Article Text

Abstract
Objective To examine how the intensity and duration of tobacco control advertising relate to adolescent smoking prevalence.
Methods Australian students (aged 12–17 years) participating in a national survey conducted triennially between 1993 and 2008 (sample size range 12 314–16 611). The outcome measure was students’ smoking in the previous 4 weeks collected through anonymous, self-completed surveys. For each student, monthly targeted rating points (TRPs, a measure of television advertising exposure) for tobacco control advertising was calculated for the 3 and 12 months prior to surveying. For each time period, cumulative TRPs exposure and exposure to three intensity levels (≥100 TRPs/month; ≥400 TRPs/month; ≥800 TRPs/month) over increasing durations (eg, 1 month, 2 months, etc) were calculated. Logistic regression examined associations between TRPs and adolescent smoking after controlling for demographic and policy variables.
Results Past 3-month cumulative TRPs were found to have an inverse relationship with smoking prevalence. Low TRPs exposure in the past 12 months was positively associated with adolescent smoking prevalence. However, smoking prevalence reduced with cumulative exposure levels above 5800 cumulative TRPs. Additionally, exposure to ≥400 TRPs/month and ≥800 TRPs/month were associated with reduced likelihood of smoking, although the duration needed for this effect differed for the two intensity levels. When intensity was ≥400 TRPs/month, the odds of smoking only reduced with continuous exposure. When intensity was ≥800 TRPs/month, exposure at levels less than monthly was associated with reductions in smoking prevalence.
Conclusions Both antismoking advertising intensity and duration are important for ensuring reductions in adolescent smoking prevalence.
Statistics from Altmetric.com
Mass media antismoking advertising campaigns are a key component of comprehensive tobacco control programmes.1 ,2 Multiple studies have shown that mass media antismoking campaigns can reduce smoking prevalence among adolescents.3–6 However, while a considerable body of research has examined the characteristics of advertisements most effective with adolescents,5 ,7 information regarding the optimal level of advertising (intensity and duration of campaigns) needed to reduce adolescent smoking prevalence is limited.6
Three studies have examined the relationship between adolescent smoking prevalence and antismoking advertising exposure using the objective measures of advertising reach targeted rating points (TRPs) or gross rating points (GRPs).8–10 TRPs and GRPs are an advertising industry measure of the number of people in a target audience potentially exposed to advertising over a specific time period. These studies suggest that cumulative antismoking advertising exposure is inversely associated with adolescent smoking prevalence, although results differ regarding the exposure levels needed for this effect. One study found that exposure to at least one state funded antismoking advertisement in the previous 4 months (100 TRPs/4 months) reduced the likelihood of adolescent smoking.10 Another found an inverse linear relationship between advertising exposure over a 4-month period and smoking prevalence.9 The third study8 examined the effects of exposure to a specific adolescent focused antismoking advertising campaign (the ‘truth’ campaign) over the campaign's first 3, 12 and 24 months. This study found that while there was no association between advertising and smoking prevalence for the first 3 months of the campaign, there was an inverse association between smoking and cumulative advertising exposure over 12 and 24 months. However, cumulative advertising levels above 10 000 TRPs over a 24-month period did not produce further decreases in smoking prevalence, leading the authors to conclude that cumulative exposure up to 10 000 TRPs over 24 months is optimal for reducing adolescent smoking.
