Article Text

Abstract
The reliability of measurement of body temperature using a new infrared skin thermometer was evaluated in 107 newborns. The use of the device was associated with low operator-related variability and acceptable limits of agreement with the temperature measured with a rectal mercury thermometer. Use of the infrared skin thermometer is a comfortable and reliable way of measurement of body temperature in newborns.
Statistics from Altmetric.com
The use of mercury thermometer has long been the commonest method for measurement of body temperature. However, the restriction of mercury has led to the development of other devices. Recently, a skin thermometer that uses infrared technology has been developed. The aim of this study was to validate, in neonatology, the accuracy and the effectiveness of this non-invasive, easy-to-use and fast-to-read thermometer.
MATERIALS AND METHODS
The study included a convenience sample of term and preterm infants admitted to the newborn nursery or neonatal intensive care unit between May and October 2006 at the Dipartimento di Scienze Ginecologiche, Perinatologia e Puericultura, La Sapienza University of Rome. We obtained written informed consent for participation from the parents.
For measurement of the rectal temperature, a mercury-in-glass thermometer was introduced into the rectum to a depth of 2–3 cm from the anal margin. The temperature was read 3 min after insertion. Immediately after the measurement of the rectal temperature, the same operator (FC) recorded the skin temperature on the central part of forehead by using the infrared skin thermometer (No Touch Sensor Diagnostic, Chicco, Italy). The probe of the thermometer was positioned 0.5 cm from the skin, and the temperature was read after 9 s on the display screen of the thermometer. The skin temperature was recorded three times. In a subgroup of 86 infants, the digital skin temperature was measured alternately by two operators (FC and AM), and each time the temperature was recorded thrice.
Statistical analysis
Data are expressed as mean (SD) or mean and 95% confidence intervals as indicated. Paired data Student t test was used for between-group comparisons. We calculated the difference between the rectal and infrared skin temperature recordings. The limits of agreement between the mercury and digital measurements and those between the digital measurements taken by the two operators were calculated according to Bland and Altman as the mean (2 SD) of the differences between the two measurements.1 Limits of agreement were also calculated between the rectal mercury temperature and the digital temperature recorded by the first operator (FC), which followed measurement of the former. Statistical significance was accepted at p<0.05.
RESULTS
The study included 107 newborns with a birth weight of 1927 (851) g and a gestational age of 32.7 (4.4) weeks, (range 25–41 weeks), at a postnatal age of 15.7 (17.3) days (range 1–93 days). The rectal temperatures ranged from 35.1°C to 38.4°C; the mean of the three infrared skin temperature readings ranged from 35.3°C to 38.4°C. The correlation between the measurements with the two devices and the correlation between the measurements made by the two operators with the same device were, as expected, statistically significant (p<0.001).
The mean temperature measured with the rectal mercury thermometer and infrared skin device was 36.62 (0.66) and 36.66 (0.66), respectively (p = 0.18). The mean of the difference between the rectal temperature and the mean digital temperature measured by the two operators was −0.038°C (0.288°C) (95% CI −0.093°C to 0.017°C; range −0.75°C to 0.72°C). The limits of agreement ranged from −0.614 to 0.538 (fig 1). The mean difference between the rectal temperature and the first digital temperature reading taken immediately after the rectal temperature measurement was also quite similar (−0.052°C (0.315°C), 95% CI −0.112 to 0.008°C), as were the limits of agreement (−0.682 to 0.578).
