Article Text

Abstract
Babies have specific needs that assist them in their development and enable them to thrive. Feeding is an important aspect of development. When feeding, there are opportunities for babies to develop a positive interactive bond with parents. This has a long-term impact on the well-being of infants in terms of emotional development, social learning, and health. Infants born prematurely and those born with specific needs making them vulnerable are likely to develop the necessary skills to allow them to mature, interact and thrive.
Many premature infants may need alternative feeding methods until they are ready to develop the skills necessary for oral feeding. A beneficial approach for infants who are showing oral readiness is the use of a non-nutritive sucking programme. This paper explores the research that supports non-nutritive sucking, and considers other variables that need to be included in further research, including those infants who have neurodisability.
Statistics from Altmetric.com
Feeding is an essential early routine that is necessary for nutrition and for developing a positive bond between parents and infants. It therefore has a long-term impact on the consolidation of well-being.1 As well as being a social activity, feeding involves the use of tactile and olfactory senses that are essential in an infant’s early development. Management of these skills in a vulnerable infant population requires a sensitive, multidisciplinary approach to maximise each infant’s potential.2 This short report seeks to explore the use of non-nutritive sucking as a support for premature infants in the development towards a smooth transition towards oral feeding. It will also consider the relevance of the evidence base for effective clinical application. A pilot project will be discussed that seeks to explore some of these issues.
SUCKING BEHAVIOUR IN INFANTS
Sucking in particular is vital in the early development of the infant whether it involves breast- or bottle feeding. It is essential as the means of receiving nutrition, of providing stability in distress and also of exploring the environment. Successful and effective feeding is an energetic activity that is described as being complex, requiring the coordination of a suck–swallow–breathe cycle.3 4 Research studies show that a stable swallow rhythm appears to be established earlier than a suck rhythm.5 In the high-risk neonatal population, the suck–swallow–breathe sequence is rarely well coordinated before 34 weeks.5 Premature infants often require approximately 20 postnatal days to achieve a maximal suck rate and their suck–swallow patterns are immature, displaying a dysrythmic pattern, although individual variation is recognised within this population.6
Infants use two types of sucking. Nutritive sucking is the process of obtaining nutrition with a rate of one suck per second, and is constant over the course of feeding. It involves intake of fluid due to the alternation of expression and suction. Suction is the negative intraoral pressure which occurs when the tongue and jaw become lower and the soft palate closes the nasopharynx.7 8 In contrast, non-nutritive sucking occurs at two sucks per second, in the absence of nutrient flow and may be used to satisfy an infant’s basic sucking urge or as a state regulatory mechanism.8 9 The two forms also differ in their influence on respiratory rate. Paludetto et al10 and Daniels et al9 suggest that increases in transcutaneous oxygen levels occur during non-nutritive sucking. They suggest that there is a higher respiratory rate during nutritive sucking pauses whereas in non-nutritive sucking, the respiration occurs during the sucking. Key environmental factors also influence the feeding process. They are the presence/absence of fluid, their viscosity11 and satiation, that is, the presence of milk in the stomach which inhibits nutritive sucking.12
THE NEONATAL ENVIRONMENT
The hospital neonatal environment is specifically designed to provide support and to maximise an infant’s potential in all areas of development. Most neonatal units will have a developmental care approach to managing their infants. Such approaches are important in providing appropriate and supportive environments for infants and their carers. The family is at the centre of this approach, and the rationale behind developmental care is rooted in a range of theories: transactional theory, neurobiological theory, psychoanalytical theory and synactive theory.13
