Myocardial infarction and stroke associated with diuretic based two drug antihypertensive regimens: population based case-control study
BMJ 2010; 340 doi: https://doi.org/10.1136/bmj.c103 (Published 25 January 2010) Cite this as: BMJ 2010;340:c103
- Inbal Boger-Megiddo, fellow trainee1,
- Susan R Heckbert, professor of epidemiology1,
- Noel S Weiss, professor of epidemiology2,
- Barbara McKnight, professor of biostatistics3,
- Curt D Furberg, professor of public health sciences4,
- Kerri L Wiggins, data manager and analyst1,
- Joseph A C Delaney, postdoctoral fellow3,
- David S Siscovick, professor of medicine and epidemiology1,
- Eric B Larson, executive director and senior investigator5,
- Rozenn N Lemaitre, research scientist1,
- Nicholas L Smith, associate professor of epidemiology1,
- Kenneth M Rice, assistant professor of biostatistics3,
- Nicole L Glazer, research scientist1,
- Bruce M Psaty, professor of medicine and epidemiology1
- 1Cardiovascular Health Research Unit, University of Washington, Seattle, WA 98101, USA
- 2Department of Epidemiology, University of Washington, Seattle, WA 98195-7236
- 3Department of Biostatistics, University of Washington, Seattle, WA 98195
- 4Department of Public Health Sciences, Wake Forest University School of Medicine, Winston-Salem, NC 27157-1063
- 5Center for Health Studies, Group Health Cooperative, Seattle, WA 98101-1448
- Correspondence to: B M Psaty psaty{at}u.washington.edu
- Accepted 14 October 2009
Abstract
Objective To examine the association of myocardial infarction and stroke incidence with several commonly used two drug antihypertensive treatment regimens.
Design Population based case-control study.
Setting Group Health Cooperative, Seattle, WA, USA.
Participants Cases (n=353) were aged 30-79 years, had pharmacologically treated hypertension, and were diagnosed with a first fatal or non-fatal myocardial infarction or stroke between 1989 and 2005. Controls (n=952) were a random sample of Group Health members who had pharmacologically treated hypertension. We excluded individuals with heart failure, evidence of coronary heart disease, diabetes, or chronic kidney disease.
Exposures One of three common two drug combinations: diuretics plus β blockers; diuretics plus calcium channel blockers; and diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers.
Main outcome measures Myocardial infarction or stroke.
Results Compared with users of diuretics plus β blockers, users of diuretics plus calcium channel blockers had an increased risk of myocardial infarction (adjusted odds ratio (OR) 1.98, 95% confidence interval 1.37 to 2.87) but not of stroke (OR 1.02, 95% CI 0.63 to 1.64). The risks of myocardial infarction and stroke in users of diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers were slightly but not significantly lower than in users of diuretics plus β blockers (myocardial infarction: OR 0.76, 95% CI 0.52 to 1.11; stroke: OR 0.71, 95% CI 0.46 to 1.10).
Conclusions In patients with hypertension, diuretics plus calcium channel blockers were associated with a higher risk of myocardial infarction than other common two drug treatment regimens. A large trial of second line antihypertensive treatments in patients already on low dose diuretics is required to provide a solid basis for treatment recommendations.
Introduction
Untreated high blood pressure is strongly associated with myocardial infarction, stroke, and heart failure. The findings of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) suggested that low dose diuretics are superior to calcium channel blockers and angiotensin converting enzyme inhibitors as first line treatment for the prevention of one or more forms of cardiovascular disease in high risk patients with hypertension.1 A network meta-analysis confirmed and extended these findings.2
On the basis of this evidence, the seventh report guidelines issued in the United States by the Joint National Committee on Prevention, Evaluation, and Treatment of High Blood Pressure recommend the use of low dose diuretics as first line pharmacological treatment for uncomplicated high blood pressure.3 In England and Wales, the National Institute for Health and Clinical Excellence guidelines recommend the use of low dose diuretics as a first choice therapy for high blood pressure in black patients or those aged 55 or above, and recommend a combination of diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers in patients under 55 years who do not respond to initial treatment.4
About half of all patients with hypertension require a second medication to achieve control of blood pressure. In ALLHAT at five years, for instance, 40.7% of patients randomly allocated to chlorthalidone were taking at least one other antihypertensive medication. Other major classes of antihypertensive medication—β blockers, calcium channel blockers, angiotensin converting enzyme inhibitors, and angiotensin receptor blockers—all lower blood pressure.1 2 5 6 However, the optimal second line agent for the prevention of cardiovascular disease among patients who are taking low dose diuretics and who require additional treatment for blood pressure control is not known. Although a National Heart, Lung, and Blood Institute working group recommended the conduct of a trial to evaluate the optimal second line treatment for hypertension,7 no such trial has been performed to date.