{kind=link}
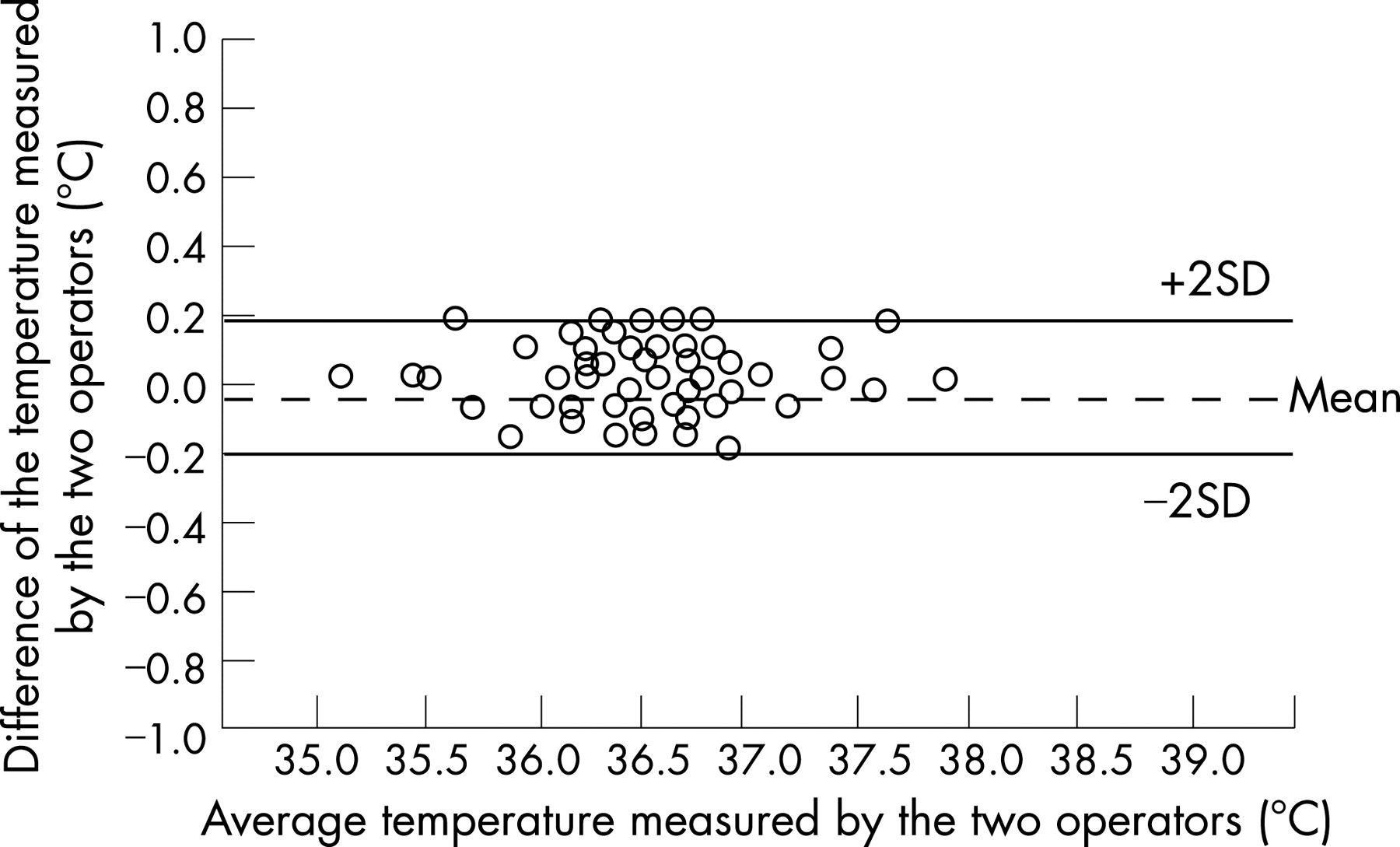
We did not find any significant differences between the means of the three infrared skin temperature recordings made by the two operators (n = 86; operator 1: 36.63°C (0.45°C) and operator 2: 36.62°C (0.44°C); p = 0.16). The mean difference between the means of the temperatures taken by the two operators was −0.017°C (0.111°C) (95% CI −0.007°C to 0.041°C; range −0.27°C to 0.27°C). The limits of agreement of the difference between the infrared skin temperature recorded by operator 1 and operator 2 were as follows: first measurement: −0.249 to 0.251; second measurement: −0.267 to 0.269; third measurement −0.273 to 0.279. The limits of agreement between the three temperature recordings made by each operator ranged from −0.20 and 0.20 or even narrower.
None of the newborns in this study were found to be hypothermic (ie body temperature <35.0°C) and hyperpyrexia (ie body temperature >38.0°C) was present in only 3/107 cases (detected with both the mercury and the infrared thermometers). The body temperature measured with the digital thermometer was in concordance with that measured by the rectal thermometer in 7/7 cases for temperatures <35.5°C, in 9/14 (64%) cases for temperatures <36.0°C and in 13/20 (65%) cases for temperatures ⩽36°C. The infrared skin thermometer measured body temperature >37.5°C in 8/8 cases (100% concordance) as with the mercury thermometer, >37°C in 18/23 cases (86% concordance) and ⩾37.0°C in 23/31 cases (74% concordance). The infrared skin thermometer confirmed the body temperature recordings made with the rectal thermometer between 36.0°C and 37.0°C (n = 72 infants) in 82% of the cases.
