Article Text

Abstract
Introduction Neonatal infection is an important cause of morbidity and mortality. Neonatal infection surveillance networks are necessary for defining the epidemiology of infections and monitoring changes over time.
Design Prospective multicentre surveillance using a web-based database.
Setting 12 English neonatal units.
Participants Newborns admitted in 2006–2008, with positive blood, cerebrospinal fluid or urine culture and treated with antibiotics for at least 5 days.
Outcome measure Incidence, age at infection, pathogens and antibiotic resistance profiles.
Results With the inclusion of coagulase negative Staphylococci (CoNS), the incidence of all neonatal infection was 8/1000 live births and 71/1000 neonatal admissions (2007–2008). The majority of infections occurred in premature (<37 weeks) and low birthweight (<2500 g) infants (82% and 81%, respectively). The incidence of early onset sepsis (EOS; ≤48 h of age) was 0.9/1000 live births and 9/1000 neonatal admissions, and group B Streptococcus (58%) and Escherichia coli (18%) were the most common organisms. The incidence of late onset sepsis (LOS; >48 h of age) was 3/1000 live births and 29/1000 neonatal admissions (7/1000 live births and 61/1000 admissions including CoNS) and the most common organisms were CoNS (54%), Enterobacteriaceae (21%) and Staphylococcus aureus (18%, 11% of which were methicillin resistant S aureus). Fungi accounted for 9% of LOS (72% Candida albicans). The majority of pathogens causing EOS (95%) and LOS (84%) were susceptible to commonly used empiric first line antibiotic combinations of penicillin/gentamicin and flucloxacillin/gentamicin, respectively (excluding CoNS).
Conclusions The authors have established NeonIN in England and defined the current epidemiology of neonatal infections. These data can be used for benchmarking among units, international comparisons and as a platform for interventional studies.
Statistics from Altmetric.com
Introduction
Neonatal infection is an important cause of morbidity, prolonged hospital stay and mortality among infants, particularly those born preterm and of very low birthweight (VLBW).1 Pathogens causing neonatal infections and their antibiotic susceptibility patterns may change over time2,–,4 and differ between countries.5 It is therefore essential to monitor the epidemiology of neonatal infections to inform policy and clinical practice.
Neonatal infection surveillance networks have been established in a number of countries, and include the Australasian Study Group for Neonatal Infections (ASGNI),6 the Israeli National VLBW Infant Database,7 the Canadian Neonatal Network (http://www.canadianneonatalnetwork.org), the US National Institute of Child Health and Human Development (NICHD) Neonatal Research Network (http://www.nichd.nih.gov), the Vermont Oxford Network (https://www.vtoxford.org/home.aspx) and the German Krankenhaus-Infektions-Surveillance-System (NeoKISS).8 With the exceptions of the ASGNI and Canadian groups, existing neonatal infection networks focus on VLBW babies cared for in tertiary neonatal units. A variety of data are collected on culture proven sepsis, as well as presumed and possible sepsis.8 Definitions of sepsis vary between networks, but all consist of a combination of clinical and laboratory parameters.3 Neonatal infection networks have been useful for benchmarking practice,9 as a platform for interventional studies10 and for monitoring changes in pathogens3 and their antibiotic resistance over time.6 11 They have also been used to document changes in clinical practice,12 inform policy and improve quality of care.13
What is already known on this topic
▶ Neonatal infections are an important cause of morbidity and mortality, particularly in very low birthweight infants.
▶ Neonatal infection surveillance networks have been established in several countries and are useful for documenting changes in clinical practice, benchmarking, monitoring changes in pathogens and their antibiotic resistance over time, informing policy and improving quality of care.
What this study adds
▶ The neonatal infection surveillance network (NeonIN) monitors the epidemiology and empiric antibiotic treatment of neonatal infections.
▶ Penicillin and gentamicin in combination cover 95% of early onset pathogens; flucloxacillin and gentamicin cover most late onset pathogens.
▶ Compared with the USA, group B Streptococcus causes a higher proportion and Escherichia coli a lower proportion of early onset infections.
