Article Text

Abstract
Attention deficit/hyperactivity disorder (ADHD) may affect all aspects of a child’s life. Indeed, it impacts not only on the child, but also on parents and siblings, causing disturbances to family and marital functioning. The adverse effects of ADHD upon children and their families changes from the preschool years to primary school and adolescence, with varying aspects of the disorder being more prominent at different stages. ADHD may persist into adulthood causing disruptions to both professional and personal life. In addition, ADHD has been associated with increased healthcare costs for patients and their family members.
- CHQ, Child Health Questionnaire
- ODD, oppositional defiant disorder
Statistics from Altmetric.com
Attention deficit/hyperactivity disorder (ADHD) is a chronic, debilitating disorder which may impact upon many aspects of an individual’s life, including academic difficulties,1 social skills problems,2 and strained parent-child relationships.3 Whereas it was previously thought that children eventually outgrow ADHD, recent studies suggest that 30–60% of affected individuals continue to show significant symptoms of the disorder into adulthood.4 Children with the disorder are at greater risk for longer term negative outcomes, such as lower educational and employment attainment.5 A vital consideration in the effective treatment of ADHD is how the disorder affects the daily lives of children, young people, and their families. Indeed, it is not sufficient to merely consider ADHD symptoms during school hours—a thorough examination of the disorder should take into account the functioning and wellbeing of the entire family.
As children with ADHD get older, the way the disorder impacts upon them and their families changes (fig 1⇓). The core difficulties in executive function seen in ADHD7 result in a different picture in later life, depending upon the demands made on the individual by their environment. This varies with family and school resources, as well as with age, cognitive ability, and insight of the child or young person. An environment that is sensitive to the needs of an individual with ADHD and aware of the implications of the disorder is vital. Optimal medical and behavioural management is aimed at supporting the individual with ADHD and allowing them to achieve their full potential while minimising adverse effects on themselves and society as a whole.

Stages of ADHD. Adapted from Kewley G (1999).6
The aim of this paper is to follow the natural history of this complex disorder through preschool years, school life, and adulthood and to consider its effect on the family, the community, and society as a whole. In addition, comorbidities and healthcare costs are examined.
THE PRESCHOOL CHILD
Poor concentration, high levels of activity, and impulsiveness are frequent characteristics of normal preschool children. Consequently, a high level of supervision is the norm. Even so, children with ADHD may still stand out. In this age group there is often unusually poor intensity of play and excessive motor restlessness.8,9 Associated difficulties, such as delayed development, oppositional behaviour, and poor social skills, may also be present. If ADHD is a possibility, it is vital to offer targeted parenting advice and support. Even at this early stage parental stress may be huge when a child does not respond to ordinary parental requests and behavioural advice.9 Targeted work with preschool children and their carers has been shown to be effective in improving parent child interaction and reducing parental stress.10,11 A useful review of the available evidence and methods is provided by Barkley.12
PRIMARY SCHOOL YEARS
The primary school child with ADHD frequently begins to be seen as being different as classmates start to develop the skills and maturity that enable them to learn successfully in school. Although a sensitive teacher may be able to adapt the classroom to allow an able child with ADHD to succeed, more frequently the child experiences academic failure, rejection by peers, and low self esteem (fig 2⇓). Comorbid problems, such as specific learning difficulties, may also start to impact on the child, further complicating diagnosis and management. Assessment by an educational psychologist may help to unravel learning strengths and difficulties, and advise on necessary support in the classroom.

Frequently, difficulties at home or on outings with carers (for example, when shopping, out in the park, or visiting other family members) also become more apparent at this age. Parents may find that family members refuse to care for the child, and that other children do not invite them to parties or out to play. Many children with ADHD have very poor sleep patterns, and although they appear not to need much sleep, daytime behaviour is often worse when sleep is badly affected. As a result, parents have little time to themselves; whenever the child is awake they have to be watching them. Not surprisingly, family relationships may be severely strained, and in some cases break down, bringing additional social and financial difficulties.14 This may cause children to feel sad or even show oppositional or aggressive behaviour.