The purpose of this case-control study was to examine the association of myocardial infarction and stroke with several commonly used two drug treatments regimens: diuretics plus β blockers; diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers; and diuretics plus calcium channel blockers.
Methods
Study setting and participants
Participants were identified from patients enrolled in the Group Health Cooperative, a large health maintenance organisation located in western Washington state. Although Group Health provides hypertension treatment guidelines similar to those of the Joint National Committee on Prevention, Evaluation, and Treatment of High Blood Pressure, practising physicians are free to choose an antihypertensive treatment from any of the major drug classes, all of which are included in the formulary.
Ongoing studies on drug-gene interactions enabled us to both identify and follow Group Health patients with hypertension. This includes both patients who were identified for previous studies8 as well and new patients diagnosed with hypertension. Cases were identified from the Group Health hospitals’ computerised discharge abstracts, the bills for out of plan services provided by non-Group Health physicians and healthcare facilities, and the results of a computerised match between Group Health enrolment files and the Washington state death registry. Individuals between the age of 30 and 79 years with pharmacologically treated hypertension and a diagnosis of an incident fatal or non-fatal myocardial infarction between January 1989 and December 2005 or a fatal or non-fatal stroke between July 1989 and December 2005 were included in the study. Individuals with myocardial infarction or stroke events that were a complication of a medical procedure or surgery were not included. Cases’ diagnoses were validated by medical record reviews as described elsewhere.8
Controls were Group Health members who were pharmacologically treated for hypertension and met the same eligibility criteria as the cases but had not experienced either a myocardial infarction or stroke. Controls were frequency matched to myocardial infarction cases—the largest case group—by age (within a decade), sex, and calendar year of the cases’ diagnoses, at a ratio of between 2:1 and 3:1. The case-control ratio was based on power calculations conducted for a previous study of ours that addressed a similar question.8 Given the importance of investigating the risks and benefits of second line therapy,7 we decided to address the question in the setting of a case-control study without conducting additional power calculations.
Index date and eligibility
Each participant was assigned an index date. For cases admitted to hospital, the index date was defined as the admission date for the first myocardial infarction or stroke. For out of hospital fatal cases, the index date was the date of death. The index date for controls was a computer generated random date within the calendar year in which they were sampled. Cases and controls who were enrolled in the study for less than one year or who had had fewer than four visits to a Group Health clinic before their index date were excluded. We also excluded all cases and controls who had had either a myocardial infarction or stroke before their index date.
Data collection
Data collection comprised a review of the Group Health ambulatory medical record and a telephone interview of consenting survivors. Using the Group Health medical record, trained medical record abstractors determined eligibility and collected information about traditional risk factors for cardiovascular disease such as blood pressure, smoking, angina, diabetes, and cholesterol. Only information about the period before the index date was used. For patients consenting to telephone interview, we obtained additional information about risk factors such as smoking status, physical activity, education, and race. For individuals who did not complete the telephone interview, these data were obtained from the medical record review.
Data on drug treatment were extracted from the Group Health pharmacy database, which includes a record for each prescription dispensed by a Group Health pharmacy. Each pharmacy record includes the drug type and dose, quantity dispensed, and the dosing instructions. When dosing instructions were missing from the pharmacy data, dosing instructions were obtained from the medical records. To determine use of a particular drug at the index date, we searched the pharmacy data for the prescription immediately preceding that date. If the patient received a dose sufficient to last until the index date and assuming at least 80% compliance, that person was considered a user of the drug at the index date. To minimise potential confounding by newly started prescriptions for conditions that require drug treatment, a current user was defined as an individual who was a user at index date as well as at 30 and/or 60 days before the index date.