The UK has not had a national longitudinal neonatal infection surveillance system.14 Studies conducted through the British Paediatric Surveillance Unit (BPSU) have been invaluable in describing the epidemiology of specific neonatal infections such as group B Streptococcus (GBS),15 Herpes simplex,16 fungal infections in VLBW infants17 and methicillin resistant Staphylococcus aureus (MRSA),18 as well as clinical syndromes such as neonatal meningitis.19 However, the BPSU is not a suitable mechanism for longitudinal surveillance. Additionally, the Health Protection Agency (HPA) routinely collects data on bacteraemias in England and Wales, but it captures only limited clinical data.20
In 2004 NeonIN was established with the objective of collecting clinical and microbiological data on episodes of neonatal infection on a longitudinal basis. Currently, 16 units are contributing data from across England. We report the incidence, pathogens and antibiotic resistance profiles of infections captured in NeonIN in the 3 years between 1 January 2006 and 31 December 2008.
Methods
An episode of neonatal infection was defined as a positive culture collected from a normally sterile site (blood, cerebrospinal fluid (CSF) and supra-pubic aspirate) for which clinicians prescribed at least 5 days of antibiotic treatment. Repeatedly positive samples with the same organism were considered as part of the same episode if the period between samples was less than 7 days for all organisms, other than coagulase negative Staphylococci (CoNS) and fungal infections, for which the specified period was 10 days. Early onset sepsis (EOS) was defined as infection in the first 48 h of life and late onset sepsis (LOS) as infection occurring thereafter. This age cut-off was chosen as it probably best reflects the transition between infections caused by pathogens acquired by vertical transmission and those acquired by horizontal transmission, and because it has also been used by other surveillance networks. However, the data were collected such that other time points could also be applied (see online supplementary tables 1–3). Small for gestational age (SGA) was defined as birthweight <10th centile for gestational age.
Because bacteraemia with CoNS may indicate a true infection or may reflect contamination,21 there is debate about its inclusion in infection surveillance data. From 2007 onwards we elected to include CoNS bacteraemia if the episode was treated for a minimum of 5 days with appropriate antibiotics (ie, generally vancomycin), a definition consistent with that used by other networks (http://www.nichd.nih.gov; https://www.vtoxford.org/home.aspx).
A standardised proforma was completed by the clinician for each positive culture, and included the infant's demographic details (birth weight, gestational age, gender), clinical information and microbiological data, as well as the antibiotic resistance profile of the isolate. Currently most microbiology units use automated antibiotic sensitivity testing techniques such as VITEK 2. However, as the database uses routine data, this was not prespecified and may not be consistent over time or among units. Anonymised data were then transferred onto a remote Microsoft Access database (NeonIN). Data were cross-checked against the local microbiology databases on a regular basis to ensure completeness.
Data regarding the total number of live births and the number of neonatal unit admissions by birth weight and gestational age bands were collected for each unit. Participating units were designated as level 1, 2 or 3 according to British Association of Perinatal Medicine criteria.22
Data were analysed with STATA 9. Antibiotic resistance data were analysed in relation to the antimicrobial combinations recommended by the British National Formulary,23 that is, benzylpenicillin and gentamicin or amoxicillin and cefotaxime for EOS and flucloxacillin and gentamicin or amoxicillin and cefotaxime for LOS. Organisms were deemed resistant to the combinations if resistant to both antibiotics and sensitive if sensitive to at least one of the antibiotics in the combination.
The NeonIN study received ethics approval from the London-Surrey Borders Research Ethics Committee in April 2005 (05/Q0806/34). Each participating centre received separate approval from their local ethics committees prior to joining the network.
Results
All infections for 2006–2008 (excluding CoNS)
Data were available for eight units in 2006, nine in 2007 and 12 in 2008.24 A total of 541 episodes of neonatal infection (representing 443 infants) were recorded. Of the participating units, two were level 2, and 10 were level 3; 50% of the units managed infants with surgical conditions (general, abdominal and cardiac surgery).