The Newborn Individualized Developmental Care and Assessment Program (NIDCAP)13 focuses on observing and interpreting infant behaviour to allow practitioners and carers to interpret the infant’s needs. Individualised care plans recognise the unique and individual needs of each infant. Swaddling is a strategy used to reduce stress, and lighting as well as noise are reduced to a minimum as too much sensory stimulation can be detrimental to the infant’s well-being. Holding the infant, such as in Kangaroo Care can decrease stress and have positive psychological and emotional aspects.13 14
The development of feeding for the infant within a developmental care model is based around observing the infant’s general state, then interpreting their behaviour when preparing them to accept oral intake through approaches such as non-nutritive sucking. Observations during gavage feeding when the non-nutritive sucking programme may occur can provide important assessment information as to how to proceed with a feeding management plan.13
USING NON-NUTRITIVE SUCKING TO DEVELOP FEEDING SKILLS
Speech and language therapists in collaboration with parents, carers and other healthcare practitioners often recommend non-nutritive sucking programmes for tube fed preterm infants. This is so that the transition to oral feeding is increased, and to provide a pattern for nutritive sucking. It is considered that non-nutritive sucking will assist neurodevelopmental organisation, aid neurobehavioural maturation and optimise ventilation in preterm babies who require nasal non-invasive ventilatory support.6 15–23 In addition, use of a non-nutritive sucking programme may allow critical aspects of oral motor development to receive stimulation and reduce the adverse impact of other necessary procedures such as nasogastric feeding.24 These are important considerations as studies show that feeding difficulties within the neonatal population may prolong discharge home.25 26 Delayed introduction to oral stimulation and feeding may also lead to longer-term aversions.2
Breast feeding is regarded as an important method of feeding for all infants. Its benefits are multi-factorial and include positive growth and development,27 as well as providing protection from environmental pathogens28 29 and positive outcomes for the immune system of a baby.30 Mothers also report that when breast feeding, they actually feel that they are promoting a beneficial support for their baby.31 Breast feeding has many benefits for the developing infant, and the World Health Organization promotes breast feeding worldwide due to the many health advantages. However, it can prove particularly difficult for premature infants and this has posed something of a challenge for nurses and speech and language therapists who play a specific role in promoting breast feeding in young infants.
Nevertheless, the speech and language therapist’s principle role is to maximise an infant’s functional sucking skills regardless of the mother’s choice of feeding. Cultural, personal and health issues may also contribute to the decision as to whether to breast feed. Concerns have been raised on the use of dummies and teats during breast feeding. However, there is little evidence that the inter-changeable use of teats and nipple presentations causes confusion or that dummy use influences breast feeding development.32
Healthcare professionals working with neonates have also used assessments such as the “Neonatal Oral Motor Assessment Scale” (NOMAS33), to categorise the oral motor patterns that underlie poor feeding behaviour in neonates. The NOMAS has largely been used with bottle fed infants. Meier34 has raised issues around describing sucking during breast feeding and suggests that the terminology used in the NOMAS such as “transitional sucking” does not translate to breast feeders as a wide jaw excursion is essential for effective breast feeding. However, given the Collins et al32 findings above where there is minimal evidence to support the issue of nipple/teat confusion, the NOMAS is regarded as a valuable clinical tool. Furthermore, evaluations have revealed that the NOMAS has a high inter-rater reliability, and also has been described as being helpful in identification of those infants who present with long-term risk.33–35
RESEARCH INTO NON-NUTRITIVE SUCKING
Studies have evaluated the impact of non-nutritive sucking on oral feeding. However, none have clearly addressed the link between non-nutritive sucking and nutritive sucking, nor have they proposed an intervention strategy for use in a neonatal environment. Measel and Anderson6 randomly assigned infants aged 28–34 weeks’ gestation to a treatment group (use of dummy during non-oral feeding to provide an association between sucking and satiation) or control group (no dummy). Specific details of the treatment protocol are not given, but the treatment group of infants were ready for bottle feeds earlier, had fewer tube feeds, gained more weight and were discharged earlier. Field et al17 and Seghal et al36 obtained similar results.
