frequency, intensity, location, time of day, and subsequent time off. To maintain simplicity we included only intensity and location. The contract proposals indicate that those who are on an on-call rota with a high frequency should receive a supplement of up to 8% of their basic salary. Our results show that consultants would require at least 20% of their net NHS income for “very busy” on-call. Although these two figures are not directly comparable, the figure of 8% seems too low.
Conclusions
The pricing of the various elements of the consultant contract will ultimately be the result of negotiation, and prices generated from discrete choice experiments should act as estimates of such prices, given the caveats of the study. We have shown how it is possible to derive such prices that are based on consultants' own preferences between different hypothetical jobs. The results also have implications for the recruitment and retention of consultants because if negotiated national prices are lower than individual consultants' valuations the consultant is likely to remain dissatisfied with work and seek compensation in other ways, such as doing more private work, working part time, or leaving. The proposed contract also introduced flexibility for local employers to pay recruitment and retention premiums. These results may be useful to local employers in setting such premiums. Given the importance of NHS workforce policy in meeting NHS goals, the paucity of research on this issue is surprising. Further research is required on the effects of job characteristics on decisions in the labour market.
What is already known on this topic
There has been little rigorous research on the preferences of hospital consultants for various aspects of their job
Such information is crucial for the development of evidence based policies to enhance recruitment and retention and to change behaviour
What this study adds
According to a discrete choice experiment consultants feel most strongly about on-call conditions and freedom to do non-NHS work
In Scotland, the least important consideration was additional hours of work, although the importance changed as the number of hours increased
Estimates of required compensation measure the strength of consultants' preferences for job characteristics, and can be used as a basis for determining levels of remuneration
Footnotes
-
 Contributors All authors contributed to the design of the questionnaire and interpretation of results. FF and MA undertook piloting and focus group work. CU designed and analysed the discrete choice experiment under the supervision of AS. CU and AS drafted the paper. GN, FF, AS, Linda Leighton-Beck, and Jill Mollison were involved in the design of the project. Helen Coutts assisted with piloting. Kim Walker and Linda Leighton-Beck provided overall project management for the flexible workforce study. Jill Mollison provided statistical advice and Jane Andrew assisted with data analysis. AS, FF, GN, LLB and JM were grantholders. AS is the guarantor.
Contributors All authors contributed to the design of the questionnaire and interpretation of results. FF and MA undertook piloting and focus group work. CU designed and analysed the discrete choice experiment under the supervision of AS. CU and AS drafted the paper. GN, FF, AS, Linda Leighton-Beck, and Jill Mollison were involved in the design of the project. Helen Coutts assisted with piloting. Kim Walker and Linda Leighton-Beck provided overall project management for the flexible workforce study. Jill Mollison provided statistical advice and Jane Andrew assisted with data analysis. AS, FF, GN, LLB and JM were grantholders. AS is the guarantor. -
Funding Scottish Council for Postgraduate Medical and Dental Education (now NHS Education for Scotland). The Health Economics Research Unit is funded by the Chief Scientist Office of the Scottish Executive Health Department. The views in this paper are those of the authors. The guarantor accepts full responsibility for the conduct of the study, had access to the data, and controlled the decision to publish.
-
Competing interests None declared.