Infection was more common in male (n=247, 56%) than in female infants (n=196, 46%; p=0.0001). The majority of episodes of infection (n=443, 82%,) occurred in infants born at <37 weeks gestation, of which 71% (n=313) occurred in infants ≤32 weeks gestation. Similarly, 81% of episodes occurred in infants with a birth weight <2500 g (n=437), of which 53% (n=237) occurred in infants <1000 g, 18% (n=81) of infants were SGA, 9% (n=51) had more than one episode of sepsis, and 3% (n=16) had more than one pathogen cultured during the same episode.
While most episodes were diagnosed through positive blood cultures (505, 93%), pathogens were isolated from the CSF in 24 infants, of whom nine (37%) had negative blood cultures. Eight of the latter were late onset, with a median age of infection of 17 days (range 6–92 days). The pathogens responsible for late onset meningitis were GBS, Enterobacter cloacae (two), Escherichia coli (two), Citrobacter, Streptococcus viridans and Enterococcus faecalis. The early onset blood culture negative meningitis was caused by Candida albicans.
The remaining isolates were obtained from urine (27, 5%). All urine infections were late onset (median 19 days, range 3–279 days).
The incidence of neonatal infection was 4.1 per 1000 live births (541/130,763)and 38 per 1000 neonatal admissions (541/14,225) and was similar across the 3 years of surveillance (p>0.1). The distribution of infections was also comparable for birth weight and gestational age categories. However, in 2008 there was a smaller proportion of infection episodes in infants over 2500 g and a larger proportion in extremely premature infants (≤32 weeks gestation) compared to previous years (p<0.001 and p=0.002, respectively; table 1).
Infection episodes per year as a percentage of all live births in each birth weight category
Early onset sepsis (≤48 h of age)
EOS incidence was 0.9 per 1000 live births and 9 per 1000 neonatal admissions and was similar for the 3 years of surveillance (p>0.1).
Of the 125 episodes of EOS, 74% (93) were due to gram-positive organisms, 25% (31) to gram-negative organisms and one to C albicans (table 2); GBS was the most frequent organism isolated. The incidence of early onset GBS was not significantly different over the 3-year period, averaging 0.5 per 1000 live births (65/130,763). The majority of organisms (95%) were susceptible to the two most commonly used empiric antibiotic combinations. The major exception to this was S aureus, all of which were resistant to the benzylpenicillin and gentamicin combination.
Most common pathogens
Late onset sepsis (>48 h of age)
The incidence of LOS in each of the 3 years of surveillance was similar (overall 3/1000 live births and 29/1000 neonatal admissions, n=416; p>0.1 for comparison between years). The median age at infection was 18 days (range 3–386 days) and the majority of episodes (70%) occurred in extremely premature infants (85% were <37 weeks gestation). Overall, gram-positive organisms accounted for 49% (203/416), gram-negative for 42% (177/416) and fungi for the remaining 9% (36/416) of episodes. The predominant fungus isolated was C albicans (72%) and the proportion of VLBW infants with one of more episodes of Candida sepsis was 1.8% in 2006, 1.2% in 2007 and 1.3% in 2008.
The most common pathogens causing LOS are listed in table 2.
With the exclusion of CoNS, the majority of isolates were susceptible to the two most commonly used empiric antibiotic combinations, although susceptibility to flucloxacillin and gentamicin was higher (84%) than to amoxicillin and cefotaxime (79%) due to the relatively high resistance rate of Enterobacteriacae to cephalosporins (table 3).
LOS resistance
CoNS infections (2007–2008)
There were 358 episodes of CoNS sepsis in 321 infants (166 females and 155 males) in 2007–2008, increasing the total incidence for all infections to 8/1000 live births (728/91,243) and 71/1000 neonatal admissions (728/10,315).
CoNS were associated with 21 episodes of EOS (representing 20% of all EOS) and 337 episodes of LOS (representing 54% of all LOS). The majority of CoNS infections were in infants ≤32 weeks gestation (307, 86%) and in extremely low birthweight infants (234, 65%).