A common practice among mass media campaign planners is to run advertising campaigns for a limited period, followed by periods of very low intensity or no advertising. Currently there is no information regarding whether this ‘pulsing’ advertising strategy aids or detracts from the effectiveness of advertising. Work with adult smokers is beginning to investigate the impact of advertising duration on quitting behaviours with a recent study finding increased quit attempts after 6 weeks of continual exposure to antismoking advertising.11
To date, studies conducted in the area of adolescent smoking have examined cumulative levels of advertising exposure over specific time periods with results then used to estimate an average monthly level of exposure. However, no study has specifically examined the optimal monthly exposure levels. The US Centers for Disease Control and Prevention (CDC) recommend that antismoking advertising be aired at a minimum average of 1200 TRPs per quarter for the introduction of a campaign followed by an average of 800 TRPs per quarter.2 These recommendations equate to an average of 400 TRPs/month during a campaign's introduction followed by 267 TRPs/month. As evidence regarding the exposure levels needed to reduce smoking among adolescents is inconsistent, the current study examines how duration of exposure to three minimum advertising intensity levels: (1) ≥100 TRPs/month; (2) ≥400 TRPs/month; and (3) ≥800 TRPs/month influences adolescent smoking. The threshold point of ≥100 TRPs was chosen to represent a minimum level of advertising exposure. The second minimum intensity threshold point of ≥400 TRPs/month reflects the minimum monthly average of the CDC's recommended level of advertising for the introduction of a campaign.2 This threshold point is also the average level of advertising Farrelly et al8 found reduced the odds of smoking by 22% over a 2-year campaign period. Farrelly et al8 found that exposure to 10 000 TRPs over approximately the first 12-month period of the campaign, reduced the likelihood of an adolescent smoking by 44%. This annual exposure level averages to 800 TRPs/month and this monthly level was used as the third minimum intensity threshold level (≥800 TRPs/month). The differing findings from previous research may suggest that the minimum intensity level needed to produce a decrease in adolescent smoking depends on the exposure times. To examine this, the impact of the different advertising intensities was examined for two exposure times: past 3 months and past 12 months.
This is the first study outside the USA to explore the effects of advertising intensity using TRPs on adolescent smoking prevalence. Mass media campaigns in Australia have generally taken a health consequences approach and since 1998 most advertisements have used graphic images or personal emotional stories to illustrate the serious health effects of smoking. While advertisements have generally targeted adult smokers, they have high recall among youth12 and research has consistently shown that these advertisements appeal to adolescents and can reduce youth smoking intentions.6 ,13
Methods
Study population
Data are from students of five Australian states participating in national cross-sectional surveys involving representative samples of secondary school students conducted triennially between 1993 and 2008.14 In all study years, a stratified two-stage probability sample was used, with schools selected at the first stage and students at the second. In each state, schools were selected from the three main education sectors (government, Catholic, independent) to ensure proportional representation. The number of students surveyed from each state was proportional to the population size of that state. Students completed surveys anonymously between May and December with surveys administered on school premises by external research staff. All surveys were approved by the Cancer Council Victoria's Human Research Ethics Committee.
As advertising exposure data were only available for capital city metropolitan areas in each state, only data from students residing in these areas were used in analyses. Institutional ethics approval was obtained.
Survey data
Questionnaire items were identical in all surveys. Students reported their sex, current age and postcode of where they resided. The date of the survey was added to each student’s survey by survey administrators after completion. Past month smoking, assessed through the question ‘have you smoked in the past four weeks?’ (response: yes or no), was the outcome variable.
Teenage tobacco control TRPs
The advertising exposure measure was antismoking adolescent (13–17-year olds) TRPs. TRPs data obtained from the media monitoring company responsible for determining television ratings in all Australian states and territories were used to measure advertising exposure. TRPs are an indicator of the percentage of a target audience potentially exposed to the advertisement and the number of times exposed. Therefore, 100 TRPs is equivalent to one potential advertisement exposure per month for all adolescents within a media market. Adolescent TRPs are derived from television programmes watched by this age group, which include both youth-specific and general audience programmes.
Australia's media market is divided into five metropolitan areas covering the regions associated with five major mainland cities (Adelaide, Brisbane, Melbourne, Perth, Sydney) and six regional areas. Advertising exposure data for the entire period of the study was only available for the five metropolitan advertising areas representing a potential audience reach of around two-thirds of Australia's population. Students' postcode data was used to determine whether a student resided in the five metropolitan advertising areas and only data from those students living in these areas were used in analyses.