Recent studies23 24 have described a non-nutritive programme more precisely. The treatment group received a daily 15-minute oral stimulation programme (stroking the peri- and intra-oral structures), for 10 days prior to oral feeding. This is an impressive result given the relatively undemanding treatment programme. The first study,18 found that independent oral feeding was attained, on average, 11 days sooner in the group that received the intervention within a group of 32 infants. In addition, the treatment group went home 5 days sooner. The later study19 looked again at 32 infants but those who had a gestational age of between 26 and 29 weeks. The oral motor programme commenced 48 h post-cessation of continuous positive airway pressure (CPAP). The intervention was carried out by nurses or researchers 30 minutes before a tube feed. Those infants who had received the intervention went on to full oral feeds 7 days sooner than the control group. Later studies also demonstrate positive outcomes, but researchers or therapists have carried out the intervention, rather than the parents themselves.37 38 The Boiron et al study37 examined 43 infants aged 29–34 weeks’ gestation. The oral motor programme as used by Fucile et al18 19 was carried out, but there were additional groups involving use of cheek and chin support, use of oral stimulation and support, and use of the oral stimulation alone. The group that received both oral support and oral stimulation took the least amount of time — 5.6 days — to move onto full oral feeding. There was no mention of breast feeding, or encouraging parents to participate in the programme. The Rocha et al study,38 which looked at 98 very low birth weight premature infants, also had similar outcomes. Speech and language therapists carried out this intervention, but this was largely focusing on bottle fed infants with little focus on developing parental skills in enhancing the infant’s feeding potential. This seems to go against the principles of collaborative working with parents and carers that healthcare professionals continually attempt to achieve.
RELATING THE LITERATURE TO CLINICAL PRACTICE
Clinically, therapists and nurses are aware of developing positive oral experiences to promote both interaction and to encourage and maximise oral skills.39 40 Early oral motor stimulation is encouraged to maintain and develop the sucking reflex. Within this framework, early communication and learning to respond to the infant’s attempts to interact are an integral part of a therapist’s role. Authors such as Harris24 and Wolf and Glass23 recommend perioral and intraoral touch–pressure and nipple and finger-sucking experiences before bottle- or breast feeding. Bazyk39 suggests that non-nutritive interventions for premature infants who receive tube feeds are justified and can accelerate the transition from tube-to oral feeding by allowing the infant to practise using their oral motor musculature.
LIMITATIONS OF THE STUDIES
Review of the literature reveals that despite considerable variability in methodology as well as in outcomes being measured, non-nutritive sucking clearly has benefits in promoting an infant’s readiness to begin oral feeding. The rationale as to when to implement non-nutritive sucking, that is, before a tube feed, on initiation of a tube feed, or after a tube feed, is wide ranging, with unclear links to feeding development. In addition, the major studies quoted18–20 22 37–39 focus on researchers and staff, not parents actually carrying out the procedure, with a high level of bottle fed infants, rather than a mixture of the expected breast- and bottle feeders. As has already been stated, breast feeding and the development of an infant’s ability to do this pre-discharge are regarded as highly important. None of the studies have any longitudinal aspect to them in terms of any longer-lasting benefits for the infants participating, or have reflected on the early communication development.41 Finally, none of the studies actually use infants with neurodisability, and hence the more typical speech and language therapy caseload infants.
REFLECTIONS ON A PILOT PROJECT
A pilot study involving 14 infants41 devised a parent-lead non-nutritive sucking programme based on speech and language therapy principles. These principles focused on parents’ understanding of the rationale underpinning the intervention where they actually carried out the non-nutritive intervention to promote both positive communication opportunity and develop productive oral motor skills. The aims were to ascertain if a parent-lead non-nutritive sucking programme assisted infant feeding development, enabled effective development of jaw and tongue movement and had any influence with long-term benefits when the infants were ready to wean.
The study took place within a developmental care environment. This study specifically was exploring the rationales underpinning a recommended therapy approach, that is, non-nutritive sucking to promote successful transition to oral feeding within a population of premature infants.