Age at disease by pathogen (2007–2008)
Almost a quarter (23%) of all neonatal infections occurred in the first 48 h of life (early onset) and the majority of these occurred on the first day (88%). Using 72 h as the threshold for early onset infections increased the percentage of early onset infections to 26% and made the most difference (proportionately) to the following pathogens: Enterobacter, other Streptococci, C albicans and S aureus (see online supplementary tables 1–3). The E coli associated with EOS (<48 h) also appeared to be different to those associated with LOS based on antibiotic susceptibilities; 83% of early onset E coli were amoxicillin resistant but were otherwise fully susceptible, whereas 18% of late onset E coli were amoxicillin resistant, 24% were resistant to augmentin, 28% to ceftazidime, 27% to ciprofloxacin, 12% to gentamicin and 25% to tobramicin. This difference is noted in E coli beginning from day 3 of life. Finally, using a definition for early onset infections of 0–6 days,15 the percentage of early onset infection increases to 33% but the number of GBS infections barely changed (an additional three between days 3 and 6).
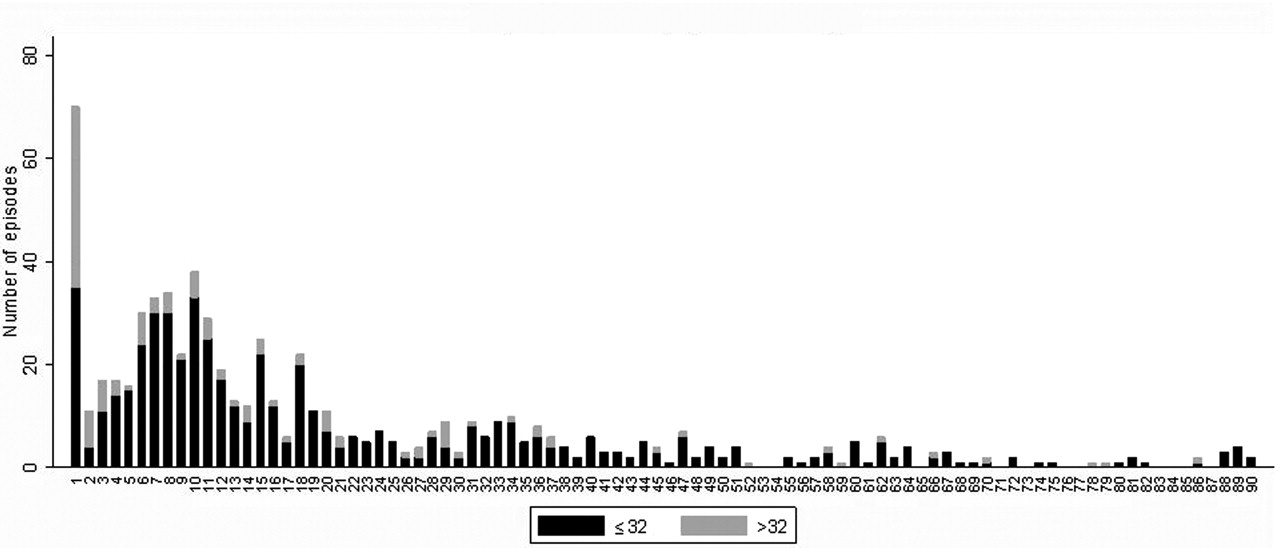
Approximately one half of infections on day 1 occurred in infants over 2500 g (49%) and 63% occurred in infants of 32 weeks gestation or above (figure 1). Of all late onset infections, 18% occurred between days 3 and 7 and 66% in the first month of life. The age at disease was not influenced by gender (p=0.62) but varied significantly by pathogen. GBS occurred most often on the first day of life, followed by E coli and CoNS. Among late onset pathogens, E coli infections peaked on day 6 and CoNS on days 6–11 (remaining prevalent for the first month), while Enterobacteriaceae, S aureus and Enterococci occurred later, without a discernable pattern (figure 2).

Day of infection by gestational age.

{kind=link}
{kind=link}
Pathogens per day of onset. CoNS, coagulase negative Staphylococci; E coli, Escherichia coli; GBS, group B Streptococcus; S aureus, Staphylococcus aureus.
Discussion
We have established a neonatal surveillance network and described the burden of infections in a number of English neonatal units. Preterm and low birthweight babies carry the highest burden of infection, with 26% of all babies <1000 g experiencing one or more episodes of infection during their neonatal stay. Neonatal infections in this population are associated with prolonged hospitalisation, adverse neurodevelopmental outcome1 and increased mortalities.25
The two main pathogens causing EOS were consistently GBS and E coli, accounting for approximately two-thirds of all episodes. The incidence of early onset GBS disease averaged 0.5/1000 live births, equivalent to the 0.48/1000 reported from the national BPSU surveillance conducted in 2000–2001.15 It therefore seems unlikely that a significant reduction in early onset GBS disease occurred despite the introduction of national GBS prevention guidelines in 2003.26 This is supported by passive surveillance data reported to the HPA.27 An explanation for this is offered by a recent audit conducted through the NeonIN units which indicated that a significant proportion of early onset GBS cases did not receive intrapartum antibiotic prophylaxis (IAP) despite the presence of risk factors.28 In contrast, in the USA and Australasia the incidence of early onset GBS has decreased29 30 with the introduction of robust IAP policies.31 Attention to new or improved GBS prevention policies in the UK is urgently required.
A wider range of pathogens accounts for LOS, although over 80% were due to CoNS, S aureus, Enterobacteriacea, E coli and Enterococci. Preterm infants have the highest burden of LOS, with 19% of all babies <1000 g experiencing one or more episodes of late onset infection, excluding CoNS, increasing to 42% with the inclusion of CoNS.
Comparisons can be made between NeonIN data and that of several other UK studies. The incidence of MRSA infections over the 3-year period (eight episodes, 6/100 000 live births) is comparable with that of a recent national MRSA surveillance study (8/100 000 live births).18 We can report that NeonIN infants with MRSA infections were predominantly female, of low birthweight (median 820 g) and experienced their infection at a median of 36 days of age (all were late onset). A single centre study by Haque et al reported a similar incidence of neonatal sepsis (1% of live births and 8% of neonatal admissions) and distribution of causative pathogens,32 as did a perinatal mortality study conducted in the North of England.33 The incidence of VLBW infants experiencing invasive fungal infection (14/1000 over 3 years) is comparable with the annual incidence of 10/1000 reported from the national BPSU study in 2003–2004.17 The slightly higher incidence may indicate an increase over the last 5 years or may reflect the predominance of tertiary units in our network, and is worthy of further study. Taken together with our equivalent incidence of early onset GBS disease to that of national surveillance,15 these comparisons provide some support for the generalisability of NeonIN surveillance data to the UK neonatal population.
Comparison of NeonIN data with data from other international neonatal infection surveillance networks provides some interesting insights.6 11 There is a striking predominance of E coli sepsis in the USA, partly accounted for by a lower proportion of GBS and CoNS episodes (see online supplementary table 4). Similarly, when compared to the Australasian data, GBS is a more common pathogen in UK units (NeonIN: 0.49/1000 live births vs ASGNI: 0.25/1000 live births6), while E coli is less commonly found (NeonIN: 0.17/1000 live births and 2.9/1000 VLBW vs ASGNI: 0.3/1000 live births and 6.2/1000 VLBW6). A plausible but partial explanation is the differences in use of IAP as discussed earlier. Time-trend analysis of NICHD data showed that the decline in GBS coincided with the rise in E coli, and specifically of ampicillin resistant strains.34 This, however, had not been observed in the Australasian series.6
Comparison of LOS data from NeonIN with NICHD and NeoKISS data25 35 36 reveals a comparable incidence of infection episodes.36 NeonIN and NeoKISS surveillance data show less than half the incidence of fungal sepsis compared with the NICHD network (see online supplementary table 5).
NeonIN data indicate that approximately 95% of early onset infections are susceptible to a penicillin/gentamicin combination, which, therefore, appears to be a satisfactory empiric choice. The only early onset pathogen that is not covered by this regimen is S aureus and further work may be able to identify babies at high risk for this pathogen for whom empiric therapy should be modified. It is worth noting that there were no deaths among early onset S aureus episodes. With the exclusion of CoNS, the majority of LOS infections (84%) are also susceptible to the relatively narrow spectrum combination of flucloxacillin and gentamicin. The British National Formulary for Children (BNFC) also offers cefotaxime and ampicillin as an alternative regimen for EOS and LOS; however, our data do not support this. Indeed this combination provides less coverage for the relevant disease causing organisms, yet as the broader spectrum combination, has a greater potential to promote antibiotic resistance and the emergence of other pathogens such as fungi.13 37 It is important however, that neonatal units are aware of their local resistance patterns and that this is reflected in their empiric antibiotic policies.
There is a wider question regarding the use of aminoglycosides that needs to be tackled by the neonatal community regarding the potential for ototoxicity, especially in those with the m.1555A>G genetic mutation.38 This requires further research and discussion.
An important role for the empiric use of cefotaxime is in suspected meningitis, where the favourable CSF penetration of cefotaxime makes it the preferred agent (in combination with ampicillin and possibly an aminoglycoside39). Meningitis should therefore be excluded as soon as possible.
Neither of the BNFC recommended empiric combinations adequately accounts for CoNS, although it may be argued that empiric cover for this pathogen is not essential. CoNS are a rare cause of life-threatening infection in neonates.4 Moreover, excessive use of vancomycin may be associated with antibiotic resistance and emergence of other pathogens.40 A reasonable approach is therefore to institute antibiotic therapy for CoNS only when a positive culture is obtained and deemed to be clinically relevant. Further study is required on whether a specific high risk group can be identified that would merit empiric use of vancomycin. The case definition used for sepsis may also be criticised as being too simple. It is clear, however, that this is essential to ensure the cooperation of busy clinicians and the completeness of data collection. It is also consistent with that used in other well established surveillance systems (http://www.nichd.nih.gov; https://www.vtoxford.org/home.aspx). The potential weakness of such a definition relates to the interpretation of positive cultures due to pathogens that are also frequent skin contaminants (especially CoNS). This is based on the clinician's decision to treat with antibiotics for at least 5 days and is therefore likely to be subjective. This is particularly so for early onset infections caused by CoNS, which in our dataset are much more numerousthan expected. As with late onset CoNS episodes, we suspect that this reflects an overestimation resulting from this pragmatic definition of sepsis. However, it ensures some consistency in assessing the burden of CoNS infections and will enable comparison over time and between units. An alternative is to incorporate more clinical and laboratory markers into the case definition.41However, this requires more effort from clinicians and may therefore compromise data completeness. We are investigating ways that information on markers may be incorporated into the database and still ensure ease of use.
In summary, NeonIN presents the first national data on the epidemiology of neonatal sepsis and provides an insight into the relevant pathogens and the appropriate antibiotics for empiric therapy. Ongoing expansion of the network across the UK will strengthen the richness and utility of the database.
Acknowledgments
Dr Hannah Baynes, Dr Zoe Smith, Dr Lee Geraint, Dr Peter Chow, Dr John Chang, Dr Paul Clarke, Julia Hill, Louise Stickland, Claire Long, Dr Imogen Storey, Dr Lorna Gillespie, Dr Bernd Reichert, Dr Mithilesh Lal, Dr Ruppa Geethanath, Dr Kate Farrer, Dr Priya Muthukumar, Debbie Marshall, Dr Santosh Pattnayak and the NeonIN neonatal infection surveillance network.
References
Footnotes
-
Competing interests None.
-
Ethics approval The NeonIN study received ethics approval from the London-Surrey Borders Research Ethics Committee in April 2005 (05/Q0806/34). Each participating centre received separate approval from their local ethics committees prior to joining the network.
-
Provenance and peer review Not commissioned; externally peer reviewed.