Article Text

Abstract
Background/Aims To compare ophthalmic viscoelastic devices (OVDs) in protecting the cornea from endothelial cell loss during cataract surgery.
Methods A systematic review yielded 21 randomised controlled trials including 1769 patients. OVDs were classified according to the Arshinoff classification. Traditional pairwise meta-analyses were performed for each direct comparison. Mixed treatments comparisons (MTC) analysis was also performed to combine all direct and indirect comparisons. The outcome measure was loss in endothelial cell density 3 months after surgery.
Results Direct comparison meta-analysis showed that viscoadaptives lead to a lower loss in cell density compared with very low viscosity dispersives, and compared with super viscous cohesives. The soft shell technique, a combination of viscous cohesives and medium viscosity dispersives, showed a lower loss compared with viscous cohesives, but was not compared with the other treatments. The MTC analysis shows that comparing all treatment options together, all mean differences were ≤100 cells/mm2. The probability of being the best treatment option is 80% for viscoadaptives and 18% for the soft shell technique.
Conclusion Viscoadaptives may be superior to the other OVDs, but absolute differences in loss in endothelial cell density are <100 cells/mm2.
- Cataract surgery
- ophthalmic viscoelastic devices
- endothelial cell density
- cornea
- treatment medical
Statistics from Altmetric.com
Introduction
The corneal endothelium, the single cell layer lining the posterior surface of the cornea, has poor regenerative ability.1 Any direct trauma or injury to the endothelial cell layer results in a decrease in the number of cells and affects the ability of the endothelium to withstand further insult. But, even though the cell density may be low, the remaining endothelial cells are often capable of preventing corneal swelling until a critical threshold is reached, estimated at less than 500–1000 cells/mm2.2 When the endothelial cell density falls below this level, the cornea becomes oedematous and assumes the clinical appearance of bullous keratopathy, a serious complication that may occur following cataract surgery in up to 0.3% of patients.3 Such cases of bullous keratopathy are the third most common cause of penetrating keratoplasty,4 and are particularly common in patients with endothelial disease, such as Fuchs' endothelial dystrophy. Pseudophakic bullous keratopathy may occur many years after cataract surgery, because the normal rate of cell loss with age is accelerated after surgery. Studies indicate that long-term endothelial cell loss is influenced by the amount of surgical trauma.5 Therefore careful microsurgery with the use of protective ophthalmic viscosurgical devices (OVDs) is mandatory to minimise endothelial cell loss.6
A wide range of OVDs are available for surgeons to choose from, differing in their constituent components and in some cases in the concentration or chain length of these components. OVDs are classified according to the Arshinoff classification,7 which distinguishes two main properties of each OVD: viscosity and cohesion. Viscosity (more precisely zero-shear viscosity) is proportional to space creation and maintenance in surgery, whereas decreasing cohesion (or increasing dispersion) results in better coating of tissue and enhanced retention of the OVD in the eye during phacoemulsification,7 which makes them also more difficult to aspirate at the end of the procedure.
However, to date there are few data to support any one agent or type of OVD as being superior in terms of minimising endothelial cell loss following cataract surgery. The aim of this systematic review and meta-analysis was to synthesise all available evidence on the relative protective effect of the various OVDs and estimate more precisely which OVD is best at preserving endothelial cell density.
Methods
Literature search
The literature was searched systematically in the two major medical databases, Medline and Embase, from inception up until June 2007. The search terms used are listed in table 1. Randomised controlled trials (RCTs) evaluating the effect of OVDs on endothelial cell density in patients undergoing cataract surgery were eligible. All non-RCTs were excluded, as were studies in languages other than English, French, German or Dutch.
Search terms in Medline and Embase
All OVDs were classified according to the Arshinoff classification7: viscoadaptives, super viscosity cohesives, viscous cohesives, medium viscosity dispersives, very low viscosity dispersives, and the soft shell technique (a combination of viscous cohesives and medium viscosity dispersives). Studies using a not classifiable substance were excluded. Other exclusion criteria for the meta-analysis included: neither absolute nor relative change from baseline reported, studies presenting data on subgroups of patients only, studies comparing treatments from the same Arshinoff class, and studies without active comparator. This last criterion was used because the purpose of the meta-analysis was to compare the various OVDs in their protective effect on the endothelial cells, and the efficacy of OVDs compared with placebo treatment was not questioned.8 9
The selected articles were then critically appraised using an extended version of the Jadad scale10 available from the Dutch Cochrane Centre's website (http://dcc.cochrane.org). Subsequently, data were extracted in duplicate. Sample size was expressed in number of patients where available. The outcome was the absolute number of cells/mm2 lost 3 months after the cataract procedure, compared with the baseline density.
