Article Text

Abstract
Background Randomised trials suggest that high-flow (HF) therapy is comparable with continuous positive airway pressure (CPAP) for postextubation respiratory support in neonates, and HF has been widely adopted in neonatal intensive care.
Methods We conducted a population-based study of very preterm infants born <32 weeks’ gestation within the Australian and New Zealand Neonatal Network (ANZNN) data set from 2009 to 2012, who received respiratory support with HF.
Results 3372 very preterm infants were treated with HF. HF use in this population increased significantly from 15% in 2009 to 35% in 2012. In 2012, 53% (542/1029) of extremely preterm infants born <28 weeks’ gestation received HF. 98% (3308/3372) of infants had received endotracheal ventilation or CPAP prior to receiving HF. The maximum HF gas flow was ≤8 L/min in almost all infants.
Conclusions HF use in extremely preterm and very preterm infants increased significantly within the ANZNN from 2009 to 2012.
- Non-invasive ventilation
- Infant, premature
- Respiratory distress syndrome, newborn
Statistics from Altmetric.com
What is already known on this topic
Surveys indicate that prior to publication of good quality evidence from clinical trials, high-flow (HF) therapy was adopted by many neonatal clinicians.
Randomised trials suggest that HF is comparable with continuous positive airway pressure (CPAP) for postextubation support in preterm infants.
What this study adds
The use of HF therapy has increased significantly in extremely preterm and very preterm infants in Australia and New Zealand.
Most very preterm infants receiving HF had previously received endotracheal ventilation, CPAP or both.
The majority of infants received HF gas flows in keeping with those used in subsequently published randomised trials.
Background
While endotracheal ventilation is a life-saving treatment for many infants, its association with adverse outcomes such as chronic lung disease (CLD) has resulted in increasing interest in ‘non-invasive’ respiratory support modes. These include nasal continuous positive airway pressure (CPAP) and the more recently introduced high-flow (HF) therapy. Randomised controlled trials suggest that HF is comparable with CPAP for postextubation respiratory support in neonates.1–3 Trials investigating HF have typically recruited very preterm infants (born <32 weeks’ gestational age (GA)), following extubation. Surveys have indicated that HF was widely adopted into use in neonatal units around the world prior to the publication of randomised trials, in the absence of good quality evidence of efficacy and safety and often without clinical treatment protocols.4
The Australian and New Zealand Neonatal Network (ANZNN) is a network of 29 tertiary neonatal intensive care units and 27 non-tertiary neonatal units in Australia and New Zealand. Infants are registered in the ANZNN data set if they are born at <32 weeks’ GA or <1500 g, receive respiratory support for ≥4 h, have major surgery or receive therapeutic hypothermia. We aimed to assess trends in HF use in infants <32 weeks’ GA within the ANZNN. The use of HF was first recorded in 2009, and 2012 is the most recent data available.
Methods
We conducted a population-based study of all infants <32 weeks’ GA within the ANZNN data set who received respiratory support between 2009 and 2012, and identified all infants who received HF. Outcomes were selected from those routinely recorded for all ANZNN registrants.5 These included demographic data such as birth weight and gestation, exposure to other respiratory support modes (endotracheal ventilation, CPAP), the duration of HF, HF gas flows received, pneumothorax requiring drainage, CLD and death. CLD was defined as receiving supplemental oxygen and/or respiratory support (endotracheal ventilation, CPAP or HF) at 36 weeks’ postmenstrual age. Subgroup analysis by GA (<28 weeks; ≥28 weeks) was performed.
Data were analysed using Stata V.13.1 (Stata Corp., College Station, Texas, USA). A Pearson χ2 test was used to assess significant linear trends over time.
Results
From 2009 to 2012 in the ANZNN, 13 298 infants <32 weeks’ GA (GA at birth mean±SD 28.4±2.2 weeks, birth weight median (IQR) 1203 (905–1500) g) received respiratory support during their admission. Of these, 3372 or 25.4% (GA at birth mean±SD 27.6±2.1 weeks, median weight 1031 (820–1300) g) were treated with HF during admission. The majority of these infants (65%) were delivered by caesarean section, they had high rates of antenatal steroid exposure (88%) and 29% were multiple births. Fifty-two per cent (1744/3372) of infants who received HF had been intubated in the delivery room (52%), and 75% (2519/3372) received exogenous surfactant treatment.