To minimise confounding by indication, we excluded participants with heart failure or evidence of coronary heart disease (defined as a history of coronary bypass surgery, angioplasty, previous myocardial infarction, or angina), diabetes, or chronic kidney disease (defined as creatinine level >2 mg/dl). Of the remaining participants, we included only those patients who were currently treated with one of the three common two drug combinations: diuretics plus β blockers; diuretics plus calcium channel blockers; and diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers.
Statistical analysis
Participants were classified according to their treatment as of the index date: (a) diuretics plus β blockers; (b) diuretics plus calcium channel blockers; and (c) diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers. Multiple logistic regression models were used to determine maximum likelihood estimates and their associated robust standard errors, which were then used to compare the risk of myocardial infarction and stroke among the three groups.9 Users of diuretics plus β blockers served as the reference group. Models were adjusted for the matched variables age (linear), sex, and index year (linear spline: 1989-1992; 1993-1996; 1997-2000; and 2001-2005), and for other possible confounders including smoking status (current v not) and total cholesterol levels (linear). We divided daily drug doses into low, medium, or high. The modal daily dose for each generic drug was classified as “medium,” whereas daily doses below that amount were classified as “low” and daily doses above that amount as “high.” Median values were used for subgroup analyses by age, serum glucose concentration, pretreatment systolic blood pressure, treated systolic blood pressure, and hypertension duration. Chained equations multiple imputation was used to account for missing data.10 The analyses were conducted using Intercooled Stata 8.2 (StataCorp LP; College Station, TX) and SAS 9.1.3 (SAS; Cary, NC). Odds ratio (OR) estimates were used to approximate the relative risk.
Results
We identified 1305 patients who used two drug antihypertensive treatment regimens: 211 patients who had a first myocardial infarction, 142 who had a first stroke, and 952 controls. Of these 1305 individuals, 629 were treated with diuretics plus β blockers, 273 with diuretics plus calcium channel blockers, and 403 with diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers. The exclusions to minimise the chance of confounding by indication resulted in a study population at relatively low risk of cardiovascular disease.
Among controls, those treated with diuretics plus calcium channel blockers had a longer history of hypertension, higher recent systolic blood pressure, and higher glucose levels than patients treated with diuretics plus β blockers (table 1⇓). Controls treated with diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers were younger and had been enrolled at Group Health for a shorter period than those treated with diuretics plus β blockers. Among cases, those treated with diuretics plus calcium channel blockers were younger, had been enrolled at Group Health for a shorter period of time, and had a higher BMI and a higher recent systolic blood pressure than cases treated with diuretics plus β blockers (table 1). Cases treated with diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers were younger than those treated with diuretics plus β blockers.
Characteristics of cases and controls receiving various two drug antihypertensive regimens that included a diuretic
Table 2⇓ compares the relative risks of myocardial infarction and stroke in patients receiving the three antihypertensive drug regimens. Compared with treatment with diuretics plus β blockers, treatment with diuretics plus calcium channel blockers was associated with an increased risk of myocardial infarction (OR 1.93, 95% confidence interval 1.34 to 2.77) and remained so after adjustment for age, sex, index year, smoking, and total cholesterol levels (OR 1.98, 95% CI 1.37 to 2.87). The two treatment regimens were associated with a similar risk of stroke (fully adjusted OR 1.02, 95% CI 0.63 to 1.64). An increase in the risk of myocardial infarction was also observed when diuretic therapy was limited to thiazides only (OR 2.08, 95% CI 1.41 to 3.09) and when we excluded patients with an index year before 1994 (that is, who were included in our previous publication about antihypertensive drug therapy; OR 1.95, 95% CI 1.24 to 3.08).7
Relative risk of myocardial infarction and stroke in patients receiving various two drug antihypertensive regimens that included a diuretic
Treatment with diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers might be associated with a lower risk of myocardial infarction and stroke than treatment with diuretics plus β blockers (myocardial infarction: OR 0.76, 95% CI 0.52 to 1.11; stroke: OR 0.71, 95% CI 0.46 to 1.10); however, these associations could well have been the result of chance (table 2). The difference in stroke risk between these two regimens was more pronounced when we limited our analysis to ischaemic strokes (OR 0.56, 95% CI 0.33 to 0.96). Additional adjustment for pretreatment systolic blood pressure, hypertension duration, most recent systolic blood pressure, or smoking (pack years) altered the relative risk estimates only minimally.