Handling of studies with poor data reporting
A set of three conventions to impute missing information were applied uniformly on all studies when appropriate, as recommended by the Cochrane Collaboration11 as follows. (1) When not available, the variance of the absolute number of cells/mm2 lost was calculated based on the available variances from the baseline and post-surgery densities, and assuming the average correlations from the other studies. (2) When not available, the number of patients post-surgery was assumed to be identical to the number of patients at baseline, ie assuming there was no loss to follow up. (3) When not available, baseline density was assumed to be identical to the average baseline density of all other studies selected in the analysis. These three conventions could influence the precision of the estimate (variance), but not the estimate itself (no bias introduced).
Meta-analysis of direct comparisons
Traditional pairwise meta-analyses were performed, one per each head-to-head comparison, using the weighted mean difference method for continuous outcomes.12 Because some comparisons showed heterogeneity in the study results, random effects models were preferred to the fixed effect model. All pairwise meta-analyses were performed using Review Manager version 4.2.13
We did not stratify our analyses according to cataract surgery type, as no significant difference in endothelial cell loss between extracapsular cataract extraction and phacoemulsification was identified in the Cochrane systematic review.14
Mixed treatment comparisons
Of the 15 possible pairwise comparisons with six treatments, only 11 were directly observed. Therefore, we performed a mixed treatments comparisons (MTC) analysis, which is a natural generalisation of the meta-analysis evidence structure,15 16 and combines all effects from direct and indirect comparisons to obtain estimates for all comparisons. It also allows ranking all treatment options by probability of being the most efficacious.
The choice between fixed effects and random effects model was based on a goodness-of-fit statistic (deviance information criterion (DIC)).17 Consistency of the evidence sources was assessed by calculating the posterior mean residual deviance for each individual treatment arm.
Sensitivity analyses were planned on mean baseline endothelial cell density of less than 1000 cells/mm2, as this is a relevant threshold clinically, and it can be hypothesised that the magnitude of the absolute change in endothelial cell density after cataract surgery depends on the baseline density. Another sensitivity analysis was planned excluding studies on patients with hard nucleus cataracts.
Graphical presentation of the network was based on the ‘diamond’ network proposed by Lumley.18 All MTC models were fitted with the WINBUGS (version 1.4.1) software.19
A difference of more than 100 cells/mm2 between two OVDs was considered a clinically relevant difference. We based this on the fact that corneal decompensation occurs at a density of below 500–1000 cells/mm2 and hence a difference of 10–20% in this value was considered likely to be clinically relevant. Similarly such a difference would account for a difference of 5% in a typical patient undergoing cataract surgery with a baseline endothelial cell density of 2000 cells/mm2.
