Are antibiotics effective for acute purulent rhinitis? Systematic review and meta-analysis of placebo controlled randomised trials
BMJ 2006; 333 doi: https://doi.org/10.1136/bmj.38891.681215.AE (Published 03 August 2006) Cite this as: BMJ 2006;333:279
- 1 Department of General Practice and Primary Health Care, University of Auckland, Private Bag 92019, Auckland, New Zealand
- Correspondence to: B Arroll
- Accepted 7 June 2006
Abstract
Objective To systematically review the evidence for the effectiveness of antibiotics in acute purulent rhinitis (many guidelines advise against their use on the basis of one study that showed no effect).
Data sources Medline, Embase, Cochrane Register of Controlled Trials, and reference lists of retrieved articles.
Review methods Meta-analysis of data from double blind randomised placebo controlled trials comparing antibiotics with placebo for acute purulent rhinitis (duration less than 10 days).
Results Seven studies were retrieved; four contributed data on benefits of antibiotics, and four contributed data on harms of antibiotics. The pooled relative risk of benefit for persistent purulent rhinitis at five to eight days with antibiotics was 1.18 (95% confidence interval 1.05 to 1.33). The numbers needed to treat ranged from 7 to 15 when the pooled relative risk was applied to the range of control event rates. The relative risk for adverse effects with antibiotics was 1.46 (1.10 to 1.94). The numbers needed to harm for adverse effects ranged from 12 to 78. No serious harms were reported in the placebo arms.
Conclusions Antibiotics are probably effective for acute purulent rhinitis. They can cause harm, usually in the form of gastrointestinal effects. Most patients will get better without antibiotics, supporting the current “no antibiotic as first line” advice.
Introduction
Acute purulent rhinitis (a runny nose with coloured discharge) is a common feature of the common cold. One study of the natural history of acute rhinitis stated that clear and purulent rhinitis both lasted about two weeks,1 although the duration might vary with the prevalence of specific infecting organisms. Nevertheless, the presence of purulent nasal discharge has repeatedly been shown to be an important determinant of the prescribing of antibiotics for respiratory tract infections for both adults and children.2–4 Indeed, one study found that purulent nasal discharge was a stronger predictor of antibiotic prescribing than any other characteristic of patients.4
Most guidelines recommend that antibiotics should not be used for this condition,5 6 citing one study that found no evidence that antibiotics reduce the duration of acute purulent rhinitis.7 However, a recent larger study reported that treatment with amoxicillin reduced the duration of purulent rhinitis, although it found no significant difference between the groups in terms of general improvement in symptoms.8
Concern exists about overuse of antibiotics leading to bacterial resistance.9 Most antibiotics are used in primary care, so this is where any reduction needs to take place. As antibiotic use is often based on the presence of purulent rhinitis, determining whether antibiotics are effective in this condition is important. Our aim was to systematically search for studies on the effectiveness and harms of antibiotics for acute purulent rhinitis and to do a meta-analysis and review of the articles.
Methods
Inclusion and exclusion criteria—We included controlled trials in which the intervention was an antibiotic compared with a placebo for patients with acute purulent rhinitis. The primary outcomes were persistence versus clearance of purulent rhinitis and any adverse events reported. We defined “acute” as most patients having less than 10 days with this symptom. We chose 10 days to separate our review from the Cochrane review of chronic purulent rhinitis, which used 10 days as the starting point for the inclusion criteria.10 The patients could be seen in any setting equivalent to general practice (that is, they could self refer). We did not limit the age of participants but excluded patients who were considered, in the original studies, to have sinusitis.
Searches—We searched (to 13 November 2005) Medline, Embase, and the Cochrane controlled trials register, using the terms “purulent and (rhinitis or nasopharyngitis or rhinorrhea or rhinorrhoea).” An alternative search on the rhinitis terms and randomised controlled trial found no further relevant papers. We also considered all the papers in the Cochrane review on antibiotics for the common cold and acute purulent rhinitis and the review on antibiotics for acute maxillary sinusitis.11 12 We contacted the authors of published controlled trials of antibiotics for the common cold to see if they were aware of any unpublished studies. We imposed no language restriction.
Selection, validity assessment, and data abstraction—Each author independently assessed the titles and abstracts of potential papers; assessed the included trials for the quality of randomisation, concealment of allocation, co-interventions, losses to follow-up, intention to treat analysis, degree of blinding, and extraction of data; and scored the trials by using the Jadad scale.13 Disagreement between the authors was readily resolved by discussion.
Quantitative analysis—We used RevMan 4.2 (Nordic Cochrane Centre, Rigshospitalet, 2003) to assess the pooled relative risks and 95% confidence intervals.14 We present results of both random effects and fixed effects models for the main analysis; for simplicity, we present results of only the fixed effects model for other analyses.