Assessing the quality of life of the child suffering from ADHD is difficult. Behavioural assessments are usually carried out by parents, teachers, or healthcare professionals, and it can usually only be inferred how the child must feel. However, data from self evaluations indicate that children with ADHD view their most problematic behaviour as less within their control and more prevalent than children without ADHD.15 Participation in a school based, nurse led support group was associated with an increase in self worth in pre-adolescents with ADHD.16
Johnston and Mash reviewed the evidence of the effect of having a child with ADHD on family functioning.14 They concluded that the presence of a child with ADHD results in increased likelihood of disturbances to family and marital functioning, disrupted parent-child relationships, reduced parenting efficacy, and increased levels of parent stress, particularly when ADHD is comorbid with conduct problems.
In a survey of the mothers and fathers of 66 children, parents of children with ADHD combined and inattentive subtypes expressed more role dissatisfaction than parents of control children.17 Furthermore, ADHD in children was reported to predict depression in mothers.18 Pelham et al reported that the deviant child behaviours that represent major chronic interpersonal stressors for parents of ADHD children are associated with increased parental alcohol consumption.19
Limited attention has been given to sibling relationships in families with ADHD children. While it has been reported that siblings of children with ADHD are at increased risk for conduct and emotional disorders,20 a more recent study presenting sibling accounts of ADHD identified disruption caused by symptoms and behavioural manifestations of ADHD as the most significant problem.21 This disruption was experienced by siblings in three primary ways: victimisation, caretaking, and sorrow and loss. Siblings reported feeling victimised by aggressive acts from their ADHD brothers through overt acts of physical violence, verbal aggression, and manipulation and control. In addition, siblings reported that parents expected them to care for and protect their ADHD brothers because of the social and emotional immaturity associated with ADHD. Furthermore, as a result of the ADHD symptoms and consequent disruption, many siblings described feeling anxious, worried, and sad.21
Broader social and family functioning has been assessed using the Child Health Questionnaire (CHQ), a parent rated health outcome scale that measures physical and psychosocial wellbeing.22–,24 The studies demonstrated that treatment of ADHD with atomoxetine, a new non-stimulant medication for ADHD, resulted in improved perception of quality of life, with improvements being apparent in social and family functioning, and self esteem. Further research assessing the ongoing quality of life for the child and their family following multimodal input is urgently needed.
ADHD IN YOUNG PEOPLE
Adolescence may bring about a reduction in the overactivity that is often so striking in younger children, but inattention, impulsiveness, and inner restlessness remain major difficulties. A distorted sense of self and a disruption of the normal development of self has been reported by adolescents with ADHD.25 Furthermore, excessively aggressive and antisocial behaviour may develop, adding further problems (fig 3⇓). A study by Edwards et al27 examined teenagers with ADHD and oppositional defiant disorder (ODD), which is defined by the presence of markedly defiant, disobedient, provocative behaviour and by the absence of more severe dissocial or aggressive acts that violate the law or the rights of others. These teenagers rated themselves as having more parent-teen conflict than did community controls. Increased parent-teen conflict was also reported when parents of teenagers with ADHD carried out the rating exercise. In addition, a survey of 11–15 year olds showed that those with hyperkinesis were twice as likely as the overall population to have “a severe lack of friendship”.28

Antisocial behaviour in adolescents with ADHD.26 Data primarily represents outcomes in those with conduct disorder as teenagers.