Results
Search and selection process
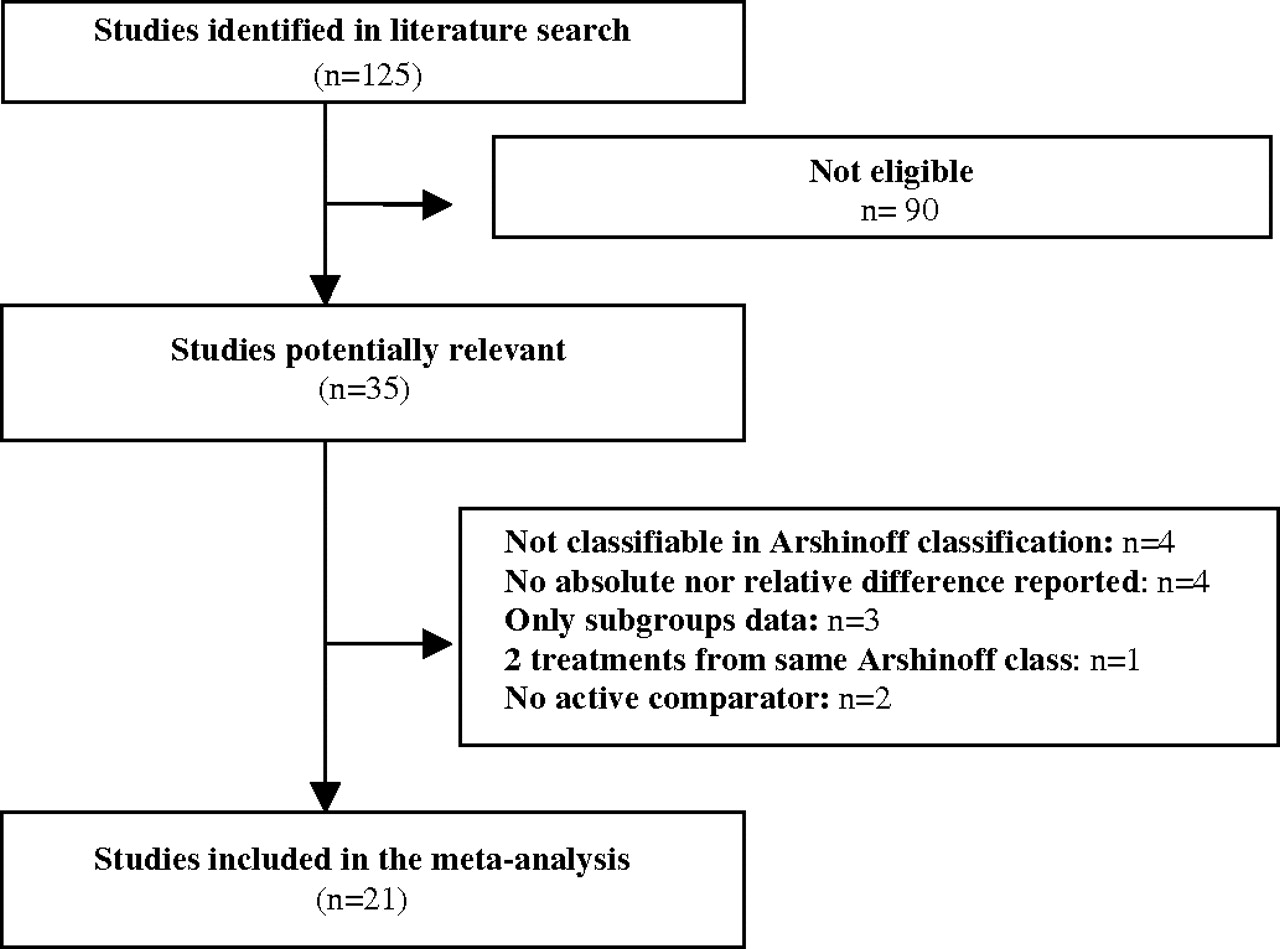
The search strategy yielded 125 articles, of which 35 were potentially relevant. Subsequently, four studies were excluded because they used a substance not classifiable in the Arshinoff classification and four studies because neither absolute nor relative change to baseline was reported. Three studies were excluded because only subgroups data were presented and one study because two treatments from the same Arshinoff class (but different commercial products) were compared with each other. Finally, two placebo-controlled studies were excluded. Because both studies compared placebo with the same comparator, ie viscous cohesives, they did not convey any additional information to the network of active comparisons.
This left 21 studies for inclusion in the meta-analysis, involving six treatment options.20–40 The selection process is presented in figure 1.

Flow chart of selection process.
Studies included
The results of the quality assessment are summarised in table 2. Two studies reported adequate concealment of allocation23 36 and two studies performed an intention-to-treat analysis.29 36 Blinding of the outcome assessors was stated in 14 of the 21 studies. Patients were excluded from the analyses because of intra-operative and postoperative complications in nine studies.22 27 32–36 38 39 Most studies recruited patients that were scheduled for routine cataract surgery. No study evaluated the OVDs specifically in patients with low baseline endothelial cell density; five studies excluded patients because of low baseline endothelial cell density.20 22 29 36 38 One study excluded patients in which the endothelial cell density varied by more than 10% between both eyes.34 One study included only patients with cornea guttata,34 and two studies included patients with hard nucleus cataracts.30 39 A description of each included study is presented in table 3.
Quality appraisal of included studies
Characteristics of included studies
The imputation conventions were applied on the following studies: compute variance of change from baseline,21 27 28 30 31 33–40 assume number of patients post surgery to be identical to number of patients at baseline,22 25 29 30 32 34–36 38–40 and impute the mean baseline value of all studies.31 37 In three other studies,24 25 28 data from two commercial products, but in the same Arshinoff class, were pooled.
The total number of patients included in all trials was 1769, with sample sizes ranging from 20 to 260 patients. In order to obtain statistical significance for a difference of 100 cells/mm2 between two treatment arms, at least 30 patients should be included in each arm assuming α=0.05, power=0.90, variance=250, and equal sample sizes in each group.41 Only 11 studies included 30 patients or more in each arm.
Baseline cell density varied from 1880 to 3085 cells/mm2, with a mean baseline density across all trials of 2385±299 cells/mm2. The mean loss in cell density 3 months after cataract surgery was 202±121 cells/mm2. The two studies that included patients with hard nucleus cataracts showed higher mean loss in endothelial cell density of 300–400 cells/mm2.30 39 Only four studies reported a significant difference between one or more OVDs, with conflicting results in two cases.38 33
Direct comparisons meta-analysis
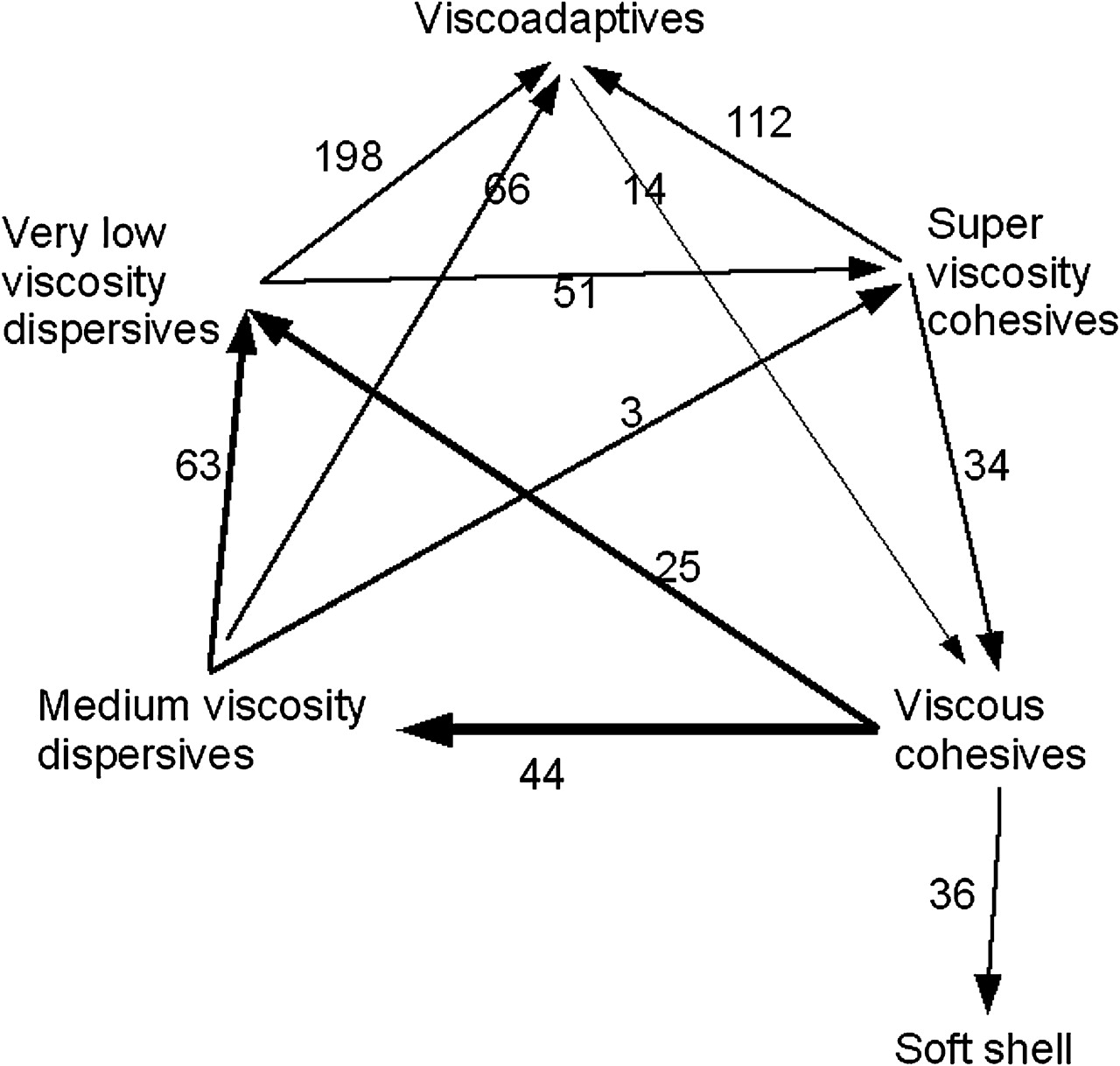
All results are presented in the upper triangle of table 4. Compared with very low viscosity dispersives, viscoadaptives lead to a lower loss in cell density of 198 (95% CI 99 to 298) cells/mm2, as shown by one single study.25 In addition, viscoadaptives lead to a lower cell loss of 112 (95% CI 14 to 211) cells/mm2 compared with super viscous cohesives, as shown by three studies.25 36 39 Compared with the other OVDs, no significant differences are identified. The soft shell technique, a combination of viscous cohesives and medium viscosity dispersives, shows a statistically significant lower loss compared with viscous cohesives of 36 (95% CI 3 to 69) cells/mm2. The soft shell was only compared with viscous cohesives, and hence no conclusion can be made with regard to the other comparisons.
Results from direct meta-analyses and results from mixed treatment comparisons
The data network (figure 2) shows that viscoadaptives have the most arrows pointing towards it, indicating potential superiority over the other options.

