Association of bacteria and viruses with wheezy episodes in young children: prospective birth cohort study
BMJ 2010; 341 doi: https://doi.org/10.1136/bmj.c4978 (Published 04 October 2010) Cite this as: BMJ 2010;341:c4978
- Hans Bisgaard, professor1,
- Mette Northman Hermansen, medical doctor1,
- Klaus Bønnelykke, senior scientist1,
- Jakob Stokholm, research doctor, PhD student1,
- Florent Baty, statistician1,
- Nanna Lassen Skytt, junior scientist1,
- Julia Aniscenko, research technician2,
- Tatiana Kebadze, technician2,
- Sebastian L Johnston, professor2
- 1The Copenhagen Prospective Studies on Asthma in Childhood; Health Sciences, University of Copenhagen, and The Danish Pediatric Asthma Centre; Copenhagen University Hospital, Gentofte, Ledreborg Allé 34, DK-2820 Gentofte, Copenhagen, Denmark
- 2Department of Respiratory Medicine, National Heart and Lung Institute, MRC and Asthma UK Centre in Allergic Mechanisms of Asthma, and Centre for Respiratory Infection, Imperial College London, UK
- Correspondence to: H Bisgaard Bisgaard{at}copsac.com
- Accepted 12 July 2010
Abstract
Objective To study the association between wheezy symptoms in young children and the presence of bacteria in the airways.
Design Birth cohort study.
Setting Clinical research unit in Copenhagen.
Participants Children of asthmatic mothers, from age 4 weeks to 3 years, with planned visits and acute admissions to the research clinic.
Main outcome measure Frequency of bacteria and virus carriage in airway aspirates during wheezy episodes and at planned visits without respiratory symptoms.
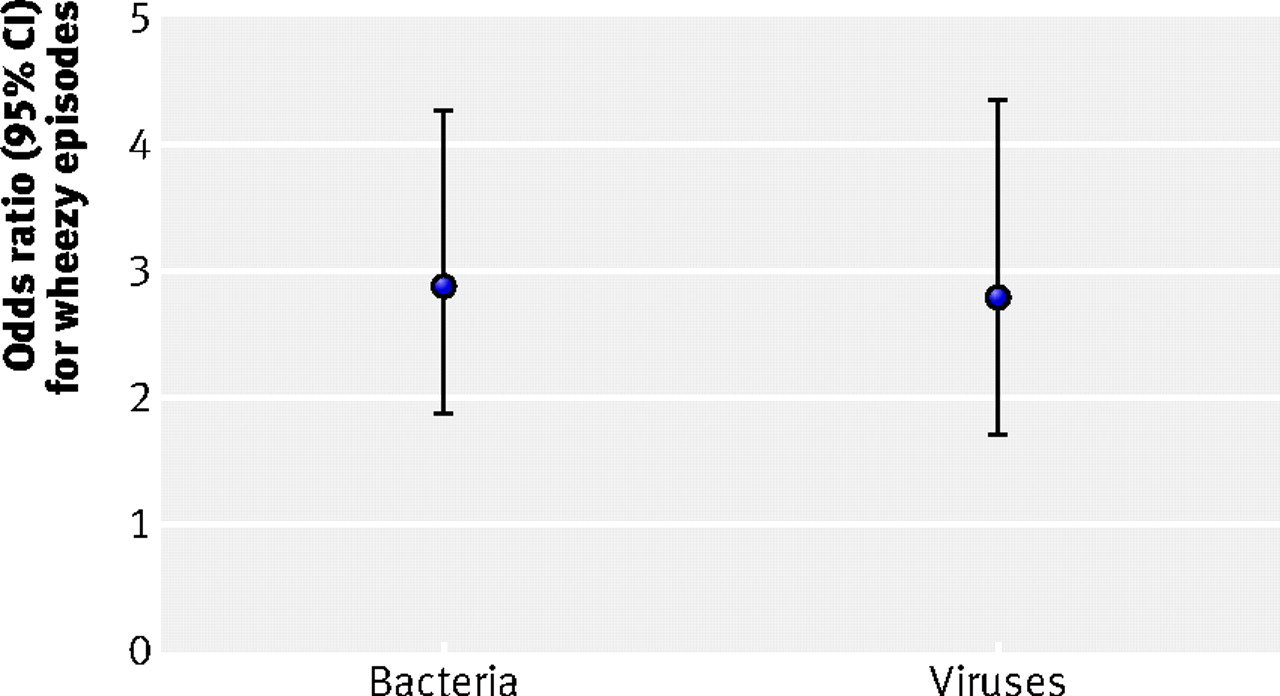
Results 984 samples (361 children) were analysed for bacteria, 844 (299 children) for viruses, and 696 (277 children) for both viruses and bacteria. Wheezy episodes were associated with both bacterial infection (odds ratio 2.9, 95% confidence interval 1.9 to 4.3; P<0.001) and virus infection (2.8, 1.7 to 4.4; P<0.001). The associations of bacteria and viruses were independent of each other.
