Article Text

Abstract
Children with visual impairment and a condition affecting their neurodevelopment (children with VND) may require extensive and specialised help but evidence on the most effective strategies for visual improvement is lacking. We defined a PICO format (Population, Intervention, Comparator, Outcome) for a scoping review and systematically searched 13 databases. Two reviewers assessed the abstracts for inclusion and a third arbitrated in cases of disagreement. We abstracted data from included studies. We found 4450 abstracts from which we identified 107 papers for inclusion. Of these, 42 related to interventions involving a change in visual input or function: 5 controlled trials, 8 before and after studies and 29 case reports. The strongest evidence supported the provision of spectacles to improve distance or near vision and the use of ultraviolet light as environmental modification for training. Less strong but suggestive evidence supported training/practice routines to improve acuity or oculomotor control. Interventions exist to help children with VND and current recommendations that they are assessed by a vision specialist are supported by the evidence. More information is needed on the effectiveness of training/practice programmes which may promote improved function, and of environmental modifications to facilitate engagement of children with VND with the surroundings.
- Child health (paediatrics)
- Vision
- Treatment other
- Treatment Medical
- Treatment Surgery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Severe visual impairment or blindness in children is often associated with other impairments.1 Children with neurodevelopmental disorders have an increased prevalence of visual impairments and the Royal College of Ophthalmologists2 and the UK government National Service Framework for Disabled Children3 recommend that such children have a routine vision check as part of their multidisciplinary care.
Assessment and management of children with visual and neurodevelopmental problems (VND) will differ according to their cognitive and motor development and day-to-day activities. We found systematic reviews or guidelines summarising the evidence supporting paediatric vision problem such as amblyopia,4–6 congenital cataract7 or retinopathy of prematurity,8 but none specifically relevant to children with VND. We therefore carried out a scoping review of the literature to identify studies of interventions that are used for children with VND.
Methods
We formed a scoping group and we defined a PICO (Population, Intervention, Comparator, Outcome) format to structure the literature search. Our population of interest comprised those aged less than 18 years with a clearly defined vision problem and a clearly defined neurodevelopmental problem. We wrote and updated a protocol. We followed the recommendations listed in the PRISMA statement as far as were applicable for a scoping review (see attached checklist in online supplementary appendix 1). We considered any intervention and planned initially to include studies only if there was a placebo or alternative treatment as comparator. This was revised after pilot searches yielded very few such studies: we therefore present all studies we found and have used the Oxford Centre for Evidence Based Medicine (OCEBM) levels table as an aid to seeing at a glance the likely strength of evidence provided by the experimental studies we have included.9
Our information specialist (CB) searched the following databases in January 2011: ASSIA (CSA); AMED (OVID); CINAHL (EBSCO); Cochrane Library; Embase (OVID); Medline (OVID); PsychINFO (OVID); SCOPUS; Web of Science; ISI Proceedings (conference papers); Dissertation Express (Proquest); ETHoS and Index to Theses. No date delimiters were set. The results were downloaded into EndNote and duplicates were removed. Hand-searches were carried out of the supplements to Developmental Medicine and Child Neurology. A sample search is shown in online supplementary appendix 2.