Two advertising exposure variables were calculated. First, the total cumulative TRPs exposure was determined for each student for both the 3- and 12-month period prior to their survey date. For students surveyed after the 16th of the month, the current month's TRPs were included in these sums. For students surveyed on or before the 16th of the month, cumulative totals were calculated starting from the previous month. Second, durations of TRPs exposure were calculated for the three intensity levels: ≥100 TRPs; ≥400 TRPs; and ≥800 TRPs over the past 3 and 12 months. For each of the previous 12 months, three binary variables were created to indicate if the student's TRPs exposure was ≥100 TRPs; ≥400 TRPs; and ≥800 TRPs for that month. Using these variables, a duration variable was then created to indicate how many months each student was exposed to antismoking advertising at these three minimum intensity levels. The duration variable includes no exposure (0 months) at these minimum intensity levels.
Control variables
Tobacco control policies
As our previous work found that youth access, point-of-sale advertising/outdoor advertising and clean indoor air policies were associated with changes in adolescent smoking prevalence between 1990 and 2005,15 our current analyses control for these policy changes. The coding scheme to describe the strength of each policy in each state is described elsewhere.15 In brief, a number of target provisions in each policy area were identified to reflect key tobacco control objectives. For clean indoor air policies, the degree of implementation of each provision was assessed using a scale of 0 ‘absent’, 1 ‘partially implemented’ and 2 ‘fully implemented’. For the other two policies, the scale extended to 3 to reflect the level of policy implementation. Within each policy area, scores for each provision were tallied and expressed as a percentage of the maximum score possible.
Cigarette price
State-specific data on recommended retail cigarette prices were obtained from the retail trade magazine Australian Retail Tobacconist for the period January 1993 to December 2008. Cigarette prices were extracted for the one or two brands and pack-sizes most commonly smoked by adolescents in those states. Prices were adjusted to December 2008 values using the consumer price index. We use change in cigarette price in the 12 months prior to the student being surveyed as our control variable.15
Adult smoking prevalence
As indicated, antismoking advertising campaigns in Australia have generally been directed at adult smokers rather than adolescents. As the level of adult smoking in a state may have influenced that state's level of antismoking advertising, we controlled for state adult smoking prevalence in analyses. Adult smoking prevalence is available for the year prior to the adolescent survey from national studies designed to determine adult smoking prevalence.16 ,17
Student level controls
In addition, gender, age and education sector were controlled in analyses. In Australia, Catholic and independent schools charge school fees, with elite independent and Catholic schools commonly located in higher socioeconomic areas and commonly attended by children from higher socioeconomic families. For this reason, there is considerable confounding between education sector and socioeconomic measures and after controlling for education sector, adolescent smoking was not associated with socioeconomic status. Therefore, socioeconomic status was not included in the statistical models.
Statistical analysis
A two-step approach was taken for analyses. First, analyses were conducted to examine whether higher cumulative TRPs over the past 3 and 12 months were associated with reduced adolescent smoking. In these analyses, cumulative TRPs were scaled such that the estimated ORs give the change in likelihood of smoking given a change of 400 TRPs/month. Diminishing returns at higher TRPs exposure was tested for by including a quadratic term for cumulative TRPs (TRPs squared). Where there was a significant association between cumulative TRPs exposure and smoking prevalence, we used the results from the logistic regression analyses to plot this relationship using the average (or median for skewed variables) values for all significant variables in the logistic regression model.
We then examined whether the duration of advertising at the three minimum intensity levels was associated with reduced smoking prevalence. As the duration variables were calculated from cumulative TRPs exposure the two variables were highly correlated. For this reason, separate logistic regression analyses assessed the effects of cumulative TRPs and each of the duration indicators on an adolescent smoking in the past month. Duration was used as a categorical variable with 0 months exposure to the minimal level of advertising, the reference category. Where possible we used each month in the duration period as a separate category. However, for ≥400 TRPs/month and ≥800 TRPs/month over a 12-month period, this was not possible due to small numbers of students exposed to this level of advertising for some duration periods (generally less than 300 cases). In these situations, we have combined the data for several months to achieve a total of at least 2000 cases exposed to the duration of advertising.
All analyses adjusted for policy variables, cigarette price change, adult smoking levels, student level variables and a categorical indicator of survey year. Analyses adjusted for the clustering of students at the school level with the Huber–White sandwich method used to calculate robust SEs. All analyses were conducted using Stata V.12.1.