Table 3⇓ shows the results of an analysis of dose levels for the three treatment groups. Patients receiving diuretics plus low dose β blockers served as the reference group. Among patients receiving diuretics plus calcium channel blockers, the estimated risk of myocardial infarction increased as the dose of the calcium channel blockers increased (from OR 1.53, 95% CI 0.82 to 2.87 for low dose to OR 2.19, 95% CI 1.12 to 4.27 for high dose). In patients treated with angiotensin converting enzyme inhibitors or angiotensin receptor blockers, however, the estimated risk of myocardial infarction decreased as the dose of angiotensin converting enzyme inhibitors or angiotensin receptor blockers increased (from OR 1.56, 95% CI 0.77 to 3.16 for low dose to OR 0.61, 95% CI 0.34 to 1.10 for high dose). The tests for trend were not significant (table 3).
Relative risk of myocardial infarction and stroke in patients receiving different daily doses (low, medium, high) of two drug antihypertensive regimens that included a diuretic
We repeated our main analysis limited to the most common drugs in each class used at Group Health (table 4⇓). Compared with use of diuretics plus atenolol, the use of a diuretic with either of the two most commonly used calcium channel blockers was associated with an increase in the risk of myocardial infarction (OR 2.24, 95% CI 1.33 to 3.77 for verapamil and OR 2.38, 95% CI 1.16 to 4.89 for felodipine). The use of diuretics plus lisinopril may be associated with a decreased risk of stroke (OR 0.64, 95% CI 0.39 to 1.05) and with a decreased risk of myocardial infarction (OR 0.81, 95% CI 0.54 to 1.22), but the 95% confidence interval for both estimates included one.
Relative risk of myocardial infarction and stroke in patients receiving various two drug antihypertensive regimens that included a diuretic*†
The figures⇓ ⇓ ⇓ ⇓ present the relative risks of myocardial infarction and stroke in subgroups defined by age, sex, serum glucose concentration, pretreatment systolic blood pressure, treated systolic blood pressure, and hypertension duration. The relative risk of myocardial infarction associated with the use of diuretics plus calcium channel blockers compared with the use of diuretics plus β blockers was similar across categories with the exception of duration of hypertension, where the association was limited to those with shorter than median duration (P=0.01 for the test for interaction). Stroke risk was similar in users of diuretics plus calcium channel blockers and users of diuretics plus β blockers in all of the subgroups. The relative risks of myocardial infarction and stroke associated with the use of diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers was also similar across all subgroups. We would expect on average at least one false positive for these 24 statistical tests at the 0.05 level.