Young people with ADHD are at increased risk of academic failure, dropping out of school or college, teenage pregnancy, and criminal behaviour (fig 4A⇓ and B). Driving poses an additional risk. Individuals with ADHD are easily distracted from concentrating on driving when going slowly, but while driving fast may also be dangerous. It has been shown that, compared with age matched controls, drivers with ADHD are at increased risk of traffic violations, especially speeding, and are considered to be at fault in more traffic accidents, including fatal ones (fig 5⇓).30 The risk of such events was increased further by the presence of concomitant ODD.29 However, it has been suggested that treatment may have a positive effect on driving skills.31
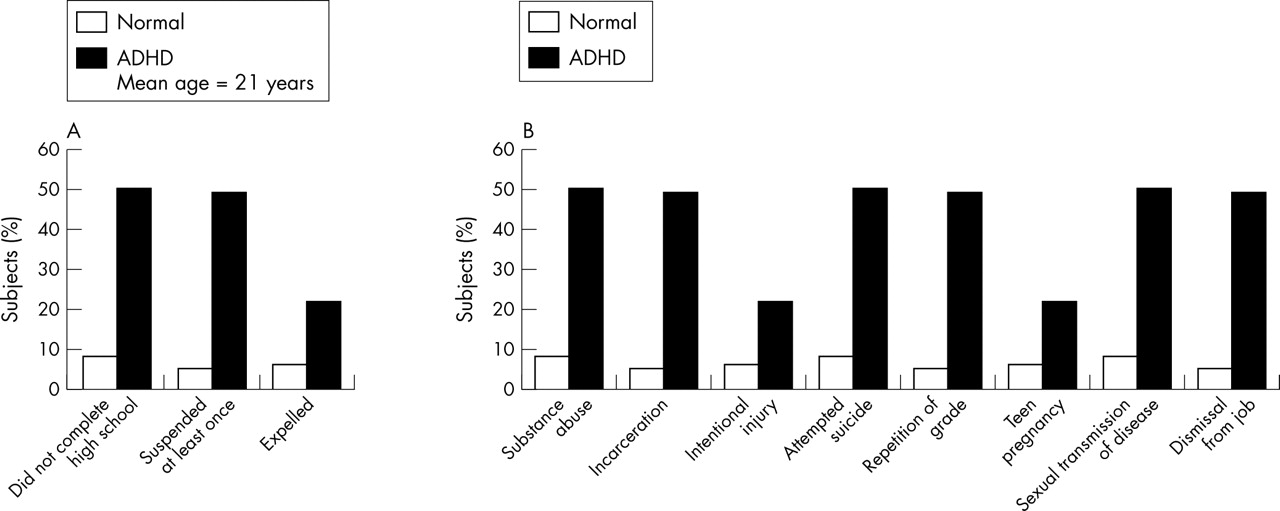
Impact of ADHD in adolescence. Data from Barkley RA;26 (A) Impact at school; (B) impact on health, social, and psychiatric wellbeing.

Driving-related offences in young adults with ADHD and controls. NS, not significant. Data from Barkley RA et al.29
ADULT LIFE
As many as 60% of individuals with ADHD symptoms in childhood continue to have difficulties in adult life.32,33 Adults with ADHD are more likely to be dismissed from employment and have often tried a number of jobs before being able to find one at which they can succeed.5 They may need to choose specific types of work and are frequently self employed. In the workplace, adults with ADHD experience more interpersonal difficulties with employers and colleagues. Further problems are caused by lateness, absenteeism, excessive errors, and an inability to accomplish expected workloads. At home, relationship difficulties and break-ups are more common. The risk of drug and substance abuse is significantly increased in adults with persisting ADHD symptoms who have not been receiving medication.34 The genetic aspects of ADHD mean that adults with ADHD are more likely to have children with ADHD. This in turn causes further problems, especially as the success of parenting programmes for parents of children with ADHD is highly influenced by the presence of parental ADHD.35 Thus, ADHD in parents and children can lead to a cycle of difficulties.