Results
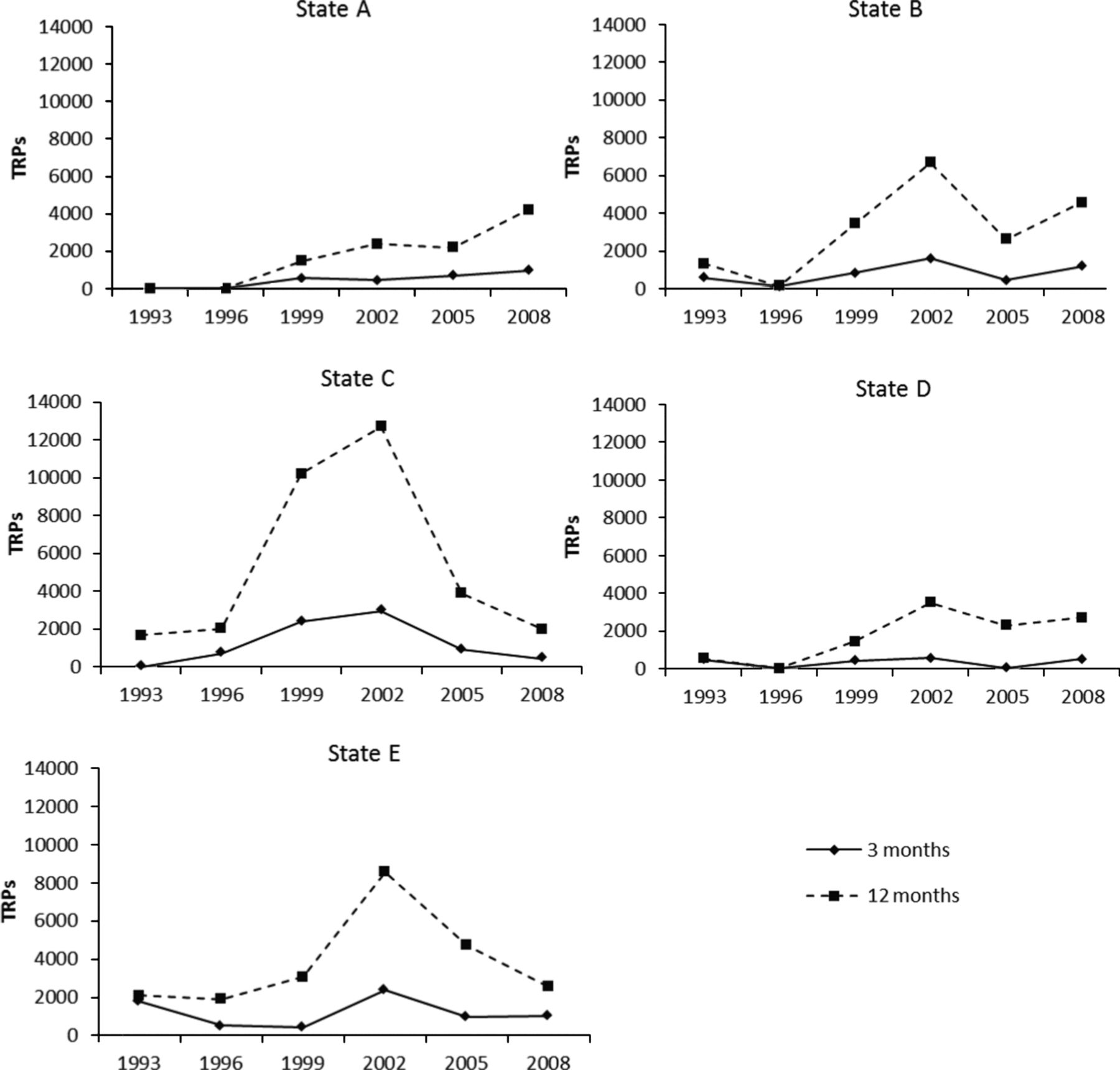
The prevalence of student smoking varied between states and by survey year with prevalence decreasing in all five states after 1996 (table 1). The extent of implementation of the three tobacco control policies increased over time. By 2008, 100% of the clean indoor air target policies, 80% of the youth access target policies and nearly 90% of the tobacco advertising target policies had been implemented (table 1). In 1993 and 1996, students in two states were exposed to minimal levels of tobacco control advertising in the 3- and 12-month period prior to being surveyed (figure 1). From 1999 onwards, students in all states were exposed to some level of tobacco control advertising in the two time periods.