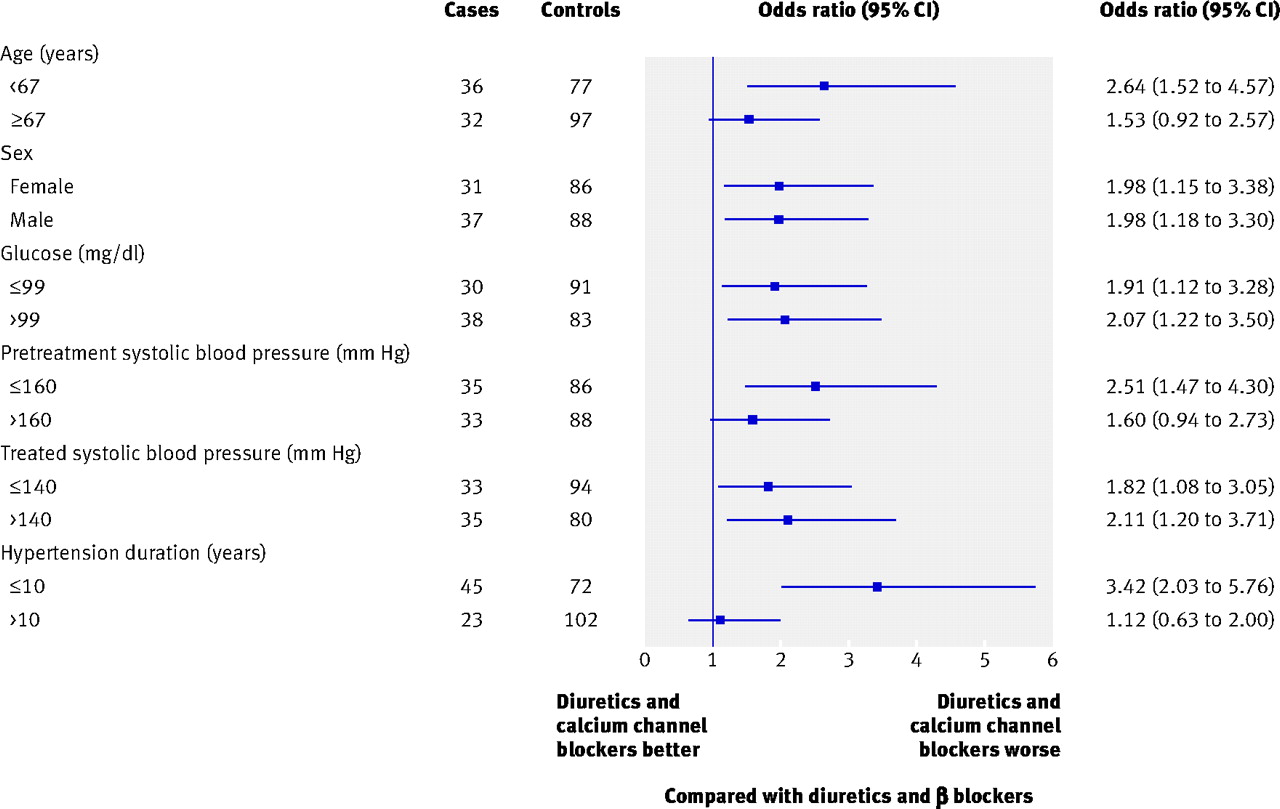
Fig 1 Relative risk of myocardial infarction in specified subgroups of patients on diuretics and calcium channel blockers, with diuretics plus β blockers as a reference. Odds ratios adjusted for age, sex, index year, smoking, and total cholesterol
{kind=link}

Fig 2 Relative risk of myocardial infarction in specified subgroups of patients on diuretics angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), with diuretics plus β blockers as a reference. Odds ratios adjusted for age, sex, index year, smoking, and total cholesterol
{kind=link}

Fig 3 Relative risk of stroke in specified subgroups of patients on diuretics and calcium channel blockers, with diuretics plus β blockers as a reference. Odds ratios adjusted for age, sex, index year, smoking, and total cholesterol
{kind=link}

Fig 4 Relative risk of stroke in specified subgroups of patients on diuretics and angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), with diuretics plus β blockers as a reference. Odds ratios adjusted for age, sex, index year, smoking, and total cholesterol
{kind=link}
Discussion
In this case-control study of relatively low risk patients, treatment with diuretics plus calcium channel blockers was associated with a higher risk of myocardial infarction than treatment with diuretics plus β blockers or diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers. This effect was consistent across subgroups defined by age, sex, serum glucose levels, pretreatment blood pressure, and most recent systolic blood pressure. Treatment with diuretics and angiotensin converting enzyme inhibitors or angiotensin receptor blockers was associated with a slightly lower risk of myocardial infarction and stroke than treatment with diuretics and β blockers, but these associations could have been the result of chance.
Strengths and limitations
The strengths of this study include the use of a population based setting, the completeness of case identification, the validation of case diagnosis, the ascertainment of a number of potential confounding factors, and the use of the Group Health pharmacy database to obtain comparable data on antihypertensive therapy in cases and controls. All participants were members of a health maintenance organisation and thus had similar access to health care. The similarities in the clinical characteristics of the three treatment groups minimised the likelihood of important confounding by such characteristics. We used exclusion to minimise confounding by specific drug therapies for conditions such as diabetes, heart failure, coronary heart disease, and chronic kidney disease.