Participants were recruited from the neonatal unit of a district general hospital based in the south of England. All parents gave informed consent after reading information prepared for them and after discussion with the speech and language therapist and nursing staff. They were advised that they could withdraw consent at anytime.
Fourteen infants participated: 11 boys and three girls. Infants were included if they were born between 27 and 35 weeks and weighed between 1000 and 2000 g at 32 weeks after which oral feeding was introduced. They were required to have a minimum Apgar score of 3 at 1 minute and 5 at 5 minutes. Infants with chronic medical problems (cardiac difficulties, unresolved respiratory problems requiring oxygen, renal sepsis, surgery, or medications with central effects, intra-ventricular haemorrhages, and general congenital or neurological anomalies) were excluded.
A matched-pairs design was used. Infants were matched for gestational age and birth weight and a member of each pair was randomly allocated to a treatment or control group. Infants were assigned to groups using a stratified random sampling technique to ensure that the groups were similar in mean gestational age and birth weight. Selection to the intervention or control group was carried out by a computer-generated random number system. The groups were compared on the length of their stay in hospital, the number of days taken to transfer to full oral feeding and the change in NOMAS scores during the intervention (table 1). Informal follow-up occurred at 8 months.
Procedure
Four training sessions were delivered to nursing and medical staff to provide a background to the intervention rationale. Parents in the treatment group were expected to provide 10 minutes of oral stimulation by gently stroking the bottom lip with a finger or dummy, then moving intraorally to stimulate the tongue in a gentle front to back movement until the finger/dummy was prompting a non-nutritive suck pattern. This was carried out during the first 10 minutes of a tube feed.
The NOMAS was used to assess oral–motor performance during non-nutritive sucking before and after intervention. It scores infants on the number of normal, disorganised or dysfunctional patterns seen. Disorganised patterns are characterised by arrhythmic jaw movements, difficulties coordinating a suck–swallow–breathe pattern and an inability to slow down the sucking pace. Dysfunctional characteristics include an excessively wide jaw excursion or minimal excursion, asymmetry of the jaw and limited tongue movement, and either a flaccid or retracted tongue. The assessment was conducted by the researcher and a peer unaware of the group allocation of the babies, both trained users of NOMAS.
Data were collected at a scheduled tube feed prior to implementation of the first oral feed when the infant was 32–33 weeks. Non-nutritive sucking patterns were observed for a 10-minute period and evaluated in terms of the NOMAS categories.
Infants in the control group still received the usual developmental care approach from the unit, with a speech and language therapist providing verbal support and discussion of oral feeding. Developmental care seeks to benefit infants by adapting the nursery environment, adapting the care of the infant, through an infant-lead approach, and through close collaboration with the family.13 Care is individual and adjusted to fit an infant’s emerging skills and needs and the needs of the family. When infants in the experimental group started to tube feed, parents kept the dummy/finger in the infant’s mouth for 10 minutes using the method described earlier. All parents who elected to have a dummy used the Smoothie pacifier. This was carried out three times a day. The researcher met with parents and nursing staff daily to evaluate progress. Informal follow-up occurred once the infants were 8 months of age.