Sample characteristics of Australian students participating in each survey and tobacco control activity in Australia during each survey year

Average 3 and 12 months cumulative adolescent tobacco control targeted rating points exposure for different Australian states and survey years between 1993 and 2008.
Association between TRPs and youth smoking prevalence
Three months cumulative advertising TRPs was inversely associated with adolescent smoking prevalence (OR=0.93, 95% CI 0.88 to 0.98). There was no evidence of diminishing returns with higher TRPs exposure. Although a similar inverse association was found for 12 months cumulative TRPs, when only this variable was including in the analysis, the association was not statistically significant (OR=0.95, 95% CI 0.89 to 1.02). However, when the quadratic term for cumulative TRPs was included in the model, both terms were significant (cumulative TRPs: OR=1.31, 95% CI 1.06 to 1.69; TRPs squared: OR=0.88, 95% CI 0.81 to 0.95). The ORs for these two terms do not suggest diminishing returns at higher TRPs but instead suggest that very low levels of TRPs over a 12-month period are associated with higher smoking prevalence estimates and that smoking prevalence only reduces after TRPs cumulative exposure reaches a critical point (figure 2). We estimate that this critical point is approximately 5800 cumulative TRPs in the previous 12 months. Figure 2 suggests that for the 12-month period, higher TRPs exposure is associated with reduced smoking.

{kind=link}
{kind=link}
Association between smoking prevalence and targeted rating points (TRPs) as found in logistic regression analyses predicting smoking prevalence from cumulative 12-month TRPs and squared cumulative 12-month TRPs (adjusting for significant covariates).
Examining how delivery strategies might affect the influence of TRPs, the association between duration of exposure to ≥100 TRPs, ≥400 TRPs or ≥800 TRPs/month and adolescent smoking is shown in table 2 (3-month period) and table 3 (12-month period). The effect of advertising duration varied across the three tested minimum intensity levels. For the 3-month period (table 2), there was no association between duration of antitobacco advertising at ≥100 TRPs/month and adolescent smoking. At ≥400 TRPs/month, advertising at this level had to be continual to reduce adolescent smoking. If a student was exposed to ≥400 TRPs in each of the three previous months, the odds of them smoking was reduced by about 15% (OR=0.85, 95% CI 0.76 to 0.94). High intensity advertising (≥800 TRPs/month) for two or three of the previous 3 months was associated with reduced likelihood of smoking.
Association between tobacco control advertising at ≥100 targeted rating points (TRPs)/month, ≥400 TRPs/month and ≥800 TRPs/month at different durations over the past 3 months and adolescent smoking (Australia 1993–2008)
Association between tobacco control advertising at ≥100 targeted rating points (TRPs)/month, ≥400 TRPs/month and ≥800 TRPs/month at different durations over the past 12 months and adolescent smoking (Australia 1993–2008)
For the 12-month period (table 3), there was either no association or a positive association with any duration of advertising at a level of ≥100 TRPs/month. This association reflects the increase in smoking found for low cumulative TRPs seen in figure 2. For moderate levels of advertising (≥400 TRPs/month), only advertising at this level continually over the 12-month period was associated with reduced odds of smoking. No student was potentially exposed to antismoking advertising at ≥800 TRPs/month for 5 months or for 11–12 months. Exposure to ≥800 TRPs/month for 8–10 months in the previous 12 months was associated with a reduced likelihood of smoking.