This study was observational, however, and the patients were not assigned at random to the antihypertensive therapy options. Unknown or unmeasured confounding factors might have existed for which adjustment was not possible. The blood pressure measurements we used in this study were obtained as part of routine care and are subject to measurement error; however, any such error would most likely be non-differential and is unlikely affect our findings. Measurement error in the assessment or estimation of other covariates and their severity might have resulted in incomplete adjustment and residual confounding. There might also have been residual confounding by indication owing to the presence of other comorbid conditions, such as chronic obstructive pulmonary disease, that could reduce the likelihood of a patient being prescribed a β blocker. This confounding is unlikely to be significant in our study given that the proportion of subjects who smoked was similar in the three treatment groups (table 1) and that the adjustment for smoking did not change the relative risk estimates. The participants in our study were almost 90% white, so our conclusions might be limited in their application to other populations.
Comparison with other studies
When additional antihypertensive therapy is needed, a patient’s comorbidities may indicate the choice of second line treatment. Large long term clinical trials have identified important major health benefits associated with β blockers in patients who have coronary disease11 or heart failure,12 and major health benefits associated with angiotensin converting enzyme inhibitors in patients with coronary disease, heart failure,13 diabetes,14 and renal failure.15 However, no trials have evaluated the influence of diuretics accompanied by different possible second line agents in terms of the ability of each regimen to prevent myocardial infarction or stroke.
Several trials of first line treatments for hypertension have included active treatment comparison groups, but the trials have generally either compared “old” drugs with “new” drugs or compared one new drug with another new drug. Examples include the International Verapamil-Trandolapril Study (INVEST)16; the Losartan Intervention For Endpoint reduction in hypertension (LIFE) study17; the Captopril Prevention Project (CAPPP)18; the Swedish Trial in Old Patients with Hypertension-2 (STOP-2)19; the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA)20; and the Valsartan Antihypertensive Long-term Use Evaluation (VALUE) trial.21 Although some of these trials used diuretics as second line agents, they did not use low dose diuretics as a first line therapy and often used the β blocker atenolol as the first line agent.22
Few trials of combination therapy have used a diuretic as the first line antihypertensive agent in at least one arm of the trial. The Hypertension in the Very Elderly Trial (HYVET) used the diuretic indapamide with or without perindopril as a first line treatment in patients aged 80 years or older with hypertension, but the comparison group received placebo.23 In the recently published Avoiding Cardiovascular Events through Combination Therapy in Patients Living with Systolic Hypertension (ACCOMPLISH) trial, high risk patients with hypertension were randomly assigned to receive combination therapy with benazepril plus amlodipine or benazepril plus hydrochlorothiazide.24 The primary outcome was a composite of cardiovascular deaths and cardiovascular events (with the exception of non-fatal heart failure). Blood pressure control was similar in both groups. The trial was stopped early after about three years of follow-up because the benazepril-amlodipine arm was associated with a reduced risk of cardiovascular deaths and cardiovascular events (HR 0.80, 95% CI 0.72 to 0.90). The patients in our case-control study differed from those in the ACCOMPLISH trial in several respects. Amlodipine and benazepril were rarely used as antihypertensive therapies in our study population; neither was the two drug combination of calcium channel blockers plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers. In addition, the exclusions used to control for potential confounding by indication removed most high risk patients from our study, whereas the ACCOMPLISH trial included only high risk patients. In clinical trials of antihypertensive treatments, the strategy of selecting high risk patients who have several additional risk factors is often used to increase the event rate and the power of the trial. In observational studies of antihypertensive treatment, however, the strategy of excluding patients who have additional indications for specific drug treatments is the optimal approach to control for confounding by indication for those factors.
Possible mechanism
Our findings are consistent with the renin hypothesis, which suggests that patients’ blood pressure response to different antihypertensive drugs depends on their plasma renin levels.25
Patients in our case-control study generally received a two drug regimen only if their blood pressure was not controlled on single drug therapy, usually with a diuretic (a sodium and volume reducing drug). Patients with low renin hypertension would be expected to respond to a thiazide diuretic alone and would only infrequently require a second line drug; therefore, the pool of patients in our study receiving a two drug regimen would be enriched with those who have medium or high renin hypertension. According to the renin hypothesis, those patients receiving an additional anti-renin-system drug—such as an angiotensin converting enzyme inhibitor, an angiotensin receptor blocker, or a β blocker—would be expected to respond more favourably in terms of blood pressure control and reduction in risk of cardiovascular events than those receiving a different sodium and volume reducing drug—such as a calcium channel blocker. In contrast, in the ACCOMPLISH trial, where participants were randomly assigned to a two drug regimen, we would expect a mix of high, medium, and low renin hypertension. This difference in patient populations could be responsible for the different findings for calcium channel blockers in the two studies.