Two authors (CW and KN) independently reviewed each abstract and decided whether they should be included or excluded according to the PICO, or whether more information was needed to make this decision. A third author (JMW) arbitrated in cases where there was disagreement and consensus was reached. The full text of all papers identified as having potential for inclusion was requested excluding those not in English or unavailable electronically or by interlibrary loan. One author abstracted data from papers (CW) and another checked the data (KN), using predesigned checklists.10
Results
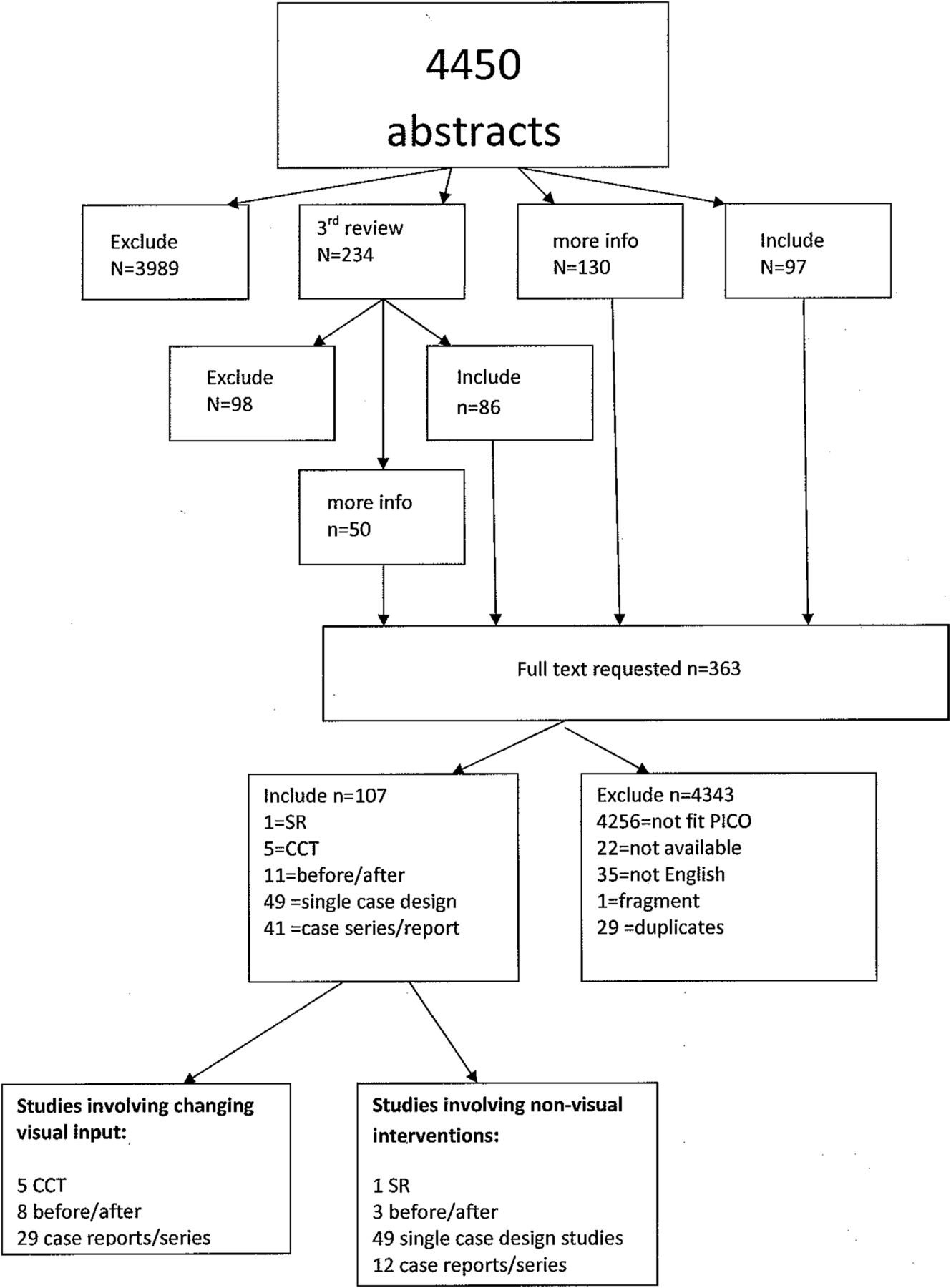
As shown in figure 1, after the initial selection process there were 107 papers for inclusion, of which 1 was a systematic review, 5 were controlled clinical trials (CCTs), 11 were before/after studies, 49 were single experimental case design studies (where all subjects are described individually) and 41 were observational case series or reports. We present here the findings for the 42 of these studies that involved manipulating or improving the child's visual input—these were 5 controlled trials, 8 before and after studies (described in table 1) and 29 case reports/series.
Table of experimental studies included in the review

{kind=link}
Flow chart showing numbers of studies included and excluded. CCT, controlled clinical trial; PICO, Population, Intervention, Comparator, Outcome; SR, systematic review.
The studies using non-vision based interventions for example, behavioural strategies and communication aids will be presented separately in another publication.
Interventions to improve distance vision
Spectacles
We found a CCT, a before/after study and a number of case reports describing the effects of prescribing distance spectacles for children with VND. The CCT11 involved four groups of children with VND with a variety of diagnoses attending specialist schools. Children needing spectacles for the first time or revision of their existing spectacles were given new spectacles either immediately, or after a 2-month delay during which the study was conducted. Observers (trained staff members) then noted whether any prespecified behaviours changed during the study. A number of visual behaviours such as making eye contact, accuracy of reaching behaviour and recognising simple pictures were described as being improved in the ‘given spectacles immediately’ group (n=73), but not in the delayed spectacles group (n=56) or in children with no need for glasses, some of whom had been given ‘placebo’ spectacles as a form of control. However the placebo group also improved in some measures such as recognising pictures and the observers were not masked as to the study group.
The before/after study12 used visual evoked potentials (VEPs) as the outcome. Improved (larger) VEP recordings were seen in 58/105 (55%) of children with their glasses on as compared with without their glasses while the rest did not show improved VEPs with their glasses.
Case reports13 ,14 also describe improved visual acuity and behaviour in children with VND with refractive errors once they have spectacles. Some patients who are intolerant of spectacles have been treated with excimer laser,15 ,16 laser assisted keratomileusis,17 phakic intraocular lenses18 and lensectomy±insertion of an intraocular lens,19 with some success although limited follow-up. Surgery has been reported as restoring or partially restoring previously observed levels of visual function for example, vitrectomy for funnel-shaped detachments20 and cataract surgery21 ,22 in children with Down syndrome and Lowe syndrome, respectively.
Vision training
Several studies reported the effects of training programmes as a means of improving visual acuity. A controlled study23 reported improved visual acuity (among other outcomes) after a year-long individualised programme providing practice in vision-based tasks. This was offered to 35 children with severe visual impairment and compared with a general developmental programme offered to a control group of 23 children with similar visual impairment. Only a subset of these children had VND: at recruitment 14 of the 58 children in the study had known additional neurodevelopmental disabilities. The median score for each outcome was better for children in the intervention group; better baseline acuity; normal developmental status (as compared with neurodevelopmental delay) and for children with specified diagnoses. Results are not quoted separately for the children with VND. However in analyses adjusted for all available predictors, being in the intervention group was still associated with better outcomes, which suggests indirectly that the children with VND shared some of the benefits of intervention. A before/after study24 compared Teller cards acuity, visual orienting and blink behaviour in 10 subjects with VND aged 9–21 years after an 8-week programme of being seated in front of progressively more complex black and white images, for 20 min per day, 4 days per week. Their performance with Teller card testing improved but there were no other changes in visual attention pattern or blink rate.
Three case series25–27 also report improved outcomes after individualised training programmes (n=9, 77 and 21, respectively). All were selected cases rather than consecutive and reported improvements over time with follow-up varying from 1 year to 20 years.
Other treatments for distance vision or general visual behaviour
Three case reports describe children with autism and very selective diets, who each presented with poor vision. This was subsequently improved by treatment with Vitamin A28 or Vitamin B12 supplements.29 ,30 We found three case series reporting less established treatments including acupuncture and stem cell implantation, with insufficient data to assess the results.31–,33
Summary of treatments to improve distance acuity
Overall there were consistent reports that distance acuity and related visual behaviour often improves, sometimes markedly, in some but not all children with VND given appropriate refractive correction. There are also some data suggesting that training programmes improve visual acuity in children with VND. However the evidence we found is either indirect,23 or based on selected case series so it is hard to know how many children may benefit. Improvements may not transfer from the trained function to more general visual behaviour,24 so more stringent evidence is needed to help guide whether vision training should be offered to some or all children with VND.
Interventions to improve near vision and/or accommodation
We found several studies investigating the use of glasses to improve near vision or accommodation. A CCT34 compared the effects of prescribing either bifocal spectacles or distance vision only spectacles, for children with Down syndrome whose accommodation was below published norms. Children with bifocals showed substantial improvements in their accommodation through the reading segment and to a lesser extent through the upper, distance viewing segment.
Two before/after studies also reported improvements in accommodation in children with Down syndrome who were given bifocals. One35 reported that all 40 children (with previous hypoaccommodation) accommodated better with their bifocals and 26/40 (65%) also demonstrated better accommodation through the distance part of the lens, implying improved active accommodation rather than just the passive optical enhancement of accuracy of near viewing. The other36 reported that all 11 children improved the accuracy of their accommodation through the bifocal segment but not through the upper segment of their glasses. Another before/after study37 reported that five children with cerebral palsy (CP) who had been given hyoscine patches to control their salivation had improved visual behaviour after the provision of spectacles designed to give clear focus at a distance of 1 m. In a case report38 the near acuity of two children with CP who were being treated with a hyoscine patch, improved dramatically when the patch was removed.
Summary of treatments to improve near acuity
Overall the evidence was consistent in suggesting that for children who hypoaccommodate, bifocal spectacles improve the accuracy of accommodation although there are conflicting results regarding whether there is also improvement when they look through the upper, non-reading part of the spectacles. These studies used careful and accurate measurements of accommodation at different distances to identify suitable subjects and it would be helpful to see results from settings using different methods to identify poor accommodators.
Interventions to improve ocular alignment
We found only case series describing results after horizontal muscle surgery in children with VND. In some reports, good results (within 10 prism dioptres of orthotropia) were obtained using conventional approaches to calculating the amount of muscle displacement required39 ,40; some however reported that fewer cases were overcorrected if surgical technique was modified and a reduced amount of muscle displacement used (compared with guidelines for typical children)41 Some, by contrast, found that using modified (reduced) surgery led to undercorrection.42 Botulinum toxin was reported as useful with equivalent success to some surgical case series.43 In one case series, horizontal muscle surgery for esotropia in children with Down syndrome also reduced previously unexplained abnormal head postures in these children.44 A series of 33 selected children with strabismus and CP reported no effect on strabismus from ‘vision therapy’ (the training programme) but a reduction in esotropic deviations in children who received surgery.45
Summary of interventions to improve ocular alignment
The reports indicate variable experience between centres of the results regarding horizontal muscle surgery in children with VND (particularly CP) and strabismus.
Interventions to improve control of pursuit or saccadic eye movements
Control of eye movements is often impaired in children with VND. Using a before/after design one group46 reported improved oculomotor control in 10 children with CP and poorly controlled eye movements, after a 6-week programme of individualised training exercises during which the children followed moving visuoacoustic targets with their head stabilised. Velocity and accuracy of smooth pursuit and saccadic movements were measured before and after the training programme using an objective photoelectric apparatus. Individual results were presented showing substantial improvements in smooth pursuit accuracy and velocity and decreases in saccadic latency were reported. Qualitative enhancements of performance were noted if subjects additionally used a hand or foot to follow the target. The specialist training programme described in the distance visual acuity section also reported better pursuit eye movements in the intervention group compared with the control group at the final assessment.23
Two studies have reported improved oculomotor control as a by-product of selective dorsal rhizotomy (SDR, a spinal operation) carried out to relieve spasticity in children with CP. A large case series47 described improved ocular alignment after SDR in 132/386 (34%) children with CP and strabismus. In another study three children with CP, abnormal eye movements and nystagmus had infrared video-oculography recordings pre SDR and post SDR.48 In two of the children eye movement control improved and nystagmus lessened while one remained unchanged. Finally a case report49 described reduced nystagmus with associated improvements in acuity and stereopsis, in a child with attention deficit hyperactivity disorder (ADHD), nystagmus and retinopathy, 1.5 h after they had taken their stimulant medication as compared with premedication. Performance returned back to premedication, baseline levels after a week of no further treatment.
Summary of interventions to improve eye movement control
We found evidence that training in pursuit and/or saccadic eye movement can lead to improved control and also that changes in central neurological inputs may also indirectly improve control, for example, after SDR surgery or with medication. Further evidence is needed as to which children may benefit and how long-lasting or transferable any functional improvements are.
Interventions to improve visuocognitive skills
Cognitive processing of visual input may be affected in a number of children with VND. We found only two studies reporting the effects of training specifically on cognitive aspects of vision in children with VND. In one single-case study50 a girl with acquired cerebral visual impairment and major motor deficits (after cardiopulmonary arrest) successfully regained the ability to identify targets by colour and shape after training with a set range of shapes/colours and using manual tracing with a black pen to reinforce the shapes being learned. After gradually removing the training strategies she retained the newly regained ability to name the coloured shapes accurately and could also accurately name black-and-white versions of the same shapes, but not other (untrained) shapes.
In another single-case study the authors investigated the effect of training in face recognition for a girl with severe prosopagnosia (face-blindness) after meningitis.51 Despite extensive practice no improvements were observed in her ability to recognise familiar or unfamiliar faces.
Summary of interventions to improve visuocognitive skills
These two reports illustrate that while training may improve some visuocognitive functions it may not improve others and more information is needed on how to better help children with VND with these difficulties.
Interventions to adapt the visual environment
We found two studies describing the use of ultraviolet (UV) light or blacklight to enhance visual characteristics of the environment. In a cross-over design trial involving four children with VND the authors reported that the use of a blacklight bulb enhanced the response to visual fixation training, as compared with a white-light bulb. All children were observed to engage in more fixations on the target when under the UV light as compared with the white, whichever light was used first.52
Similarly, in a study involving 13 severely affected children with VND, the outcomes of training in a shape-matching task (four shapes to be matched with four holes in a wooden board) were compared between seven children whose training programme was conducted using UV room lighting and UV-reflecting paint on the shapes, and another group of six similar children who were taught using the same equipment and materials, but in standard white-light room illumination. Final assessment for each group was in normal white-light illumination. Approximately half the children in each group couldn't achieve any part of the matching task at any time; of those who could achieve at least one match on one occasion, the children trained in UV light matched more shapes accurately than did the ones trained in white light.53
One study examined whether exposure to a multisensory environment (sensory room with equipment for vision and light stimulation) improved outcomes for children with VND. It reported an increased number of developmentally advanced behaviours in children after exposure to the multisensory environment as compared with baseline.54 By contrast, simplifying the visual environment was described in a case report55 as beneficial for a child whose reduced visual acuity, motor delay and dorsal visual stream impairment resulted in his having difficulties extracting information from cluttered visual scenes.
Summary of interventions to adapt the visual environment
We found some evidence that enhancing or adapting the visual characteristics of the environment can improve ability of children with VND to engage with tasks but more evidence is needed to determine how much modification, at what ages and how lasting the effects might be.
Discussion: quality of evidence and implications for practice
We have used the OCEBM levels as a guide to likely quality of evidence from the studies we found, where ‘1’ represents the likely strongest evidence and ‘5’ the likely weakest evidence. Table 1 demonstrates that although the studies using spectacles or UV paint were level ‘2’, many of the studies we found were level ‘3’ and all the case reports/series quoted would be level ‘4’. However many of the observational studies reported marked improvements, for example, with spectacles or in eye movements after training and these data may be regarded as stronger evidence than the study design might suggest—the OCEBM suggests level ‘2’ might be considered for observational studies with a dramatic effect. What is less clear from the available evidence is how generalisable many of the findings might be; whether improved vision skills result in improved general function and to what extent the bias introduced by having unmasked observers (and/or participants) will have possibly inflated the effect sizes described.
We acknowledge that there are limitations to this scoping review. In particular we note that we may have missed some potentially useful studies if they did not specifically include children with visual difficulties and neurodevelopmental problems, were not published in sources we could access or were described in conference proceedings or abstracts which were not identified by our search. However our criteria have produced a range of studies directly applicable to our target population. We also excluded studies not written in English for pragmatic reasons (no funds for translation). In addition there may be publication bias in the literature as we found few studies presenting negative findings.
In conclusion this review indicates where there are gaps in the evidence on interventions for children with VND. As is current practice, all children with VND should be assessed to determine whether spectacles for distance or near viewing could be offered and the use of hyoscine should be specifically enquired about. However, while training programmes and environmental modifications may help and could have profound implications for subsequent development, more evidence is needed on type of training or modification, optimum duration and age for training or exposure to modified environment and the degree to which improvements are lasting, transfer to other skills/activities or add to quality of life.
Acknowledgments
The authors thank Professor Gordon Dutton for his help in the work leading up to the review and his comments on a draft of the manuscript and Diana Hynam for her help with administration. This review is dedicated to Etienne Hicks and his family.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors CW devised, planned and wrote the paper with advice and support from all authors. KN shared the data retrieval and synthesis and cowrote the paper. MG and SH provided specific expertise on paediatric and developmental matters and cowrote the paper; SR and JR provided specific expertise regarding educational matters and cowrote the paper; JA provided specific help on occupational therapy matters and cowrote the paper; CB was the information specialist and devised and carried out searches with support from the team; JMW advised on data extraction and arbitrated to achieve consensus, helped design the study and cowrote the paper.
-
Funding CW is supported by a NIHR Career Development Fellowship CDF-2009-02-35.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.