Discussion
Similar to other studies8–10 we found an inverse association between cumulative antismoking advertising and adolescent smoking prevalence. However, unlike these other studies, we also attempted to provide information for programme planners regarding how much advertising is needed per month and for how long the advertising needs to be on air in order to reduce smoking among adolescents. After adjusting for the implementation of key tobacco control policies, adult smoking prevalence and year of survey, two minimum levels of advertising exposure were inversely related to adolescent smoking: ≥400 TRPs/month (four advertisements/month) and ≥800 TRPs/month (eight advertisements/month). Importantly, our findings suggest that the effect of these different minimum levels of advertising depends on their duration. If advertising campaigns are run at a minimum level of ≥400 TRPs/month, they need to be maintained every month to reduce the likelihood of adolescent smoking. However, if the advertising minimum intensity is doubled to ≥800 TRPs/month, advertising duration could be reduced, with reductions in adolescent smoking prevalence achieved when this level of advertising was reached on average every second month. As these patterns of associations are found over both time periods, our data suggest that an advertising pulsing strategy might only be effective at reducing adolescent smoking prevalence if the minimum intensity of the advertising during the months it is on air is high.
The inverse linear relationship we found between 3 months cumulative TRPs and smoking prevalence is similar to previous research.9 However, for cumulative 12 months TRPs the pattern differs in that it suggested low levels of TRPs are associated with an increased likelihood of an adolescent smoking. Indeed, the pattern of results presented in figure 2 suggest that advertising levels of at least 5800 cumulative TRPs over a 12-month period are needed to achieve reductions in adolescent smoking prevalence. The positive association between adolescent smoking and low TRPs seen in figure 2 reflects the positive association we found between advertising at ≥100/TRPs a month and smoking prevalence. This finding is in contrast to previous work suggesting that exposure to at least one antitobacco advertisement over a 4-month period reduced the likelihood of smoking among US adolescents.10 The difference in findings may be attributable to the longer period of advertising used in our study (16 years compared with 2 years) which included several years (1993 and 1996) when there were extremely low levels of tobacco control advertising in all Australian states. This period has been recognised as a time of reduced tobacco control activity including reduced funding to tobacco control programmes that limited the broadcast of mass media campaigns. Adolescent smoking prevalence in Australia increased during the early 1990s. The positive association between low levels of advertising and adolescent smoking found in our study reflects the pattern of data from these years. Our findings suggest that in the absence of well-funded tobacco control programmes and at least moderate levels of antitobacco advertising, pro-smoking factors (eg, smoking among friends and parents, images of smoking in popular culture) may reassert their influence and drive smoking prevalence up.
As previous studies in this area have not examined the duration of different levels of antismoking advertising on adolescent smoking, it is not possible to directly compare our findings with others. We found that advertising at a minimum intensity of ≥400 TRPs/month was only effective if this level of advertising was maintained continuously over a 12-month period. A recent review has suggested that tobacco control advertising needs to be aired consistently at a level of 1200 TRPs/quarter.18 Our data suggest that to be effective with adolescents over the longer period, advertising at 400 TRPs/month needs to be consistent, that is month after month. Farrelly et al8 found that cumulative advertising levels up to 10 000 TRPs over a 2-year period was most effective for reducing adolescent smoking. Again, this level of advertising equates to an average of 400 TRPs/month.
We also found that advertising at a minimum intensity of ≥800 TRPs/month on average every 2 months over a 12-month period, was associated with reduced smoking prevalence. Farrelly et al8 found that potential exposure to cumulative 10 000 TRPs after approximately 12 months of ‘truth’ (equating to an average of 833 TRPs/month) was associated with an approximate 34% reduction in the likelihood of smoking. We found that the likelihood of an adolescent exposed to 8–10 months of advertising at ≥800 TRPs/month smoking in the past month was reduced by about 33%.
Of the three previous studies in this area, only one8 assessed youth directed advertising. Our study's findings may reflect the predominantly adult-oriented campaigns used in Australia. These emphasise the serious health consequences of smoking in an emotive fashion to increase quitting motivations, an approach now being used in a new national mass media campaign in the USA: ‘Tips from Former Smokers (TIPs)’.19 Our results may have been different if we examined youth directed campaigns, but research has shown that emotive adult-focused advertisements are noticed by adolescents and are perceived by adolescents to be effective in changing their behaviour.13 ,20–22 Our findings suggest that, with continued funding, the TIPs campaign might also influence youth smoking.