Conclusion Acute wheezy episodes in young children were significantly associated with bacterial infections similar to but independent of the association with virus infections.
Introduction
Recurrent wheezy episodes in young children are the major reason for use of paediatric healthcare resources1 and represent an important unmet need for improved treatment strategies.2 Virus infections have been repeatedly and consistently associated with wheezy episodes,3 4 5 leading to the common use of the term viral wheeze.6 7 8 9
A recent survey of preschool children in Europe and the United States found that antibiotics were among the most commonly prescribed drugs for wheezy episodes in this population.10 Yet no studies have suggested that bacterial infections are associated with wheezy episodes in young children and no randomised controlled trials have reported the clinical efficacy of antibiotics for such episodes. Current guidelines for the treatment of wheezy episodes in preschool children recommend that antibiotics should not be given routinely.6
In this study we determined if common pathogenic bacteria were associated with acute wheezy episodes in children and whether any association was independent of virus infection. The children were prospectively examined for common airway pathogenic bacteria and viruses from age 4 weeks to 3 years during wheezy episodes and outside of such episodes as a part of the Copenhagen Prospective Study on Asthma in Childhood. To validate the pathogens detected, we also investigated the association of infections with clinical pneumonia.
Methods
The Copenhagen Prospective Study on Asthma in Childhood is a clinical study following a birth cohort of 411 children born in the Copenhagen area.11 12 13 Infants of mothers with a history of doctor diagnosed asthma were included at four weeks of age between August 1998 and December 2001. Children were excluded if born before 36 weeks of gestation or if they had a history of mechanical ventilation, congenital disease, or respiratory tract symptoms.
Oral and written informed consent was obtained from both parents of participating children. History was collected online during visits to the study’s clinical research unit and entered into a database. Measurements were entered into the database and double checked against source data, after which the database was locked.
The Copenhagen Prospective Study on Asthma in Childhood is an ongoing cohort study, but this report is based on a nested study during the first three years of life when children were sampled for airway bacteria and viruses during episodes of acute respiratory tract symptoms and at planned visits without lower respiratory tract symptoms.
Acute respiratory tract symptoms
We defined wheezy episodes from daily symptom diaries as three consecutive days of wheeze, at which point parents were asked to bring their child to the research unit.11 12 13 Wheeze was recorded as a composite dichotomised score (yes or no) together with use of rescue treatment (β2 agonist). The parents were taught to record symptoms, with emphasis on the lower airways. Wheeze was translated to the parents as any symptom that severely affected their child’s breathing, such as noisy breathing (wheeze or whistling sounds), shortness of breath, or persistent troublesome cough affecting the sleep or activity of the child. The parents received a book on asthma-like symptoms and treatment in young children (www.copsac.dk/content/parents-reading). The doctors at the research clinic collected and reviewed the diary cards at the half yearly visits.
Objective wheeze was diagnosed by a doctor at the research clinic and defined as audible wheeze, prolonged expiration, or ronchi by auscultation. Clinical pneumonia was diagnosed from tachypnoea, fever, and auscultation but before cultures had been obtained and independent of radiography.
Study design
The children visited the research clinic every six months as well as for acute respiratory tract symptoms, including wheezy episodes for three days (as predefined from diaries), clinical pneumonia, or other episodes of respiratory distress. This algorithm encouraged the parents to bring their child to the research clinic instead of the family doctor for such acute respiratory symptoms. At each acute visit up to age 3 years the children were examined by doctors trained in paediatrics and clinical research for diagnosis and treatment of any acute respiratory symptom episode in accordance with predefined standard procedures. The children received a standardised physical examination, including auscultation of the lungs.11 12 13 Hypopharyngeal aspirates were obtained for routine bacterial cultures and nasopharyngeal aspirates for virus identification.
Aspirates were also taken from the same children at the scheduled one year visit if they lacked lower respiratory tract symptoms or only had fever and upper respiratory tract symptoms.
Bacterial cultures
A doctor at the clinic aspirated the hypopharynx under aseptic conditions with a soft suction catheter passed through the nose. Aspiration was done intermittently assuring no suction was applied during retraction through the oropharynx and nasopharynx. The catheter was flushed with 1 ml of saline into a vessel to flush out secretions from the tube. Samples were transported at room temperature to the microbiology laboratories within two hours of collection. Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Streptococcus pyogenes, and Staphylococcus aureus were identified according to standard procedures.14
Positive bacterial cultures obtained during wheezy episodes were termed “infection” and positive bacterial cultures obtained without wheeze as “colonisation.” We excluded samples from children who had taken antibiotics within the past week.15
Detection of viruses and atypical bacteria
A doctor at the clinic aspirated the upper rhinopharynx under aseptic conditions with a soft suction catheter. We used polymerase chain reaction of nasopharyngeal samples to detect picornaviruses (mostly rhinoviruses); respiratory syncytial virus; coronaviruses 229E and OC43; parainfluenza viruses 1-3; influenza viruses AH1, AH3, and B; human metapneumoviruses; adenoviruses and bocavirus; and the two atypical bacteria Mycoplasma pneumoniae and Chlamydophila pneumoniae, as described.16 Bocavirus was detected on 2 μl random primed cDNA by polymerase chain reaction primers HBOV 01.2 TAT-GGC-CAA-GGC-AAT-CGT-CCA-AG and HBOV 02.2 GCC-GCG-TGA-ACA-TGA-GAA-ACA-GA with the cycling conditions 94°C, 56°C, and 72°C each for 20 seconds for 35 cycles. Positive control was complete coding genome of bocavirus plasmid DNA.
Viruses detected during wheezy episodes were defined as infection and viruses identified from children without wheeze were defined as virus shedding.
Bias and confounding
We adjusted for age of the children at sampling to control for bias from age differences between those attending for planned visits and those for acute wheezy episodes. A proportion of children had missing data on samples at the one year visit, primarily because the protocol was started after the beginning of the cohort study. We therefore considered these missing data as randomly distributed and did not compare the characteristics of children with or without samples at one year. As viruses are well known triggers of wheeze and a potential confounder of the association between bacteria and wheeze, we controlled for viruses in bacteria samples and bacteria in virus samples by including both in the multivariate analyses.
Statistical analyses
We used logistic regression with generalised estimating equation to assess differences in the presence of bacteria and viruses in samples from children with wheeze and those without wheeze. In our modelling we assumed a working independence correlation structure, not an unstructured correlation structure. We did not use any statistical criterion for the selection of the “best” correlation structure, but we could measure that in our data, the generalised estimating equation estimates eventually only scarcely depended on the correct choice of the correlation structure, as tested using different structures (independent, exchangeable, and first order autoregressive).
Analyses were adjusted for age at examination and for bacteria and viruses present in the same sample in the respective analyses of independent effects. P values, 95% confidence intervals, and interaction between bacteria and viruses were estimated by a robust Wald test based on the independence working generalised estimating equation approach taking repeated measurements of each child into account. We used a sandwich estimator for the estimation of the covariance matrix of the regression coefficients. All analyses were done using the R statistical software (version 2.7.0) including the package geepack.
Results
The birth cohort study included 411 children. The clinical follow-up rate of the cohort was 95% at age 1, 90% at age 2, and 85% at age 3.
Table 1⇓ shows the study base selection of samples of cases analysed for bacteria and viruses during the non-wheezy periods, cases of clinical pneumonia, and wheezy episodes.
Study base selection of samples from young children with clinical pneumonia, wheezy episodes, and periods without wheezy symptoms, analysed for viruses and bacteria
A total of 984 samples (361 children) were analysed for bacteria, 844 (299 children) for viruses, and 696 (277 children) for both viruses and bacteria. Bacterial cultures were obtained from 705 respiratory episodes; 74 samples were excluded from the group of cases because antibiotics had been taken within the past week, 87 because the sample was taken for an episode of less than three days or symptoms were judged to be caused by infection in the upper airways (including pseudocroup), 144 represented episodes with signs of clinical pneumonia, and the remaining 400 were collected during wheezy episodes.
Viruses were analysed in samples from 757 respiratory episodes; 95 were excluded from the group of cases because the sample was taken for an episode of less than three days or symptoms were judged to be caused by infection in the upper airways (including pseudocroup), 181 represented episodes with clinical pneumonia, and the remaining 481 were collected during wheezy episodes.
Web extra figure 1 shows the distribution of number of wheezy episodes with airway sampling per child. Most of the children had three or fewer wheezy episodes. Web extra figure 2 shows the distribution of samples taken during wheezy episodes according to age group. Most of the samples were from children aged 6-18 months. The type of bacteria cultured from samples during wheezy episodes was noticeably associated with age (see web extra figure 3). Colonisation shifted from a majority of S aureus in the first months of life to S pneumoniae, H influenzae, and M catarrhalis being the most commonly detected bacteria later.
Control samples from children without wheeze or other respiratory symptoms in the preceding week consisted of 279 samples analysed for bacteria and 87 analysed for viruses. Eighty one of these control samples were obtained from children with symptoms of a cold (n=47), otitis media (n=24), or fever (n=10). Table 2⇓ shows the distribution of bacteria and viruses during the non-wheezy periods, cases of clinical pneumonia, and wheezy episodes.
Distribution of bacteria and viruses during periods of no wheeze, signs of clinical pneumonia, and wheezy episodes. Values are percentages (numbers) unless stated otherwise
Bacterial infection and acute wheezy episodes
Wheezy episodes were significantly associated with H influenzae, M catarrhalis, and S pneumoniae overall (odds ratio 2.9, 95% confidence interval 1.9 to 4.3, P<0.001; figure⇓ and table 3⇓). The association was significant for H influenzae and M catarrhalis individually but not for S pneumoniae.

Association of viruses and bacteria with wheezy episodes in young children
{kind=link}
Association between bacteria and viruses and wheezy episodes in children up to age 3 years
Restricting the analysis to episodes with objective wheeze at the clinical examination (n=142) did not materially change the estimated association between bacterial infection and wheeze (2.4, 1.3 to 4.2; P=0.005), neither did restriction of the analysis to specimens with ciliated columnar epithelium from 134 non-wheezy episodes and 303 wheezy episodes (2.4, 1.3 to 4.4). Also, the association remained significant and with similar effect estimates when virus infection was included as a covariate in the more restricted population with both data (2.5, 1.0 to 6.2; P=0.049) and with no significant interactions (P=0.32). Restricting to children with four episodes or fewer increased the estimates.
Clinical pneumonia was strongly associated with H influenzae, M catarrhalis, and S pneumoniae (5.6, 2.4 to 13.0; P<0.001). Restricting the analysis of association between clinical pneumonia and bacteria to specimens with ciliated columnar epithelium (134 non-wheezy and 114 clinical pneumonia) did not materially change the estimated association (5.9, 2.1 to 17.0; P<0.001). Also, the association remained significant when virus infection was included as a covariate in the restricted population with both data (2.9, 1.2 to 7.3; P=0.02). The association was significant for S pneumoniae, H influenzae, and M catarrhalis individually, whereas S aureus showed no significant associations with either clinical pneumonia or wheezy episodes.
Viral infection and acute respiratory episodes
Wheezy episodes were significantly associated with viral infection (at least one of picornavirus, respiratory syncytial virus, coronavirus, parainfluenzavirus, influenza virus, human metapneumoviruses, adenovirus, or bocavirus) (odds ratio 2.8, 95% confidence interval 1.7 to 4.4, P<0.001; table 3). When the analysis was restricted to episodes with objective wheeze at the clinical examination (n=180), a similar association was seen between viral infection and wheeze (3.7, 2.1 to 6.6; P<0.001). The association was unaffected by bacteria as covariate (2.8, 1.6 to 4.9; P<0.001) and with no significant interactions (P=0.37). Clinical pneumonia was significantly associated with infection with any of the eight types of virus (4.2, 2.4 to 7.4; P<0.001). The association remained significant when bacteria were included as covariate (4.5, 2.3 to 8.7; P<0.001).
Atypical bacterial species and acute respiratory episodes
Atypical bacteria were detected in 2% of samples from children with wheezy episodes, 1% from children with clinical pneumonia, and none from children without wheeze. The presence of atypical bacteria was not analysed further.