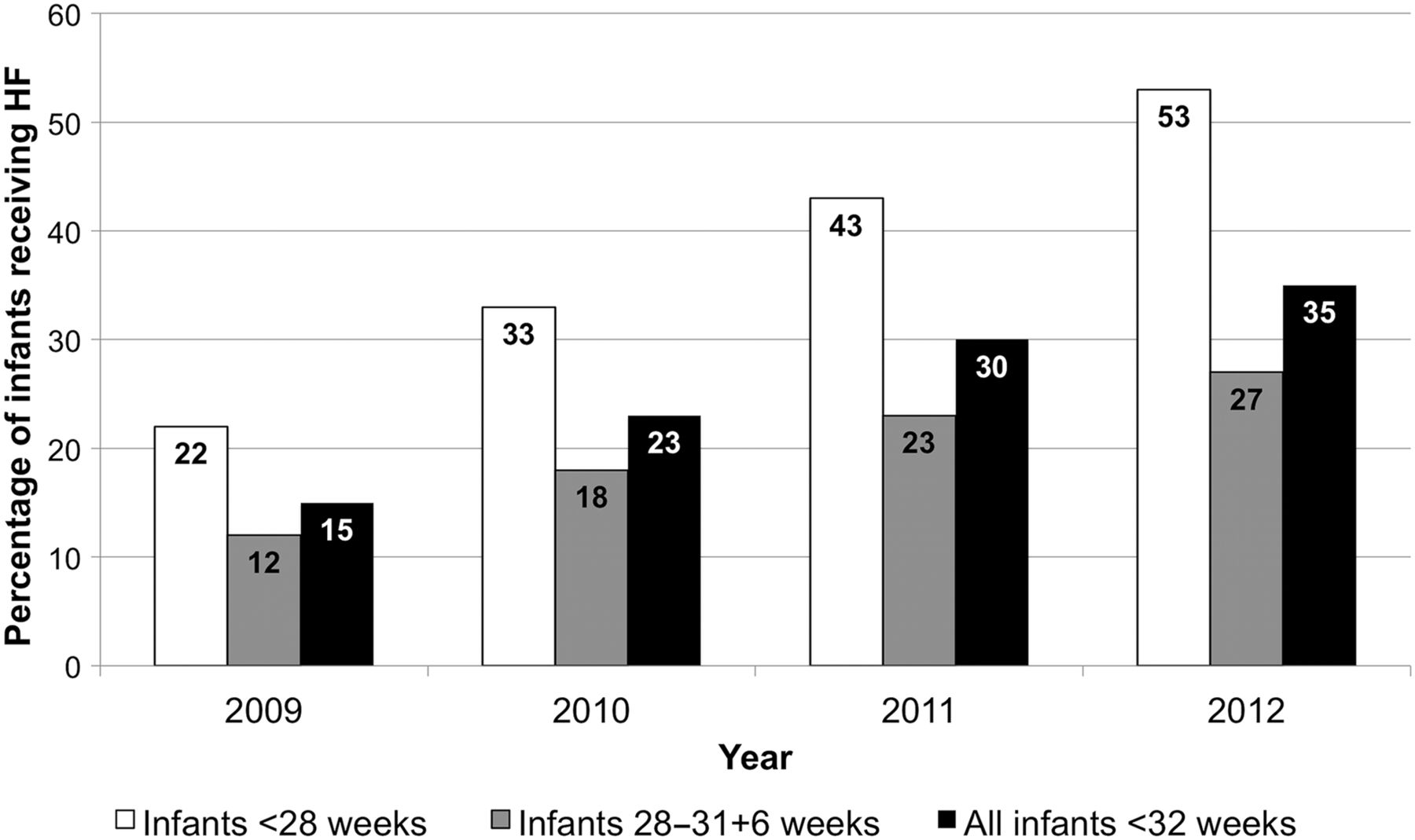
The proportion of infants <32 weeks’ GA who received HF during admission is shown in figure 1. HF use increased significantly over time overall, and within the GA subgroups (p<0.01), between 2009 and 2012.

{kind=link}
Proportion of very preterm infants receiving respiratory support treated with high flow (HF), by calendar year.
Outcomes for infants <32 weeks’ GA receiving HF are shown in table 1.
Outcomes of infants <32 weeks’ GA receiving HF
The median time on HF was 12 days; 17 days for infants <28 weeks’ GA and 8 days for those 28–31+6 weeks’ GA. Of the 3372 HF-treated infants, 3021 (90%) had received CPAP, 2408 (71%) had received endotracheal ventilation and 2170 (64%) had received both, prior to receiving HF. Only 2% (64/3372) of HF-treated infants received HF as their primary mode of respiratory support after birth. Pneumothorax occurred in 144 infants, but in 129 cases this was prior to the infant receiving HF support. Almost all infants had a maximum received gas flow of ≤8L/min, with only 14 infants (0.4%) receiving a flow >8 L/min. These 14 infants were a high-risk group: 11 had CLD, their median age at last respiratory support or oxygen was 133 days and 6 died before discharge.
Discussion
This study is the largest published cohort of neonates treated with HF. In comparison with all infants <32 weeks’ GA who received respiratory support within the ANZNN from 2009 to 2012, the 3372 infants who received HF were of slightly lower GA and birth weight.