Several study limitations need to be noted. Our survey data were cross-sectional rather than longitudinal, so we cannot resolutely conclude that higher advertising levels reduced smoking among adolescents. While our use of objective measures of potential antismoking advertising exposure is a study strength, we do not know the precise ‘dose’ of advertising an individual adolescent received. However, TRPs do correlate with recall of antitobacco campaigns.23 ,24 A further strength is that we controlled for the extent of implementation of several tobacco control policies at the time of each survey, but it is possible that some other unmeasured factor influenced smoking behaviours. Including year in our analyses attempted to control for this possibility. Over the period of the study, most antismoking advertising campaigns in Australia occurred at a state level with state-based organisations deciding when to run advertising campaigns and the exposure level at which they are run. The decision to run advertising campaigns is based on a multitude of factors including funding, introduction of new policies, specific events or days (eg, World No Tobacco Day and New Year's Day) and programme strategy. There is a high correlation between state and advertising levels that precluded both variables being in the same regression analysis. As we were interested in examining the role of antismoking advertising levels on adolescent smoking we excluded state from our analyses. Our inclusion of state-based policy variables and state adult smoking prevalence aims to compensate in part for this exclusion. However, we acknowledge that by excluding state from the models we may have overestimated the effect of advertising on adolescent smoking. In addition, we did not adjust for the presence of school based prevention programmes or school based antitobacco policies that may have influenced adolescent tobacco use. If the delivery of these programmes increased when advertising levels were higher or if their effectiveness increased when there were higher levels of antismoking advertising, our results may have overestimated the effect of antismoking advertising.
Despite these limitations, we believe our study suggests that antismoking advertising campaigns make a significant independent contribution to reducing adolescent smoking prevalence. Importantly, our study suggests that the intensity and duration of antismoking advertising campaigns drive their effectiveness. If antismoking advertising is broadcast at high intensity (≥800 TRPs/month), a pulsing strategy may be effective at reducing adolescent smoking. If only a moderate intensity of advertising is broadcast, advertising needs to be continuous if it is to reduce adolescent smoking prevalence.
What this paper adds
-
Mass media tobacco control campaigns can influence adolescents’ smoking behaviours and have been associated with reduced smoking prevalence among adolescents. Currently there is little information regarding the optimal intensity and duration of advertising campaigns to ensure their effectiveness of adolescent smoking.
-
This paper shows that over the longer term, advertising at a moderate intensity (at least four advertisements a month) can be effective in reducing adolescent smoking prevalence, but only if maintained on a monthly basis. Advertising at a high intensity (at least eight advertisements a month) also reduced adolescent smoking prevalence, and was effective even if this level was not maintained every month.
Acknowledgments
We acknowledge the work of Professor David Hill in establishing the conduct of the triennial national secondary students’ survey. Professor Melanie Wakefield was supported by an Australian National Health and Medical Research Council research fellowship. Ms Kate Purcell developed and sourced data required for the policy implementation variables used in the analyses. Mr Charles Warne prepared the data for analysis and conducted preliminary data analysis for this paper.
References
Footnotes
-
Contributors VMW is lead researcher for the national secondary students’ survey, led manuscript writing, and contributed to study design, analysis plan and interpretation of results. SJD assisted with manuscript writing, contributed to study design, devised analysis plan and assisted with interpretation of results. KC assisted in data management, conducted data analyses and assisted with interpretation of results. MAW conceived study and contributed to analysis plan and interpretation of results. All authors contributed to drafts of the paper and approved the final version of the paper.
-
Funding This study was supported by an Australian National Health and Medical Research Council (Project Grant number 504707). Funding for student survey data collection was made available from the following organisations: The Cancer Council Victoria, The Cancer Council South Australia, The Cancer Council Tasmania, The Cancer Council NSW, The Cancer Council Northern Territory, The Cancer Council Queensland, The Cancer Council ACT, Department of Health Victoria, The NSW Health Department, The Department of Health Western Australia, Northern Territory Government Department of Health and Community Services, Queensland Education Department, Queensland Health, ACT Health, Drug and Alcohol Services Council SA, Health Department of Tasmania, and the Australian Government Department of Health and Ageing.
-
Competing interests None.
-
Ethics approval Cancer Council Victoria.
-
Provenance and peer review Not commissioned; externally peer reviewed.