Discussion
Acute wheezy episodes in children up to age 3 years were significantly associated with bacterial infection. Viral infection was also associated with wheezy episodes, with similar but independent effects. Both bacteria and viruses were also associated with clinical pneumonia.
Strength and weaknesses of the study
A major strength of this study was the clinical surveillance of a birth cohort attending the research clinic and not other healthcare facilities. Clinical diagnosis and sampling were done at the clinic by experienced study doctors in accordance with standard procedures. This approach reduced the risk of misclassification of illness and variation in sampling quality. The children were brought to the clinic for diagnosis of acute respiratory episodes, including wheeze and clinical pneumonia. Although the differentiation between the clinical presentations of wheeze and clinical pneumonia may be contested, the children were assessed by the same doctors in accordance with standard operating procedures; the sampling for viruses and bacteria was independent of such a distinction, and the clinical diagnosis was independent of microbiological outcomes.
Another strength of this study was the monitoring of wheezy symptoms in daily diaries. This assured that wheezy episodes with a predefined burden of symptoms led to clinic visits. Results were validated by restricted analysis of episodes with objective wheezing verified by auscultation by the attending doctor.
That all mothers had a history of asthma may have improved the validity of their observations of wheezing in their children.
The longitudinal study design allowed for wheezy children to act as their own controls when without wheeze.
This is the first prospective clinical cohort study to investigate both bacterial and viral infections simultaneously in wheezy episodes in children using standard bacterial cultures and sensitive molecular methods for virus detection. Bacterial cultures from hypopharyngeal aspirates were routinely collected as part of this evaluation, with epithelium from the lower respiratory tract present in most samples. It is a strength that bacteria and viruses were identified both in wheezy episodes and in cases of clinical pneumonia. The doctors at the clinic distinguished clinical pneumonia from wheezy episodes on the basis of the presence of tachypnoea, fever, and crepitation on auscultation without wheeze in accordance with standard operating procedures. This is traditional clinical semantics building on scarce evidence, but we know of no better distinction. These clinical entities may be difficult to separate in clinical practice but the independent associations of viruses and bacteria were similar whether the presentation was dominated by clinical signs of pneumonia or by wheeze.
To avoid bias in the analysis we allowed children with episodes of upper respiratory tract symptoms and fever in the control group. We tested if bacteria and viruses are associated with wheezy episodes and the relevant control group was therefore children without such symptoms. Had we excluded children with all symptoms from the control group we would have inflated the risk while introducing a bias that might have resulted in a difference between groups that was due to association between microbes and such upper respiratory tract symptoms or fever. The exclusion or inclusion of upper airway symptoms from the control group did not materially change the conclusions of the statistical analyses.
The association remained significant and with similar effect estimates when we included virus infection as a covariate in the more restricted population with both data (odds ratio 2.5; 95% confidence interval 1.0 to 6.2; P=0.049) and with no significant interactions (P=0.32). The results were also robust to restriction of the analyses to children with fewer episodes than the median number.
The rate of bacterial colonisation in the Copenhagen Prospective Study on Asthma in Childhood was similar to that reported in previous cohort studies,17 18 19 although S aureus seemed slightly more common in our cohort, which may have been due to the high rate of breast feeding.20
The anatomical origin of the bacteria cultured is uncertain. Ciliated columnar epithelium arose from the lower respiratory tract in 60% of samples from 1 year olds with no wheeze and 76% from episodes with wheeze. Restricting analyses to specimens with ciliated columnar epithelium did not, however, materially change the results.
A limitation of our findings was that the investigations were carried out in a high risk population. The selection for maternal asthma and exclusion of premature babies limit the generalisability of the findings, which need replication in population based studies.
It is a limitation of this and other studies on respiratory symptoms in young children, that symptoms are reported second hand and with no available terminology that communicates specific meaning in lay terms. We put much emphasis on training and supervising parents in the understanding of asthma related symptoms. Our definition of wheezy episodes (symptoms severely affecting breathing, such as noisy breathing (wheeze or whistling sounds); shortness of breath; or persistent troublesome cough affecting sleep or activity) was validated by our previous reports on significant associations to known risk factors, including genetics.13 21 22
Furthermore, our study design only allowed a significant association to be shown between bacteria and wheezing symptoms adjusted for viruses but could not definitively prove the causative role of bacteria. This could only be done in a controlled randomised trial of antibacterial treatment. Indeed, this is similar to the role of viruses, which is only proved to the extent of association.