HF use increased significantly during the study period. By 2012, of those infants who received respiratory support, 35% (1156/3321) of infants <32 weeks’ GA, and 53% (542/1029) of infants <28 weeks’ GA, received HF during hospital admission. This increase in usage prior to published evidence of efficacy would seem to support the notion that the popularity of HF has resulted from its perceived advantages (better access to the infant, ease of use, ease of providing skin-to-skin care and oral feeds),4 and those subsequently proven (reduced nasal trauma).1–3 We suspect that since 2012 HF use in infants <32 weeks’ GA has continued to increase. This trend also appears to be occurring elsewhere: the Vermont Oxford Network reported an adjusted difference (95% CI) for HF use in infants born at 501–1500 g of 13.1 (12.5% to 13.8%) in 2009 in comparison with 2006.6
Although this cohort was managed prior to publication of large randomised trials comparing HF and CPAP as postextubation support, these infants generally received treatment consistent with subsequently published evidence.1–3 Most infants who received HF had previously received endotracheal ventilation or CPAP. The use of HF as primary respiratory support, for which evidence remains sparse, was very rare. For the majority of infants, HF was first initiated after 2 weeks of age, and it was continued for a median of 12 days in total. HF gas flows used were also in keeping with the published trials (2–8 L/min)1–3 for the majority of infants.
While the start and end times and total duration of each respiratory support mode are known, details of changes between support modes are not collected within the ANZNN data set. Unfortunately, this prevented a more detailed analysis of the use of HF as a transitional therapy after endotracheal ventilation or CPAP (the manner in which HF was used in the majority of these infants). There is some concern that HF use in this manner may lead to prolonged exposure to respiratory support or oxygen or delay hospital discharge. Two trials in which infants who were stable on CPAP were randomised to either weaning directly from CPAP or weaning using HF therapy had contrasting results: Abdel-Hady7 found infants weaned using HF to have prolonged exposure to respiratory support and oxygen, but no difference in the length of hospital stay, whereas Badiee8 found there to be no difference in age at cessation of respiratory support between groups, and a reduction in the duration of oxygen treatment and hospital stay in the HF infants.
While one postextubation randomised trial3 showed HF treatment to be associated with prolonged duration of respiratory support, a recent meta-analysis of this and four additional studies, including 818 infants, showed no difference between the HF and CPAP groups.9 However, these trials were conducted using strict protocols. While we cannot draw conclusions from our data, neonatal medical and nursing staff should be vigilant in avoiding inadvertently prolonging respiratory support when using HF.
The low rate of pneumothorax in these infants is relatively reassuring. While the incidence of CLD (43%) is high for infants <32 weeks’ GA as a whole, it is important to recognise that this is a highly selected sample, who commenced HF (ie, required ongoing respiratory support) at median 17 days of age. Infants with milder respiratory disease and briefer respiratory support requirements were therefore excluded. The infants most at risk of CLD (those with prolonged respiratory support requirements and born <28 weeks’ GA) were the group in whom HF was most frequently used. While a 2% mortality rate is low, the very preterm infants at highest risk are likely to have died early during their admission, and are therefore unlikely to have received HF treatment at all.
In addition to the number of included infants, strengths of this study are that it is based on a robust set of prospectively collected data, from a large network of neonatal units, and hence captures potential variations in practice across different units and geographical areas in Australia and New Zealand. This study is limited to information that is routinely collected within the ANZNN data set, which, while extensive, must also be feasible for units to collect. As such there is some information that might be of interest in this population, which is unavailable (eg, fraction of inspired oxygen). As mentioned above, it would have been interesting to conduct a more detailed analysis of HF use as a transitional therapy after endotracheal ventilation or CPAP, but the available data does not allow this. Furthermore, our population includes only those infants <32 weeks’ GA treated with HF, so these results cannot be extrapolated to all infants <32 weeks’ GA.
Conclusion
This population-based study of very preterm infants within the ANZNN showed a significant increase in the use of HF therapy from 2009 to 2012. It is an example of a therapy adopted into practice prior to appropriate safety and efficacy data, but which has proved successful and is now supported by good data. HF was most commonly used as postextubation support, at flows of <8 L/min, in keeping with subsequently published randomised trials. Patterns of HF use are likely to continue to change over time and should be guided by emerging evidence from well-designed clinical trials.
Acknowledgments
We wish to thank Ms Sharon Chow, ANZNN coordinator for extracting and providing the required data, and the ANZNN Advisory Council for their support of this study.
Footnotes
Contributors CR, LO, BM and PD conceptualised and designed the study, interpreted the data and revised and approved the final manuscript. CR identified the required data, which were provided by the ANZNN from their data set. CR analysed the data and drafted the initial manuscript. He is guarantor.
Competing interests None declared.
Ethics approval The study was approved by The Royal Children's Hospital human research ethics committee, Melbourne.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms