Article Text

Abstract
Objective: Public health surveillance of physical activity in children in the UK depends on a parent-reported physical activity questionnaire which has not been validated. We aimed to validate this questionnaire against measurement of physical activity using accelerometry in 6–7-year-old children.
Methods: In 130 children aged 6–7 years (64 boys, 66 girls) we estimated habitual moderate–vigorous intensity physical activity (MVPA) using the Health Survey for England parent-report questionnaire for physical activity. For the same time period and the same children, we measured MVPA objectively using 7-day accelerometry with the Actigraph accelerometer.
Results: The questionnaire over-estimated MVPA significantly (paired t test, p<0.01). Mean error (bias) when using the questionnaire was 122 min/day (95% CI 124 to 169). Mean time spent in MVPA was 146 min/day (95% CI 124 to 169) using the questionnaire and 24 min/day (95% CI 22 to 26) using the accelerometer. Rank order correlations between MVPA measured by accelerometer and estimated by the questionnaire were not statistically significant.
Conclusions: Public health surveillance of physical activity should not rely on this questionnaire. Levels of habitual physical activity in children are likely to be substantially lower than those reported in UK health surveys.
Statistics from Altmetric.com
There is increasing awareness of the importance of physical activity to short and long term health in children, with evidence that children should accumulate at least 60 min of moderate–vigorous intensity physical activity (MVPA) daily.1–3 In the UK, as in many other countries, population surveillance of physical activity is carried out by regular national surveys which use subjective methods of quantifying physical activity among children and adolescents (questionnaires completed by parents).4 5 The Health Survey for England4 and the Scottish Health Survey5 have used the same questionnaire to generate estimates of habitual MVPA which are the foundation of much research, for example health survey data are used widely to test relationships between MVPA and health.4 5 Health survey data on population physical activity underlie much of our public health policy and practice.2 3 6 Estimates of children’s MVPA from these national surveys are used to monitor secular trends, to assess the extent of adherence to the recommendation that children should accumulate ⩾60 min of MVPA per day, and to assess performance in relation to public health targets for increases in population MVPA.2 3
The UK health surveys suggest a very physically active population and have reported modest increases in MVPA among British children in recent years.4 5 In the most recent Scottish Health Survey (2003) for example, >75% of 6–10 year-old boys and >70% of 6–10-year-old girls were reported to achieve >60 min of MVPA per day every day,5 with very similar estimates from English children.2 These UK survey data, suggesting relatively high levels of habitual MVPA, are inconsistent with a wide variety of other recent evidence from UK children, which indicate low levels of energy expended on physical activity as shown by measurements with doubly-labelled water,7 population-wide increases in waist circumference,8 body mass index and body fatness,9 and trends in proxies for physical activity such as walking to school and transport by car.10 11 The UK health survey data are also inconsistent with recent studies in which much lower measures of MVPA in British children have been obtained using validated objective methods based on accelerometry (ie, motion sensing).7 12 13 However, levels of habitual physical activity have not yet been measured in the same children and at the same time with both accelerometry and the parent-report questionnaire used in the national health surveys.
In contrast to accelerometry, the questionnaires used in national surveys have not been validated for measurement of MVPA,10 14 and have been described as providing very crude estimates of the amount of MVPA.10 11 The aim of the present study was therefore to validate the Health Survey for England Physical Activity Questionnaire against objective measurements of habitual physical activity by accelerometry in the same children at the same time, as part of a cohort study, the Gateshead Millennium Study15 (www.ncl.ac.uk/gms).
METHODS
Participants
Families who participated in the present study did so during 2006–2007 as part of the Gateshead Millennium Study,15 a birth cohort study of infants born between June 1999 and May 2000 being followed up in 2006–2007. Ethics approval for the study was obtained from the Gateshead Primary Care Trust Local Research Ethics Committee, and parents provided informed consent to participation; children assented to participation.
Design
The present study was designed to provide a subjective estimate of habitual physical activity using the Health Survey for England Physical Activity Questionnaire and, for the same time period for the same child, to provide an objective measure of habitual physical activity using accelerometry with the CSA/MTI Actigraph (Medical Technologies International, Fort Walton Beach, FL). The Health Survey for England Physical Activity Questionnaire aims to assess the habitual level of MVPA but is based on parental reports which do not include physical activities undertaken at school, and assumes that all physical activities which are reported are MVPA.
Physical activities which constitute MVPA occur at energy expenditures which are at least three times the energy expended at rest for the individual child, and would typically include brisk walking, running and more intense forms of physically active play usually undertaken outdoors. The accelerometry method measures all movements undertaken during the waking hours, and a cut-off applied to the output from the Actigraph accelerometer, usually expressed as a count per minute (cpm), is used to define the intensity of movement, including amount of time spent in MVPA.16 Four paediatric studies have now been published which have attempted to “calibrate” accelerometer output for measurement of MVPA, and all have suggested that the appropriate cut-off to define MVPA for the Actigraph is in the range 3100–3600 cpm.17–20 These studies and a recent review also found that this cut-off is applicable across a wide age range and can be applied to both boys and girls.16–20
A large body of high quality and consistent evidence has accumulated in support of accelerometry for measuring the amount of physical activity undertaken by free-living children and this has been reviewed recently.16 21–25 A recent systematic review concluded that many supportive validations of the Actigraph (against energy expenditure and direct observation of movement, ie, the two “gold standards” for measurement of physical activity) have now been published and that it has low reactivity and high reliability.25 We therefore considered it appropriate to validate the questionnaire against accelerometry in the present study: differences between levels of MVPA derived from the questionnaire and the accelerometer in the present study could be interpreted with confidence as errors in the quantification of MVPA by the questionnaire.
Subjective estimation of physical activity by questionnaire
The questionnaire was directed at parents and was used exactly as described in the Health Surveys for England4 and Scottish Health Surveys.5 In brief, parents were asked to complete a series of questions on their child’s walking, sports, organised/structured activities and physically active play during the past week. Physical activity undertaken during school hours is not considered by the questionnaire, presumably since the questionnaire depends on parent reports only. Data from completed questionnaires were double-entered by a specialised data entry service. The algorithm used by the English and Scottish Health Surveys was used to convert parental responses to minutes of MVPA per day, and this was also carried out twice for each participant to minimise errors in data entry.
Objective measurements of physical activity by accelerometry
Participating children were asked to wear the Actigraph 7164 accelerometers on a waist belt for 7 consecutive days, during waking hours, as previously described.7 26–28 Parents were asked to supervise and help children put the Actigraphs on in the morning and remove them before going to bed, and to record on a brief log sheet when they were removed at other times (eg, when showering). At the end of the 7-day recording period, families returned the Actigraphs and log sheets for data analysis and manual processing. Manual processing aimed to identify periods when the accelerometers did not record any movement as indicated by consecutive zeros in the accelerometry record, and to assess if these were missing data (times when the accelerometers were not being worn, which were addressed with reference to the parental log sheet in most cases and by a telephone call to parents in a minority of families) or zeros which arose from instrument malfunction. In practice, such long periods of successive zeros were rare and were usually easily addressed by manually editing the accelerometry records with reference to the log sheets. Compliance with accelerometry was very good.
Seven days of accelerometry provides high precision in physical activity measurement and is regarded widely as the optimum length of time for measuring habitual physical activity in children.16 29 Penpraze et al found that the reliability of 7 days of accelerometry, at 10 h per day, was 80%.27
In order to convert accelerometry output to levels of MVPA, we used the previously validated cut-off point of 3200 cpm,17 as described previously.7 17–19 As noted above, a large and consistent body of evidence from published paediatric studies suggests that a cut-point in Actigraph accelerometry output between 3100 and 3600 cpm identifies MVPA with high diagnostic accuracy.16–20
Statistical analysis and power
We compared estimates of MVPA from the questionnaire with measures of MVPA from accelerometry in three ways. First, we used Bland-Altman analysis30 to determine the biases and limits of agreement between the two methods for the absolute amount of MVPA, as estimated by the questionnaire and measured by the accelerometer. Second, in order to test the statistical significance of differences in the absolute amount of MVPA between the two methods, paired t tests were used, it having first been determined that the differences between the two methods were normally distributed. These first two forms of analysis were intended to assess the ability of the self-report questionnaire to quantify absolute amounts of MVPA. Since physical activity questionnaires can be of value in the assessment of the relative amount of physical activity undertaken (for example to rank individuals as high-, medium- or low-active), the ability of the physical activity questionnaire to determine the relative amount of MVPA was determined using Spearman’s rank correlations between measures of MVPA obtained by the questionnaire and by the accelerometer.
The magnitude of the differences in MVPA between the two methods (accelerometry and questionnaire) was difficult to determine at the beginning of the present study, although we suspected that large differences might exist on the basis of the inconsistencies between studies which have used different methods in the literature described above.
RESULTS
Data collected and characteristics of study participants
We collected paired data (7-day accelerometry and physical activity questionnaires) from 149 children. Data from 19 children were excluded because of missing accelerometry data (less than 7 days) or missing questionnaire data, or because the child was reported as being ill at the time of the study (since this would not reflect habitual physical activity), leaving a sample of 130 (64 boys, 66 girls; healthy and almost all Caucasian) for analysis. Although power was limited, we found no significant difference between the 19 children with data excluded and those with data included for level of MVPA as measured by the accelerometer. Mean number of accelerometer hours per day was 11.1 (SD 1.1). The characteristics of study participants are described in table 1.
Validation of Health Survey for England Physical Activity Questionnaire: absolute amount of MVPA
In boys (n = 64), the mean difference (bias30) between the questionnaire and the accelerometer in MVPA was +127 min/day (95% CI +91 to +163). The difference in MVPA between the two methods was statistically significant (paired t test, p<0.001). The limits of agreement30 were −163 to +417 min/day.
In girls (n = 66), the mean difference (bias) between the questionnaire and the accelerometer in MVPA was +118 min/day (95% CI +91 to +144), and the difference in MVPA between the two methods was statistically significant (paired t test, p<0.001). The limits of agreement were −97 to +332 min/day.
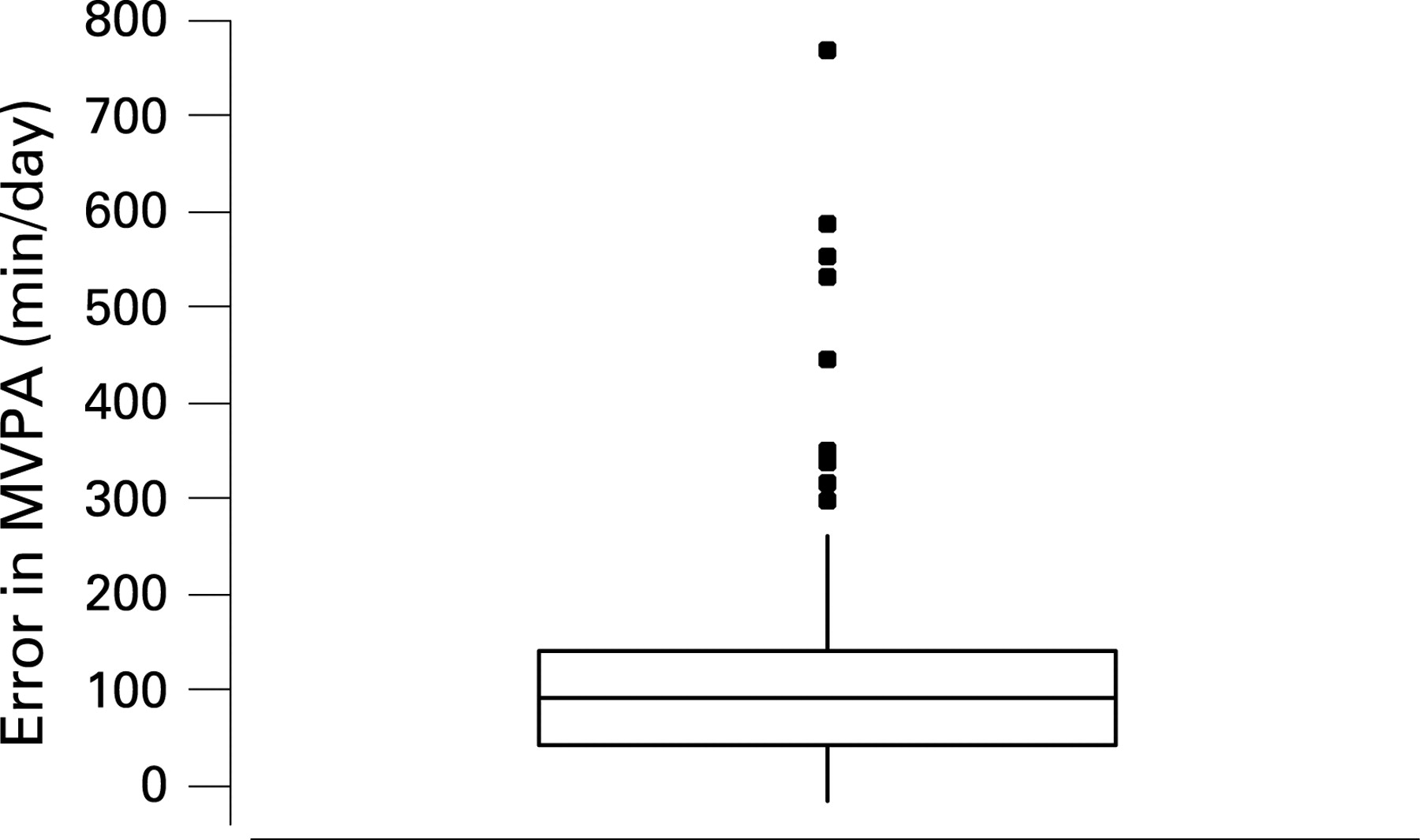
With no evidence of differences in the validity of the questionnaire between the sexes, data from both sexes were combined (n = 130). The mean difference (bias) between the questionnaire and the accelerometer in MVPA was +122 min/day (95% CI +100 to +144), with limits of agreement of −131 to +376 min/day. Figure 1 summarises errors in the estimation of MVPA using the questionnaire.

{kind=link}
Using the physical activity questionnaire data, 83% (53/64) of boys and 56% (37/66) of girls in the sample met the public health recommendation of accumulating 60 min of MVPA every day. In contrast, using the accelerometry data, only 3% (2/64) of boys and 2% (1/66) of girls in the sample accumulated 60 min of MVPA every day in the present study.
Validation of Health Survey for England Physical Activity Questionnaire: relative assessment of MVPA
Rank order correlations between MVPA as measured by accelerometry and estimated by questionnaire were low and non-significant in both sexes: r = 0.15 (p = 0.22) in boys; r = 0.10 (p = 0.14) in girls. With data from both sexes combined, the rank order correlation was low (r = 0.16) but almost reached statistical significance (p = 0.07).
DISCUSSION
Main findings and interpretation, and consistency with other evidence
The present study is the first to validate the questionnaire used for the public health surveillance of physical activity in children in the UK against an objective method of measuring physical activity. The objective method used in the present study, accelerometry, has been validated repeatedly in children, and the evidence on validity and reliability has been reviewed and critically appraised.16 21–25 It is therefore reasonable to conclude that differences in the results obtained by the questionnaire and the accelerometer in the present study are the result of errors in the questionnaire. In the present study, the levels of habitual MVPA of participating children were very low, and the questionnaire substantially overestimated physical activity, with a statistically and biologically significant bias in MVPA of around 2 h per day.
Our observations of low levels of habitual MVPA from accelerometry are consistent with recent studies in UK children which have also used accelerometry.7 12–14 In a representative sample of 3–6-year-old children in Glasgow, Scotland and in 11–12-year-old participants in the Avon Longitudinal Study of Parents and Children in England, median MVPA was <30 min/day; in these studies only a small minority of children and adolescents achieved 60 min of MVPA (as measured by accelerometry) every day.7 12 13 Our observation that low levels of MVPA are the norm is also consistent with trends in proxies for physical activity in British youth (eg, national statistics on the decline in walking and increases in car use),9 10 consistent with a study which used doubly-labelled water measures of physical activity energy expenditure in Scottish 3–7-year-old children,7 and consistent with recent population-wide secular trends in body fatness and fat distribution in British children.9 Taken together with evidence on the high validity of Actigraph accelerometry (noted above and reviewed repeatedly),16 relatively low levels of habitual MVPA in British children are more plausible than the relatively high levels of MVPA reported by English and Scottish Health Surveys.
What is already known on this topic
-
UK surveillance of children’s physical activity depends on a questionnaire to estimate levels of physical activity; this questionnaire has not been validated.
-
UK surveillance surveys report relatively high levels of physical activity in children.
What this study adds
-
The UK physical activity questionnaire substantially overestimates levels of physical activity in children.
-
Public health surveillance of physical activity levels in children should not rely on the current questionnaire.
Sources of error in the questionnaire
A detailed discussion of the reasons for the overestimation of MVPA by the Health Survey for England questionnaire would go beyond the scope of the present report. However, subjective methods measure perceptions of physical activity rather than physical activity per se, and a degree of overestimation of children’s physical activity by parents seems likely.9 16 Some aspects of the Health Survey for England Physical Activity Questionnaire may overestimate physical activity, but other aspects should underestimate physical activity, and these errors must offset each other to some degree. For example, the questionnaire algorithm assumes that all physical activity reported by parents is of moderate intensity or above (which must overestimate the amount of MVPA recorded), but any overestimate arising from this assumption may be offset by the fact that the questionnaire specifically excludes physical activity undertaken during the school day which parents are not asked to report on.