Meaning of the study
To our knowledge this is the first prospective study using good quality sampling and detection methods to analyse the roles of both bacterial and viral infections during wheezy episodes and periods with no wheeze within the same cohort of young children.
Viral infection is closely associated with acute exacerbations of asthma.4 5 Viruses were identified in 65% of wheezy episodes in the children in this study and in 40% of samples during periods without respiratory symptoms and with similar distribution among types in wheezy and non-wheezy children. The similarity in distribution of virus types in wheezy children and asymptomatic children suggests that the type of virus itself is not causally related to symptoms. Similarly, bacteria were more commonly found in wheezy episodes but with similar distribution when comparing young children with and young children without wheezy episodes.
A recent clinical trial showed telithromycin to be effective in the treatment of acute exacerbations of asthma in adults,23 and clarithromycin alleviated the symptom burden, reduced the risk of readmission for respiratory syncytial virus related bronchiolitis,24 and reduced levels of inflammatory cytokines in children with recurrent wheeze.25 A study of long term therapy (six weeks) with azithromycin in stable asthma also showed significant clinical benefits.26 It is unclear if such benefits are related to an effect on atypical bacteria, general antibacterial effects, or anti-inflammatory properties.23 27 Furthermore, adults with asthma had an increased risk of severe pneumococcal disease28 as well as impaired innate immune responses to bacterial lipopolysaccharide.29 Whether these observations are relevant to this study in children requires further elucidation.
Our findings should not be confused with our previous observation of an association between colonisation of the airways with pathogenic bacteria at 1 month of age and development of asthma years later.13 The current study reports an association between acute wheezing symptoms and presence of bacteria at the time of wheezing, a relation unrelated to the colonisation of neonates.
Clinical trials with antibiotic therapy will be required to determine whether this increased detection of bacteria during wheezy episodes has clinical effects that are amenable to modification by appropriate therapy. If bacteria can be confirmed to be contributing to wheezy episodes in young children, this may have an important impact on treatment. This discovery may also contribute to an understanding of the disappointing results from trials of anti-asthma therapies in wheezing illness in early childhood.2
Conclusion
We found a significant association between bacterial infection of the airways and acute wheezy episodes in young children. This association was independent of viral infection suggesting that bacteria may contribute independently to the burden of wheezy symptoms. The clinical relevance of bacteria for wheezy episodes should be studied in randomised controlled trials of antibiotic treatment in this setting.
What is already known on this topic
Viral infections are associated with acute wheezy episodes in young children
What this study adds
Bacterial infections are significantly associated with acute wheezy episodes in young children similar to but independent of the association with viral infections
Notes
Cite this as: BMJ 2010;341:c4978
Footnotes
We thank the participating children and parents, the Copenhagen Prospective Study on Asthma in Childhood study teams, and Tobias Allander for his assistance with the polymerase chain reaction of bocavirus.
Contributors: HB was responsible for the integrity of the work, from conception and design to conduct of the study; the acquisition, analysis, and interpretation of the data; and drafting of the manuscript. He had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. HB is guarantor. MNH contributed to the data acquisition, data analyses and helped write the manuscript. KB and JS contributed to data analyses and interpretation and helped write the manuscript. FB did the statistical analyses. NLS contributed to data acquisition. SLJ was responsible for the analyses of the viruses and helped write the manuscript. JA and TK contributed to the analyses of viruses. All authors provided important intellectual input and approved the final version of the manuscript.
Funding: The Copenhagen Prospective Study on Asthma in Childhood is funded by private and public research funds (see www.copsac.com). The study is supported by the Lundbeck Foundation, the Pharmacy Foundation of 1991, Augustinus Foundation, the Danish Medical Research Council, and the Danish Pediatric Asthma Centre. The funding agencies had no role in the study design; the conduct of the study; data collection and management; data analysis; or the preparation, review, or approval of the manuscript.
All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any company for the submitted work; no financial relationships with any companies that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: This study was approved by the ethics committee for Copenhagen (KF 01-289/96 and KF 11-107/02) and the Danish Data Protection Agency (2008-41-1754).
Data sharing: The technical appendix, statistical code, and dataset are available from the corresponding author at Bisgaard{at}copsac.com.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.