Several authors have opined that the achieved blood pressure rather than the type of treatment is the major determinant of the risk of cardiovascular complications in patients with hypertension.16 18 21 This perspective implies that the most important aim of future trials would be to evaluate the association between aggressive blood pressure control and future health outcomes.26 27 From a clinical pharmacology point of view, however, it is unlikely that the major antihypertensive drug classes, with their various different targets and mechanisms of action, all have the same effect on the risks of myocardial infarction, stroke, and heart failure. For instance, in ALLHAT, patients initially randomly assigned to doxazosin had a higher risk of heart failure than those randomised to the other three treatment strategies despite achieving a similar reduction in blood pressure, and the doxazosin arm was stopped early.28 The ACCOMPLISH trial provides additional evidence in this regard.23 Such data suggest the need to consider the use of more than one strategy of blood pressure lowering in ongoing studies such as the Systolic Blood Pressure Intervention Trial (SPRINT).29
Conclusions and implications
The goal of treating hypertension is to prevent complications associated with high blood pressure. In this case-control study of relatively low risk patients, the use of diuretics plus calcium channel blockers was associated with a higher risk of myocardial infarction than the use of diuretics plus β blockers or diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers. These findings support the National Institute for Health and Clinical Excellence guidelines, which do not recommend the use of diuretics plus calcium channel blockers. A large long term trial of second line treatments in patients who are already on a low dose diuretic—as recommended by the National Heart, Lung, and Blood Institute working group7—would be required to provide a solid basis for treatment recommendations.
What is already known on this topic
Current guidelines in the United States recommend the use of low dose diuretics as first line pharmacological treatment for all patients with uncomplicated hypertension
In England and Wales, guidelines recommend low dose diuretics for black patients or those age 55 or above
About half of patients with hypertension require a second medication to achieve control of blood pressure
What this study adds
In relatively low risk patients, the use of diuretics plus calcium channel blockers was associated with a higher risk of myocardial infarction than the use of diuretics plus β blockers or diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers
Treatment with diuretics and angiotensin converting enzyme inhibitors or angiotensin receptor blockers was associated with a slightly lower risk of myocardial infarction and stroke than treatment with diuretics and β blockers, but these associations could have been the result of chance.
Notes
Cite this as: BMJ 2010;340:c103
Footnotes
Contributors: IBM, SRH, and BMP are responsible for the conception and design of this study. IBM, SRH, NSW, BM, JACD, and BMP undertook the analysis and interpretation of the data. Drafting the article or revising it critically for important intellectual content was performed by IBM, SRH, NSW, BM, CDF, KLW, JACD, DSS, EBL, RNL, NLS, KMR, NLG, and BMP. IBM, SRH, NSW, BM, CDF, KLW, JACD, DSS, EBL, RNL, NLS, NLG, and BMP all gave final approval of the version to be published. IBM and BMP act as guarantors of the paper.
Funding: This research was supported in part by grants HL43201 (BMP), HL40628 (BMP), HL60739 (BMP), HL68639 (BMP), HL68986 (SRH), HL73410 (NLS), HL74745 (BMP), HL085251 (BMP), and HL007902 (DSS) from the National Heart, Lung, and Blood Institute. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Heart, Lung, and Blood Institute or the National Institutes of Health.
Competing interests: All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare (1) No financial support for the submitted work from anyone other than their employer; (2) No financial relationships with commercial entities that might have an interest in the submitted work; (3) No spouses, partners, or children with relationships with commercial entities that might have an interest in the submitted work; (4) No non-financial interests that may be relevant to the submitted work.
Ethical approval: All participants provided written informed consent approved by the Cooperative Human Subjects Review Committee at Group Health.
Data sharing: No additional data available.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.