Results
Search results and study characteristics
Figure 1 shows the search strategy, and the table summarises the studies found. The searches found five papers on purulent rhinitis (De Sutter 2002, Howie 1970, Taylor 1977, Todd 1984, and Vogt 1966).7 8 15–17 A further paper (Herne 1980) reported a reduction in rhinitis without stating if the rhinitis was purulent or clear18; we therefore did analyses both including and excluding this study. Another study reported a reduction in rhinitis, also without stating if this was purulent or clear, but we did not include it as the numerical data were not suitable for pooling.19 Howie used illnesses, not individual patients, as the denominator and hence is not pooled in the analysis of benefit from antibiotics (none found).15 However, the adverse effect reports were based on individual patients and so contribute to the harms analysis. Vogt found a significant improvement with antibiotic but was excluded as the antibiotic treatment was topical and compared with a locally active agent rather than placebo, an oral antibiotic was given to “most patients” in both groups, and the group allocation is not explained.17

{kind=link}
Studies included in quantitative analysis
Taylor (and Vogt) included only children, De Sutter included children and adults, and the other studies included only adults. Three studies reported purulent rhinitis without further explanation.7 15 16 De Sutter relied on the clinical decision of the recruiting doctors, although we noted that 53-56% of participants reported unilateral facial pain8; the other studies did not report the incidence of unilateral facial pain.
Quantitative analyses
The pooled effect for the studies contributing data specifically on purulent rhinitis shows a significant benefit from antibiotics at five to eight days (fig 2)—relative risk 1.18 (95% confidence interval 1.05 to 1.33, random effects); 1.21 (1.08 to 1.35, fixed effects). If data from Herne are included as purulent rhinitis, the relative risk is 1.21 (1.09 to 1.34, fixed effects). Using a relative risk of 1.18, the numbers needed to treat for a benefit from antibiotics ranged from seven for a baseline rate of 0.8516 20 to 15 for a baseline rate of 0.38.7
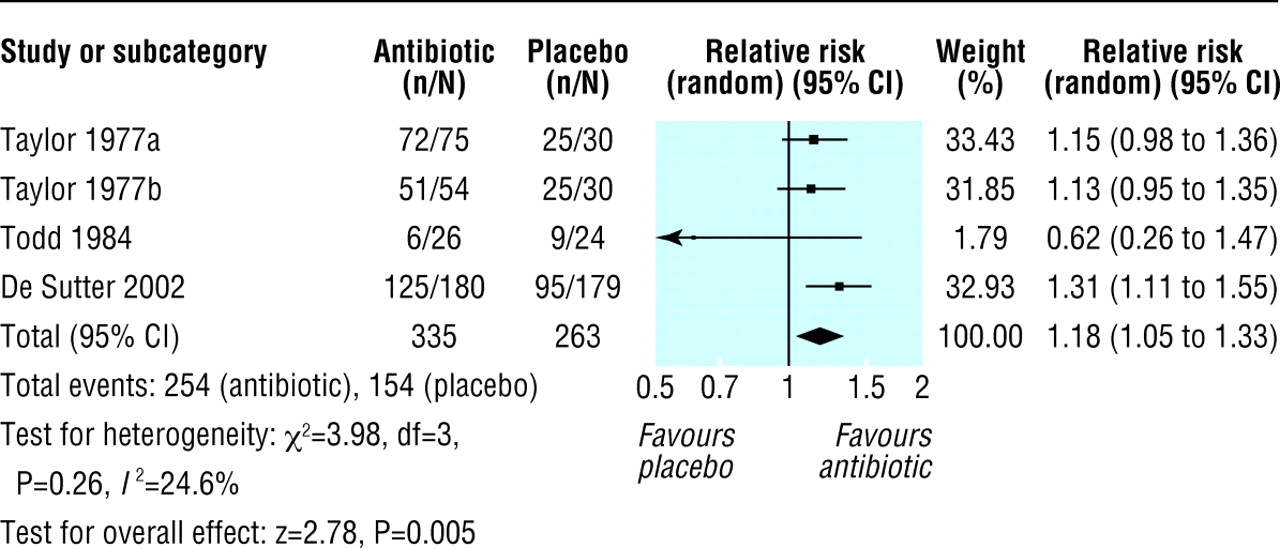
Meta-analysis of studies of outcomes of purulent rhinitis at five to eight days, antibiotic versus placebo (Taylor 1977a is co-trimoxazole arm; Taylor 1977b is amoxicillin arm)
{kind=link}
Various antibiotics were used: demethylchlortetracycline in Howie (1970), amoxicillin and co-trimoxazole in Taylor (1977), cefalexin in Todd (1984), and amoxicillin in De Sutter (2002). Pooling the two studies that used amoxicillin gives a relative risk of 1.26 (1.11 to 1.45, fixed effects).
The pooled relative risk for adverse effects was 1.46 (1.10 to 1.94, fixed effects), obtained from four studies.7 8 15 16 The numbers needed to harm ranged from 12 to 78 for control event rates in the statistically significant studies (0.1898 to 0.02815). The harms were mainly gastrointestinal and a small number of rashes.
A funnel plot suggests a paucity of small studies with small or no effects. All of the included studies scored five out of five on the Jadad scale.
Discussion
The findings from this study indicate that antibiotics for acute purulent rhinitis may be beneficial. Harms attributed to antibiotics were mainly vomiting, diarrhoea, and abdominal pain but also included rashes and hyperactivity (table). No more serious harm occurred in the placebo arm in any of the trials, which fits with the clinical notion that this is not a serious condition. At best, a number needed to treat of seven means that six patients get no benefit for every one who gets benefit. Furthermore, the number needed to treat for benefit from antibiotics (7-15) overlaps with the number needed to harm (12-78). Our results are consistent with the Cochrane review of chronic purulent rhinitis, which found a benefit for antibiotics (calculated as a reduced risk of persistent purulent rhinitis), with a pooled relative risk of 0.75 (95% confidence interval 0.61 to 0.92) and a number needed to treat of nine (at the mean control event of 0.46).10
Several of the studies were not of high quality yet scored well on the Jadad scale. None of the studies used an intention to treat analysis, which is not a requirement of the Jadad scale. As various terms are used for acute purulent rhinitis, we cannot be sure that we retrieved all the relevant articles. We found four of the studies in our Cochrane review of antibiotics for the common cold. Although the trend of results is towards an effect of antibiotics, the funnel plot indicates that some publication bias may exist. The studies also used different antibiotics, and the only clearly non-significant study used cefalexin.7 The relative risk from pooling the two amoxicillin studies was statistically significant, so amoxicillin may be preferred if any antibiotic is to be used.
The difference between sinusitis and acute purulent rhinitis is not always clear, and involvement of the sinus mucosa in the common cold may be the norm.21 We noted that between 53% and 56% of the participants in De Sutter (2002) had unilateral facial pain.8 In one study of purulent rhinitis of greater than 10 days' duration (and therefore excluded from this analysis), all participants had to be free of abnormalities on their facial x rays.22 In this study, azithromycin was significantly more effective than placebo in clearing purulent rhinitis. It seems that antibiotics may help purulent rhinitis, with or without the presence of sinusitis. Any future studies, however, should specifically assess the presence of sinus infection.
Our findings differ from the received wisdom in terms of the effectiveness of antibiotics for acute purulent rhinitis. This highlights the dangers of relying on one study (Todd)7 to decide on the effectiveness of a treatment when other studies show a different effect. Our summation would be to suggest initial management by non-antibiotic treatments or “watchful waiting,” and that antibiotics should be used only when symptoms have persisted for long enough to concern parents or patients. In this case, antibiotic treatment may be considered, given that the harms were usually gastrointestinal adverse effects and that individual patients may be aware of their own ability to tolerate specific antibiotics. Our findings are consistent with the review on antibiotics for chronic purulent rhinitis, and we do not feel that more randomised controlled trials on this subject are warranted. Thus we support the current guidelines in their advice not to use antibiotics but arrive at this point by taking into account the evidence, the benefits, and the harms of both treating and not treating.
What is already known on this topic
General practitioners often prescribe antibiotics for an acute upper respiratory tract infection when the rhinitis is purulent
Most guidelines recommend against using antibiotics for this condition, but this advice is based on one study
What this study adds
Review of seven papers indicates that antibiotics are probably effective for acute purulent rhinitis
This is not a sufficient reason to use antibiotics, however, as no serious adverse events occurred in the placebo group
Footnotes
-
Contributors Both authors reviewed the abstracts resulting from the search, extracted the data, and wrote the paper. BA did the analysis and is the guarantor.
-
Funding The initial Cochrane review “Antibiotics for the common cold” (1998) was funded by the Charitable Trust of the Auckland Faculty of the Royal New Zealand College of General Practitioners. This specific review was not funded by any external agency. The authors' salaries were from University of Auckland staff funding.
-
Competing interests: BA is a member of the Future Forum, an educational foundation funded by AstraZeneca UK, and a committee member of the Pharmac seminar series (Pharmac is the New Zealand government funding agency for drugs).