Study implications
Other authors have noted the dearth of good (ie, quantitative) population surveillance data on physical activity in youth,10 11 31 and have noted that the methodology used in the national surveys in the UK is crude and not supported by validation against objective methods.10 These authors have suggested that simple subjective methods of the kind used in UK surveys at present might be inadequate to identify relationships between physical activity and health, and may be inadequate to examine trends in physical activity over time with any confidence,10 11 31 32 but no previous study has tested the validity of these methods for assessing relative and absolute amounts of MVPA in children. We also note that recent studies which have used accelerometry to measure physical activity have generally been more successful in elucidating relationships between physical activity and health in children,12 33 in part because of their improved measurement of the amount of physical activity being undertaken.
The present study is unsupportive of current methodology for population surveillance of physical activity of children in the UK as it demonstrates that the methodology fails to adequately quantify the absolute amount of MVPA, and fails to rank individuals with respect to habitual physical activity. Marked improvements in surveillance of physical activity will be necessary in order to meet the major public health challenges of the 21st century, particularly where physical activity has been implicated in the aetiology of diseases such as obesity and related disorders.10 32 In practice, improved surveillance of population physical activity in future should mean the use of objective measurement with accelerometry, and from 2008 the English Health Survey plans to survey physical activity in children both subjectively and objectively using Actigraph accelerometry, as is the case in recent national surveys in the USA.34
The present study focused on levels of MVPA among children, since this is the construct of physical activity used in current recommendations, public health and clinical targets, and national surveillance. Children in the present study, as in other recent accelerometry studies in the UK,12–14 spent a good deal of time in light intensity physical activity (activities with an energy cost between approximately 1.5 and three times the energy expenditure of the individual at rest, such as much of childhood indoor play16). There is a dearth of evidence on the health impact of variation in light intensity physical activity during childhood and adolescence, in part because of the historical emphasis on the construct of MVPA and in part because of perceived difficulties in quantifying the amount of light intensity physical activity being undertaken. However, variation in the amount of light intensity physical activity might be important to variation in energy balance in young children,26 and light intensity physical activity is readily quantified in free-living children and adolescents using accelerometry, suggesting that it is a construct which may merit greater attention in physical activity research and surveillance in the future.14 16
CONCLUSIONS
The present study suggests that children’s apparent levels of MVPA from UK national surveys have been overestimated very substantially. The measures of physical activity obtained in UK health surveys even fail to achieve successful assessments of the relative (rank order) amounts of physical activity of children. Attempts to use children’s physical activity data from UK health surveys to assess performance in relation to public health targets, to describe secular trends in activity or to examine relationships between physical activity and health are likely to be flawed.
Acknowledgments
We acknowledge the support of an External Reference Group in conducting the study. We appreciate the support of Gateshead Health NHS Foundation Trust, Gateshead Education Authority and local schools. We warmly thank the research team for their effort. Thanks are especially due to the Gateshead Millennium Study families and children for their participation in this study.
REFERENCES
Footnotes
-
Funding: The Gateshead Millennium Study is supported by a grant from the National Prevention Research Initiative (incorporating funding from the British Heart Foundation, Cancer Research UK, Diabetes UK, Department of Health, Economic and Social Research Council, Food Standards Agency, Medical Research Council, Research and Development Office for the Northern Ireland Health and Social Services, Chief Scientist Office of the Scottish Government Health Directorate, Welsh Assembly Government and World Cancer Research Fund). The cohort was first set up with funding from the Henry Smith Charity and Sport Aiding Medical Research for Kids (SPARKS). The funding body had no influence on the decision to publish, the content of this publication, or in interpretation of the data.
-
Competing interests: None.
-
Ethics approval: Ethics approval for the study was obtained from the Gateshead Primary Care Trust Local Research Ethics Committee.
-
Patient consent: Parents provided informed consent to participation and children assented to participation.
-
Contributors: JJR was responsible for the original concept. JJR, AJA, KNP and LB designed the study. All authors contributed to study methodology, analysis, interpretation and report writing. LB, P-XL and UM collected data. All authors saw and approved the final version of the manuscript.
All authors declare that they participated in the present study as described above. The study guarantor has full access to study data and final responsibility over the decision to submit for publication.