RESULTS
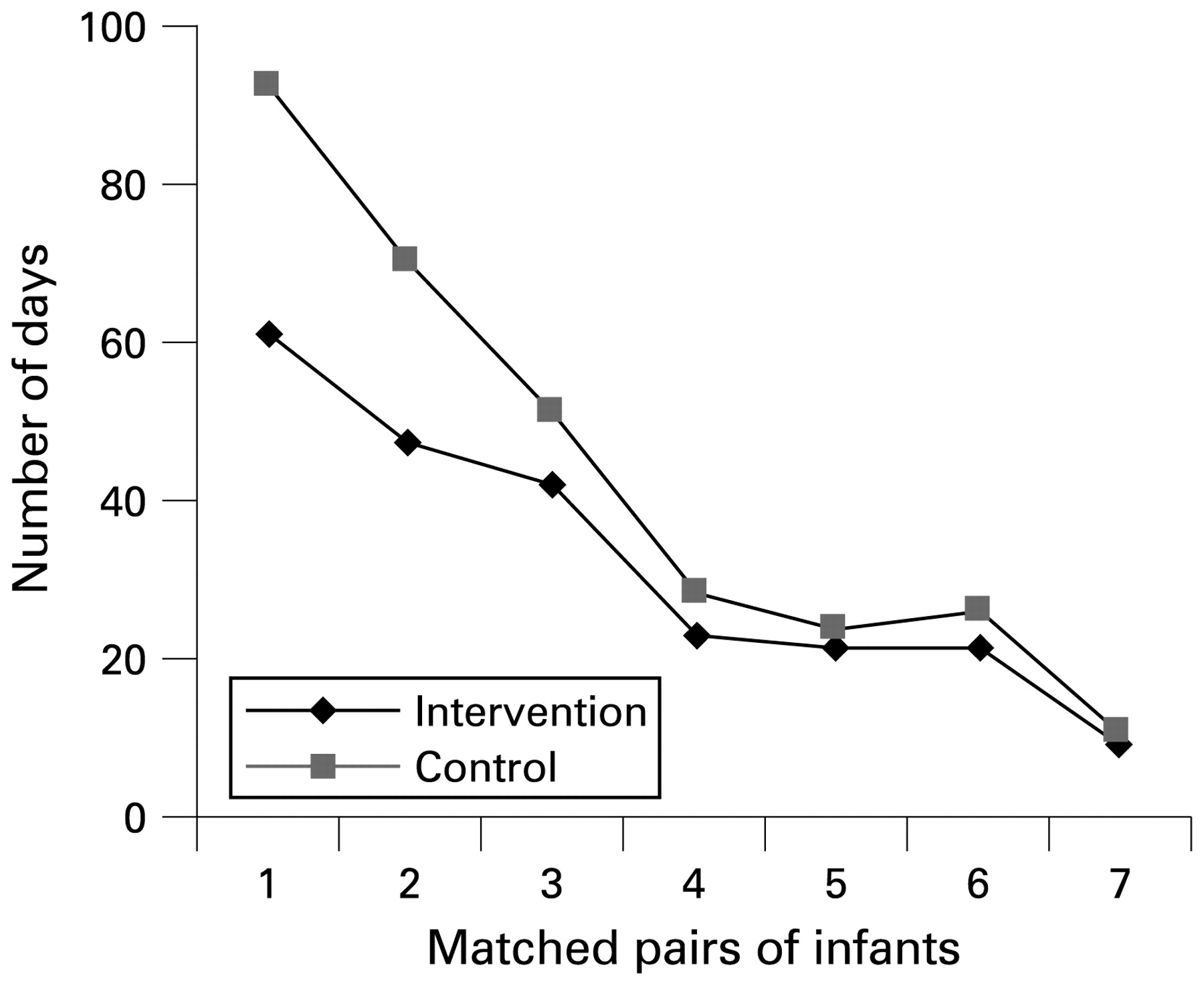
Table 2 gives the median and range for each group. The pairs of children within the groups were compared using the Mann–Whitney U test. These showed that the treated group took fewer days to achieve oral feeding (a difference of 3 days, U = 11 (n = 14), p = 0.082 >0.05: not significant, but trend apparent, fig 1), and spent fewer days in hospital (difference of 5 days, U = 16 (n = 14), p = 0.277 >0.05: not significant, fig 2). It is interesting to note that infants of a lower gestational age benefited more directly from the programme.

Graph illustrating the results for the number of days taken to achieve full oral feeds.
{kind=link}
{kind=link}
Graph illustrating the number of days spent in hospital.
Table 3 shows the change in the number of normal aspects of sucking using the NOMAS both before introduction of oral feeds, and once the infant is on full oral feeds. The change in NOMAS scores from before introducing oral feeds to when the infant was able to take full oral feeds without tube support in the two groups was compared. Table 3 shows the means and ranges of scores, and results of the Mann–Whitney U test.