Graphical representation of the network, treatment effects estimated from direct comparisons. The width of a line is proportional to the number of studies involved in the head to head comparison. The arrows always point towards the best treatment of the comparison. So,  indicates that B is better than A, with a lower mean loss of cell density of 150 cells/mm2 with treatment B.
indicates that B is better than A, with a lower mean loss of cell density of 150 cells/mm2 with treatment B.
MTC analysis
The results of the MTC analysis are shown in the lower triangle of table 4. The estimates of the MTC are generally in accordance with the results from the direct comparisons and complement the lacking comparisons for the soft shell technique and the other treatments. The 95% credible intervals are narrower than for the direct estimates. This is because of the extra information provided by the indirect evidence. Importantly, all mean differences are ≤100 cells/mm2. However, some credible intervals exceed 100 cells/mm2, indicating that clinically significant differences between some treatments cannot be ruled out entirely.
Viscoadaptives have 80% chance to be the best treatment option, followed by the soft shell technique with 18%. The other treatments are almost never the best strategy. In figure 3, the difference of each treatment option compared with viscoadaptives is shown, illustrating that these differences are very small. It also shows that the comparison with the soft shell technique has the largest variability, as there is very little evidence linking this treatment to the rest of the network.

{kind=link}
{kind=link}
{kind=link}
Treatment effects versus viscoadaptives (and 95% credible interval): results from mixed treatment comparison.
Sensitivity analyses
The study by Storr-Paulsen et al38 compared a medium viscosity dispersive to a viscous cohesive and a very low viscosity dispersive. In this study, the two comparator OVDs showed a very large loss of cell density, almost double the cell loss reported in the other studies. These large losses in cell density, compared with a relatively normal loss for the medium viscosity dispersive, led to a highly significant result in favour of the medium viscosity dispersive. In the deviance analysis, this study was identified as an outlier. However, sensitivity analyses showed that the exclusion of this study did not change the results. Therefore the study was included in the analysis. Another planned sensitivity analysis excluding the two studies30 39 with hard nucleus cataracts showed results very similar to the main results (data not shown).
The planned sensitivity analyses based on baseline density were not possible, as no single study had a mean baseline density of less than 1000 cells/mm2.