DISCUSSION
Although the gold standard method for measuring core temperature in humans is considered to be the pulmonary artery or bladder temperature, clinically, rectal temperature is the standard method of measuring temperature. Temperature measurement has to be reliable, precise and reproducible. Mayfeld et al have shown that in both term and preterm infants, rectal temperature correlates well with core temperature measured 5 cm beyond the anus with an electronic telethermometer.2
The inconvenience of rectal temperature measurement is related to the long time required for equilibration: substantial changes in the measured temperature occur up to 3 min. This long time can interfere with neonatal procedures in neonatal intensive care units, especially during neonatal transport. In addition, there is a danger of haemorrhage and perforation of the rectum when using a glass thermometer for rectal temperature measurement, particularly if the infant is struggling. Also, rectal temperature measurement is contraindicated if there is a bowel disease, especially necrotising enterocolitis.
In the past 15 years, infrared thermometers that measure the temperature at the external ear canal have become widely popular in clinical paediatrics. The infrared detector senses electromagnetic radiation emissions from tissue within the view of the probe. A microprocessor calculates the temperature value of the observed structures. In the USA, 65% of paediatricians and 65% of family physicians (general practitioners) use this method.3 A meta-analysis of 4441 children showed that the pooled mean temperature difference (rectal minus ear) was 0.29°C (95% limits of agreement −0.74 to 1.32).4 Although the pooled mean difference was small the limits of agreement remained wide, and the authors found that if the temperature measured at the rectum was 38°C, temperature at the ear could range anywhere between 37.04°C and 39.20°C. This low level of agreement between the two methods was attributed to inaccuracies in measurement at both sites, and the meta-analysis seemed to indicate that measurements taken with infrared ear thermometry cannot be used as an approximation of rectal temperature.
There are few published data on this issue with regard to the neonatal period, especially in premature infants in whom control of body temperature is very important. The novel aspects of the present study are: (i) the target population, which comprised term and preterm newborns aged less than 3 months; and (ii) the evaluation of the validity of a method of measuring skin temperature. Previous studies have mostly used ear thermometers.
After taking a few measurements (as is recommended, based on the characteristics of use of the infrared skin thermometer), the limits of agreement between the measurements taken with the two devices were such that if the skin temperature was 36.5°C, the rectal temperature would range between 35.9 and 37.0°C. Moreover, the measurements with the two devices were highly concordant even in conditions possibly relevant in clinical practice, such as for body temperatures <35.5°C or >37.5°C. In our study, none of the infants was hypothermic (<35.90°C) and only a few (n = 3) were pyrexial (>38.0°C) Thus we cannot draw conclusions about the concordance of the two devices in these conditions.
It should be noted, however, that in the present study the digital measurement of skin temperature was taken on the centre of the forehead, and, accordingly, we did not expect to observe a high rate of concordance with rectal temperature. The digital device tended indeed to provide lower readings than the mercury rectal thermometer, with the difference being negative in 61% of cases in our sample. Undoubtedly, infrared skin thermometer has the advantage that the temperature can be recorded in only a few seconds and it is not an expensive device (€59 in Italy). The intra-operator as well as inter-operator agreement of the measurements in our study indicate that the infrared skin thermometer provides reproducible values. Although the study was not designed to evaluate the safety of use and the acceptability of the infrared skin temperature, we did not encounter any adverse effects nor was there any apparent discomfort. Finally, in comparison with the ear thermometer, as the infrared skin thermometer measures the temperature of the forehead, this method avoids the technical problems associated with this modality of measurement or the chance of occlusion of the ear canal.
A possible limitation of the study was the narrow range of temperatures measured in these newborns, the majority of measurements having been taken in a temperature controlled environment. Thus our data should preferably be extrapolated to measurements taken under the same conditions.
In conclusion, measurement of infrared skin temperature with an infrared skin thermometer is easy and associated with a low risk of technical error due to operator’s skill. According to our data, infrared skin measurement cannot act as a substitute for rectal measurement in all cases; however, the differences between the two measurements were modest and this is encouraging for the use of infrared skin thermometer in monitoring body temperature in newborns.
What is already known on this topic
The mercury thermometer is the commonest method for measurement of body temperature in the neonatal period.
However, this method is associated with the inconvenience of a long period of equilibration.
Also, substantial changes in the measured temperature can occur up to 3 min, and it can disturb procedures in neonatal intensive care units during this time.
What this study adds
The infrared skin thermometer is a useful and valid device for easy and rapid measurement of the skin temperature in the neonatal period.
Footnotes
Funding: This study was not supported by any funds or other forms of personal institutional financing from company producing the thermometer.
Competing interests: None.