Parents received an informal follow-up telephone call 8 months after discharge. Comments from the parents of infants who had received the intervention remarked that weaning had progressed well. In addition, some commented that they had felt they were providing support for their baby and enabling them to develop skills by carrying out the non-nutritive sucking programme. A parent from the control group commented that her son had had significant difficulties weaning, and was finding it difficult to move away from pureed textures. Informal follow-up at 8 months of age indicated that weaning was more quickly established with the treatment group. Parents were asked to reflect on the non-nutritive sucking programme. Comments from the treatment group included: “I felt that the sucking programme was helpful not just to BS, but to me also. I often felt so helpless looking after him, but the programme made me feel I was doing something to help my son”. Interestingly, parents in the control group mentioned some difficulties with establishing weaning: “I dread mealtimes and I get really frustrated. Already I am getting angry with him”. This information was an informal consideration, and does require a much more rigorous approach and evaluation within a wider-scale study.
SUMMARY
The results gained from this study where parents carried out the intervention were comparable to studies described in the rationale,6 22 with treatment group infants going home 5 days sooner than the control group, and gaining full oral feeding ability 3 days sooner. In addition, significant differences were noted with oral motor function as measured by use of the NOMAS33 between both groups. More importantly, this study involved the parents and carers actually carrying out the intervention, not researchers. The informal follow-up at 8 months did highlight some issues that would benefit from further study. Within this pilot project, this was only a superficial exploration, and therefore requires a more rigorous study that attempts to evaluate some of these issues further. It is interesting to explore further the weaning development of infants within an intervention group, although there will need to be a more structured analysis of how and when the infants developed. In addition to this, there is clearly a highly beneficial effect for infants born earlier, and this has influenced to some extent the populations used in two of the more recent studies.37 38 It is possible to speculate on neonatal feeding development in relation to plasticity of the system with earlier gestational ages, although this finding clearly requires much greater analysis and exploration.
In summary, it appears that there are undoubted benefits as indicated by the literature discussed of using non-nutritive sucking with infants who are premature. In particular, non-nutritive sucking is seen to have benefits in terms of successful transition to oral feeding and quicker discharge home. Interestingly, infants who are born earlier benefit more from the procedure than those born later, and this would clearly benefit from further study.
It is hard to consider if other variables with the developmental care model such as the sensory and tactile feedback associated with use of Kangaroo Care contribute to an infant’s well-being and therefore readiness to progress and develop other skills such as feeding. However, most of these studies do not make a clear distinction between breast- and bottle feeders; this is an issue that does require further careful consideration given the high priority and encouragement that is actually given to breast feeding within the UK. In addition, within neonatal units there is an ethos of encouraging parents to participate in aspects of their infant’s care; only one paper attempts to address this issue.38 Long-term implications are largely absent in terms of longer-term benefits, although one paper tentatively explores this.38 Finally, none of the papers discussed actually reflect on the typical population that nurses and therapists would usually implement a non-nutritive sucking programme with, that is, those with neurodisability. Further research needs to build on the current literature base and address these issues more clearly so that a cohesive strategy for an approach that has undoubted benefits for a vulnerable population can have clinical application for a wider group.
What is already known on this topic
Non-nutritive sucking is a beneficial process in helping to stabilise the infant during a range of processes.
In particular, non-nutritive sucking has been shown to assist quicker transition from tube- to oral feeding within a premature infant population.
What this study adds
Consideration about how future studies need to consider the benefits of non-nutritive sucking and its application to a neurodisability population of premature infants.
Evaluation of current research in relation to current practice and how it can be applied to the neonatal environment.
REFERENCES
Footnotes
Competing interests: None declared.
Ethics approval: Ethical approval was granted by the local Trust.
Patient consent: Parental consent obtained.