COMORBIDITIES
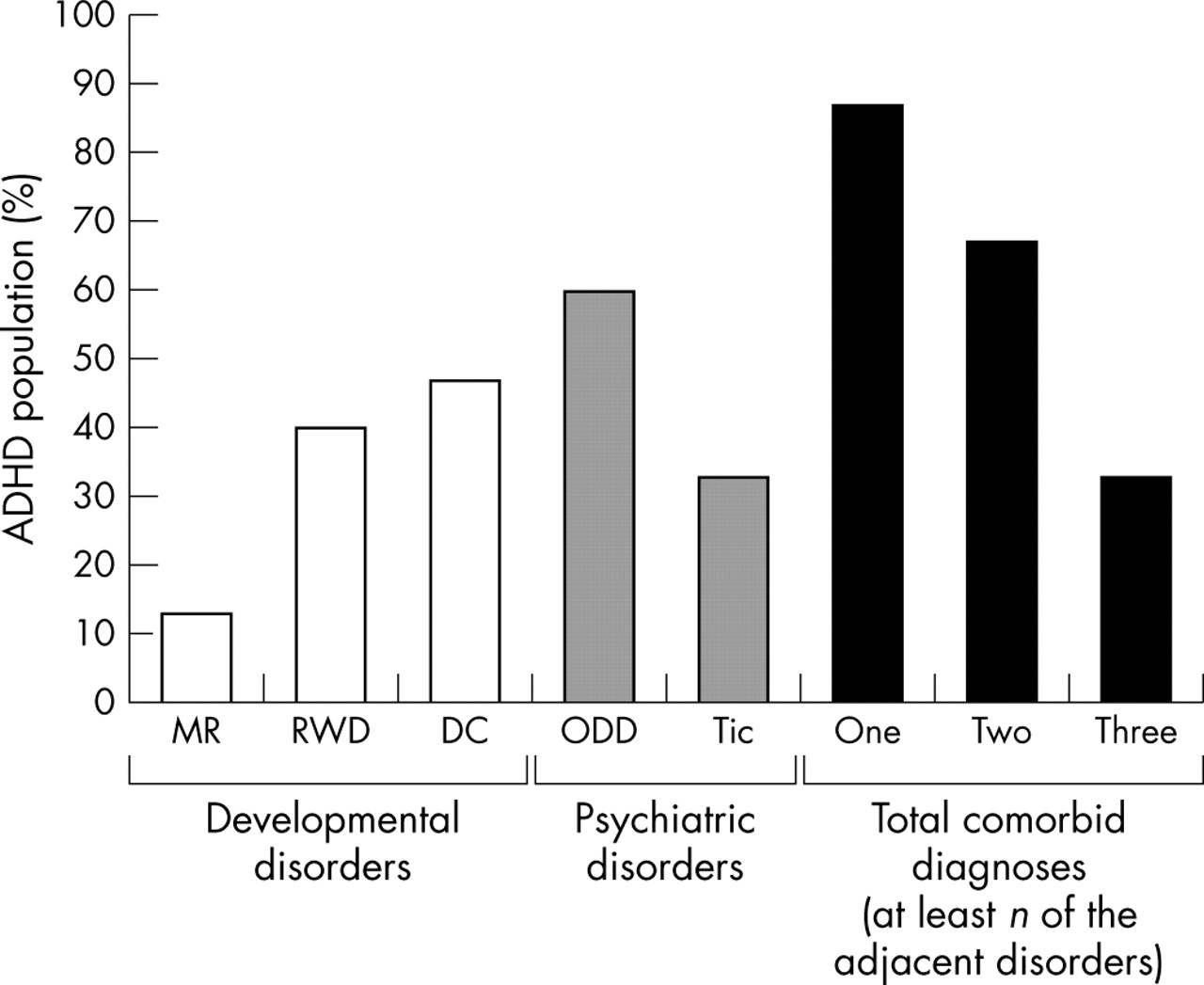
Comorbid disorders may impact on individuals with ADHD throughout their lives. It is estimated that at least 65% of children with ADHD have one or more comorbid conditions.36 The reported incidence of some of the most frequent comorbidities is shown in figure 6⇓, with neurodevelopmental problems, such as dyslexia and developmental coordination disorder, being particularly common. Many children with ADHD also suffer from tic disorders (not related to stimulant medication). In addition, around 60% of children with Tourette’s Syndrome fulfil criteria for ADHD,38,39 and autistic spectrum disorder is increasingly recognised with comorbid ADHD.39 Initially, excessive hyperactivity may mask the features of autistic spectrum disorder until the child receives medication. Conduct disorder and ODD coexist with ADHD in at least 30%, and in some reports up to 90%, of cases.36 These most frequently occurring comorbidities can, however, be considered more as complications of ADHD, with adversity in their psychological environment possibly determining whether children at risk make the transition to antisocial conduct.40
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
ADHD and comorbidity in Swedish school age children.37 MR, mental retardation; RWD, reading/writing disorder; DC, developmental coordination; ODD, oppositional defiant disorder.
PROBLEMS ASSOCIATED WITH TREATMENT
Growth deficits in children receiving stimulant treatment for ADHD have long been the subject of scientific discussion. Conflicting results have been reported with some authors indicating that stimulants do indeed affect growth in children,41–,43 but that this only occurs during active treatment phase and does not compromise final height.44 Other studies, however, have not found any evidence to suggest that stimulants influence growth.45,46 Taken together, the results suggest that clinicians should monitor the growth of hyperactive children receiving stimulants, and consider dose reduction in individual cases should evidence of growth suppression occur.
Another frequently quoted concern about treatment of ADHD with stimulant medications is that it could lead to drug addiction in later life. Young people with ADHD are by nature impulsive risk takers, and there is clear evidence that untreated ADHD—especially with concomitant conduct disorder—is associated with a three- to fourfold increase in the risk of substance misuse.47,48 In contrast, patients medicated with stimulants have a similar risk of substance misuse to controls.49 These data therefore provide strong evidence in favour of careful treatment and support for young people with ADHD.
HEALTHCARE COSTS
Healthcare costs for individuals with ADHD in the UK have not been fully estimated, but evidence from the USA suggests that they are increased compared with age matched controls. A population based, historical cohort study followed 4880 individuals from 1987 to 1995 and compared the nine year median medical cost per person: ADHD medical costs were US$4306, whereas non-ADHD medical costs were US$1944 (p<0.01).50 These findings are likely to reflect increased injury following accidents and a rise in use of substance abuse services and other outpatient facilities, although poor ability to comply with advice on medication (for example, asthma management) may also be implicated. A study of the injuries to children with ADHD established that children with ADHD were more likely to be injured as pedestrians or bicyclists than children not suffering from ADHD. They were more likely to sustain injuries to multiple body regions, head injuries, and to be severely injured.51 ADHD has been found to represent a risk factor for substance abuse,47,52 and an investigation of prevalence of ADHD among substance abusers has established that ADHD was significantly overrepresented among inpatients with psychoactive substance use disorder.53 Increased use of health services is also seen in the relatives of individuals with ADHD. A study has shown that direct and indirect medical costs were twice as high as those of family members of a control group.54 The difference in these costs was primarily due to a higher incidence of mental health problems in the family members of ADHD patients, which reflects the increased stresses and demands of living with an adult or child with ADHD. Indeed, ADHD related family stress has been linked to increased risk of parental depression and alcohol related disorders.55–,57
It is vital to consider the role of treatment of ADHD in decreasing the individual’s risk of adverse outcomes. A number of studies on the effect of treatment of ADHD on the risk of substance abuse encouragingly demonstrate a fall in risk to that of the normal population.58–,60
CONCLUSION
Mannuzza’s review of the long term prognosis in ADHD concludes that childhood ADHD does not preclude high educational and vocational achievements (for example, Master’s degree or medical qualification).61 However, ADHD is a disorder that may affect all aspects of a child’s life. Careful assessment is paramount, and if this demonstrates significant impairment as a result of ADHD, there is clear evidence that treatment of ADHD should be instituted.62,63 Current treatment focuses mainly on the short term relief of core symptoms, mainly during the school day. This means that important times of the day, such as early mornings before school and evening to bedtime, are frequently unaffected by current treatment regimes. This can negatively impact on child and family functioning and fail to optimise self esteem and long term mental health development.
In 2003, the American Academy of Pediatrics recommended that clinicians should work with children and their families to monitor the success (or failure) of treatment, using certain criteria to assess specific areas of difficulty and quality of life as a whole.64 There has been a reluctance in the UK to treat ADHD with medication, fuelled by concerns about possible over-prescription in the USA. In addition, newspaper and media coverage of ADHD is often negative and stigmatising. The evidence of potentially severe difficulties for the child, the family, and, in some cases, for society as a whole, means that coordinated multi-agency effort to support the child and family is essential. Moreover, healthcare professionals have an important role in providing balanced and supportive information about ADHD and meeting the needs of affected individuals and their families.
REFERENCES
Linked Articles
- Editorial