Discussion
The results from this MTC including 1769 patients show that there are small differences of ≤100 cells/mm2 between the various OVDs in endothelial cell density loss 3 months after cataract surgery. These differences are not clinically relevant in most patients. Viscoadaptives and the soft shell technique have a probability of 80% and 18% respectively of being superior over the other OVDs. This probability should not be interpreted as the chance of adding benefit to a single patient, but rather as the number of times this option was the best in the simulations.
When the number of treatment options becomes large, a classic meta-analysis on all observed head to head comparisons has some drawbacks. First, with a large number of treatments, not all treatments are compared head to head, resulting in blanks in the evidence matrix. Second, this approach does not take all information into account. If one trial shows evidence of a treatment effect in a direct comparison, and five trials indirectly show no evidence of treatment effect, then this information should be accounted for somehow. Third, with a large number of treatments, the question is not so much how they compare with each other, but rather which one is the best. These three drawbacks of classic head-to-head meta-analysis are elegantly covered by MTC. In one global model, all direct and indirect evidence are combined to estimate all treatments effects, and, for each option, estimate the probability that it is the best among the set.42 43 The ‘price to pay’ is that an additional assumption needs to be made on the data: MTC requires that there is no confounding factor between the treatment effect and the treatments being compared. For instance, if older studies show a smaller treatment effect, and if two treatment options were only compared in older studies, time of study would be a confounding factor. This is not the case in our MTC, as all studies used comparable inclusion and exclusion criteria, except for the two studies including patients with hard nucleus cataracts. However, the sensitivity analysis in which these studies were excluded showed that the results and conclusions were robust to this exclusion. In addition, time of study and type of surgery are equally spread over the dataset.
The outcome that was chosen in this meta-analysis was the absolute loss in endothelial cell density 3 months after surgery, rather than the relative loss expressed as the % change from baseline. The latter outcome can be preferred if the amount of cell loss depends on baseline density. However, baseline density did not differ markedly between studies, we therefore preferred to use the outcome that has most face validity for clinicians.
It has been shown that the mean rate of endothelial cell loss even 2 years after surgery is significantly higher than the physiological rate, amounting to 0.9% per year.44 It is unclear, however, whether the OVD contributes to this decline independently from other risk factors such as the amount of surgical trauma and the type of intraocular lens.5 Endothelial cell density is to be considered as an intermediate for ultimate patient-oriented outcomes, such as corneal oedema, keratoplasty and vision. Four studies mentioned the proportion of patients suffering from postoperative corneal oedema and found no statistically significant differences; three others mentioned there were no significant differences in overall postoperative complications. However, from our data, it is not possible to make inferences about these patient-oriented outcomes, as the study was not designed for this outcome.
We did not identify a randomised trial specifically comparing OVDs in patients with very low endothelial cell density at baseline. The mean baseline density of all trials was 2385 cells/mm2, but there was no information on the proportion of patients with densities under 1000 cells/mm2. Hence this study does not provide direct evidence about whether or not a specific OVD is more favourable in patients with less than 1000 cells/mm2. A new RCT, including patients with a low baseline endothelial cell count would provide essential information for clinical practice. Nonetheless, most studies included patients regardless of their baseline endothelial cell density. In addition, one study compared OVDs in patients with cornea guttata and two studies recruited patients with hard nucleus cataracts prone to more severe loss in cell density. A direct comparison of viscoadaptives and soft shell would ‘close the loop’ of the MTC analysis as these two treatment options have not been compared directly.
When choosing an OVD, surgeons base their decision on whether they value the optimal endothelial coating properties of dispersive OVDs or the superior anterior chamber maintaining properties of viscoadaptive OVDs. Our results demonstrate that dispersive OVDs, ie medium viscosity dispersives and very low viscosity dispersives, do not protect the endothelial cornea more than the other OVDs. Hence it would appear that the equation traditionally followed by surgeons is flawed. Our study provides surgeons with an evidence base to refer to when making this decision, rather than depending on theoretical arguments. The next step would be to extend these results with a cost-effectiveness analysis, taking the costs of the OVD into account.
References
Footnotes
Funding This work has not been funded externally, and consequently there is no funding source that has been involved in this work.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance