Article Text

Abstract
Objective: To determine the viral aetiology of respiratory infections in children presenting to primary care with “more than a simple cold”.
Design: Observational study in 18 Oxfordshire general practices over four winters (2000–01 to 2003–04).
Patients: 425 children aged 6 months to 12 years with cough and fever for whom general practitioners considered prescribing an antibiotic.
Methods: Nasopharyngeal aspirate obtained from 408 (96%) children was subjected to PCR for respiratory viruses. Parents completed an illness diary for the duration of illness.
Results: A viral cause of infection was detected in most (77%) children. Clinical symptoms correctly identified the infecting virus in 45% of cases. The duration of illness was short and the time course was very similar for all infecting viruses. One third of children were prescribed an antibiotic (34%), but this made no difference to the rate of parent-assessed recovery (Kruskal-Wallis, p = 0.67). About one in five children with influenza who did not receive an antibiotic had persistent fever on day 7 compared to no children receiving antibiotics (p = 0.02); this difference remained after adjustment for severity and other factors and was not seen with other viruses.
Conclusions: Most children receiving antibiotics for respiratory symptoms in general practice have an identifiable viral illness. In routine clinical practice, neither the specific infecting virus nor the use of antibiotics has a significant effect on the time course of illness. Antibiotics may reduce the duration of fever in children with influenza which could reflect an increased risk of secondary bacterial infection for such children.
- CARIFS, Canadian Acute Respiratory Illness and Flu Scale
- CART, classification and regression tree
- IQ, interquartile
- NPA, nasopharyngeal aspirate
- PCR, polymerase chain reaction
- respiratory infection
- primary care
- antibiotic
- influenza
Statistics from Altmetric.com
- CARIFS, Canadian Acute Respiratory Illness and Flu Scale
- CART, classification and regression tree
- IQ, interquartile
- NPA, nasopharyngeal aspirate
- PCR, polymerase chain reaction
The UK government has advised general practitioners to avoid prescribing for “simple coughs and colds” because of the risk of antibiotic resistance.1 From 1995 to 2001 antibiotic prescribing in primary care was reduced but more recently has not declined further and remains common, particularly for children with respiratory infections.2 This partly reflects the limited evidence base for the government advice: clinical trials focusing on cough and fever have excluded children under 8 years of age or have been of poor quality.3,4 It also reflects a belief that antibiotic trials of respiratory infections in general practice have tended to exclude the children with more severe symptoms who might benefit most from an antibiotic.5
We asked participating general practitioners to identify children presenting with cough and fever whom they considered to have more severe clinical symptoms and signs than a simple cold and for whom they would consider prescribing an antibiotic. We report a prospective study of the aetiology and time course of illness in these children.
METHODS
Study design and participants
We prospectively recruited 425 children from primary care who fulfilled five inclusion criteria: (i) age 6 months to 12 years; (ii) a cough; (iii) a fever reported by the parent within the past 72 h; (iv) severity of symptoms/signs suggesting an acute respiratory infection which was “more than a simple cold”; and (v) the general practitioner considered prescribing an antibiotic. The exclusion criteria were non-consent and an inability to complete a parental diary. Recruitment took place over four winter seasons (2000–01 to 2003–04). The analysis reported here is restricted to the 408 children (96%) in whom we obtained a nasopharyngeal aspirate with parental consent.
Recruitment of participants
We recruited children from 18 general practices in Oxfordshire, UK (four practices participated in all four winter seasons). After seeking parental agreement (and in the case of older children, their agreement), general practitioners contacted a research nurse with paediatric training who saw the child on the day of referral, either in the practice or in the child’s home. We asked general practitioners to rate the severity of illness of each child by marking a 0–10 visual analogue scale with the range “child with a simple cold” to “child sufficiently unwell to need admission to hospital” on a referral form. Recording of prescribing, symptoms and demographic details was done by the study nurse. We asked parents to record symptoms in a diary (see below) and to rate the severity of their children’s illness on a 0–10 visual analogue scale with the range “best possible health” to “worst possible health”.
Parental diary
We asked parents to record their child’s symptoms three times a day for the first 2 days of their child’s illness, and then daily until 2 days after their child had recovered using a diary based on the 15-item Canadian Acute Respiratory Illness and Flu Scale (CARIFS).6,7 Using CARIFS parents recorded whether a symptom was major, minor or no problem. The diary data were double-entered by the research nurses participating in the study and errors were reconciled with the original data. In analysing data on temperature, children were characterised as having fever if the recorded axillary temperature was 37.5°C or above or they had been given paracetamol for fever by the parent.
Nasopharyngeal aspirate
After we had obtained consent, a research nurse collected a nasopharyngeal aspirate (NPA) with a Vygon infant mucus extractor (Vygon, Ecouen, France) and suction catheters size 6F and 10F using a DeVilbiss suction unit (Sunrise Medical, Wollaston, UK). The sample was transported to the laboratory within 4 h and samples were processed upon arrival. We performed polymerase chain reaction (PCR) assays on an aliquot of the nucleic acid extract from the sample and amplified gene fragments from influenza A and B, respiratory syncytial virus A and B, human metapneumovirus, parainfluenza 1–4, adenovirus and picornavirus.8,9
Statistical analysis
We performed all analyses using the statistical packages SPSS and R.10 We assessed statistical significance using the Kruskal-Wallis test to compare continuous variables and χ2 tests to compare categorical variables except for the analysis of duration of fever where we employed Kaplan-Meier plots and the log rank statistic for the unadjusted comparison and a Cox proportional hazards model to adjust for potential confounding factors. In reporting the overall time course of the illness from presentation, median CARIFS scores were plotted and statistical significance assessed by a Kruskal-Wallis test of the difference in the summed daily CARIFS scores for each child (for the first 2 days, when parents made more than one diary entry, the value taken for the analysis was the first recording of the day). To explore the diagnostic potential of clinical symptoms in identifying individual viruses, we used the Therneau and Atkinson RPART routine in R to create a classification and regression tree (CART) model.
RESULTS
Cause and severity of illness
A probable viral cause for the illness was detected in 316/408 (77%) children. The main viruses detected were influenza virus (134, 33%), respiratory syncytial virus (59, 14%) and parainfluenza virus (58, 14%). The recently identified human metapneumovirus was responsible for 33 (8%) cases. In 55 (2.7%) children we identified two or more viruses. Table 1 reports the duration and severity of illness at presentation according to viral aetiology. The median length of illness before consultation was between 5 and 7 days. Children with respiratory syncytial virus had a median physician assessed severity score of 5.0 compared to 3.1–4.1 for the other viruses, but the interquartile (IQ) ranges for each virus overlapped substantially. The median age at presentation was highest for influenza (4.2 years), but again with substantial overlap of the ranges for each virus.
Duration and severity of illness and antibiotic prescribing at presentation according to virus identified
Presenting symptoms
The infecting virus could not be diagnosed with any certainty from the clinical symptoms. Cough and fever were entry criteria for the study and were presenting symptoms in all children. Nasal discharge (present in 84% of children) also occurred with very similar frequency in all viruses. Conjunctivitis occurred more often in human metapneumovirus than other viruses (30% vs 10%, p = 0.01). Wheeze occurred more frequently with respiratory syncytial virus than with the other viruses (44% vs 21%, p<0.01). The best performing clinical decision rule generated by the CART programme was based on a combination of symptoms (presence or absence of conjunctivitis, wheeze, ear infection, vomiting and lymphadenopathy) which correctly identified the infecting virus in 45% of cases (human metapneumovirus 32%, influenza 38%, parainfluenza 44%, respiratory syncytial virus 71%).
Overall impact and duration of illness
Figure 1 illustrates the duration and impact of the illnesses caused by the different viruses. The similarity between the time course of illness with all viruses is clear. Irrespective of infecting virus, the median CARIFS score fell to 0 (ie, the parents reported no illness-related problems) within 9 days. The absolute difference in the overall CARIFS score between viruses on any single day was not more than 5 points (which equates to an approximately 1-point difference on a 10-point visual analogue scale from best to worst possible health). There was no significant difference in time to recovery between influenza and respiratory syncytial virus, but the time to recovery from these two illnesses was slightly longer (median 1 day) compared to parainfluenza, metapneumovirus or no virus identified (Kruskal-Wallis, p = 0.001).
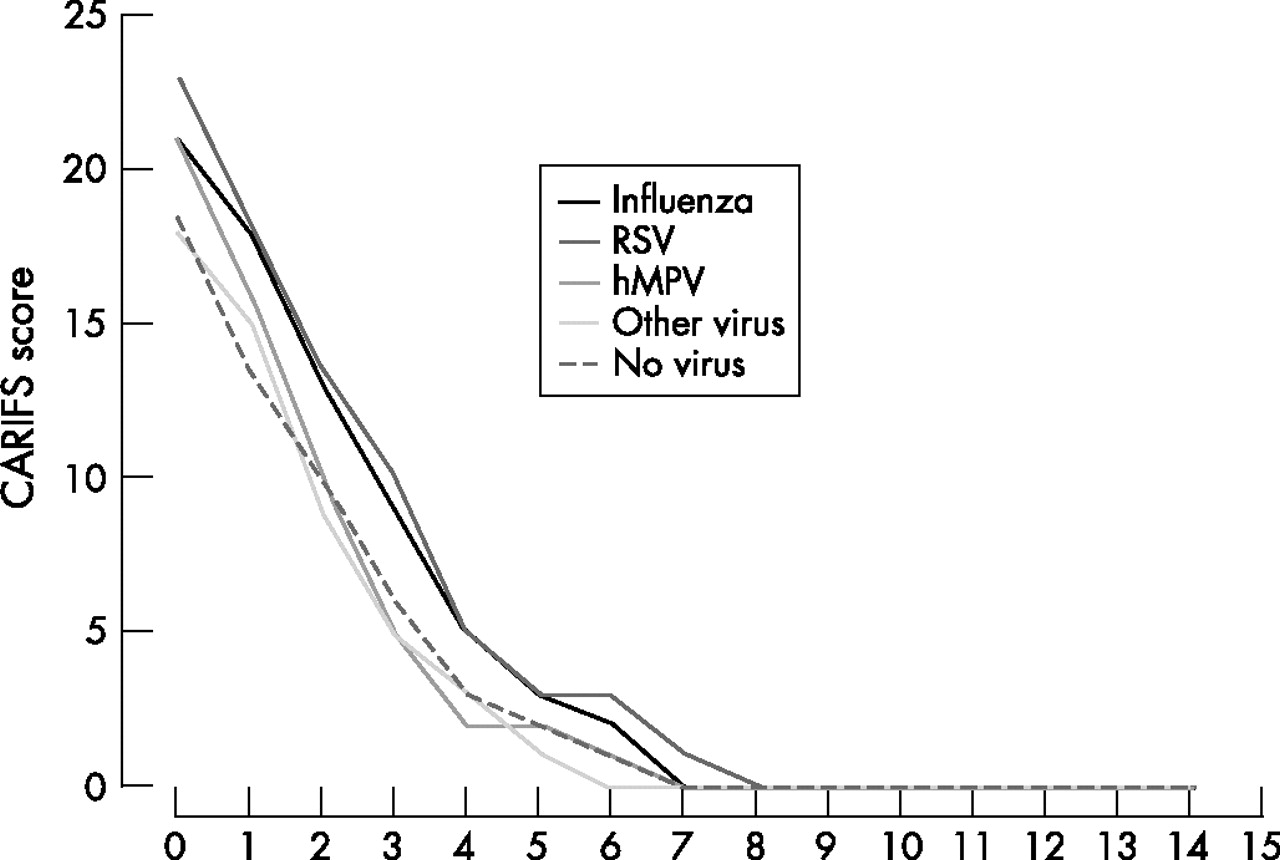
Duration and severity of illness (median overall CARIFS score on each day following presentation) according to virus detected. hMPV, human metapneumovirus; RSV, respiratory syncytial virus.
Time course of symptoms
The time during which the parent characterised the child as “unwell” mirrored the overall CARIFS score, with a median duration of illness of 4 days and only 5% of children remaining unwell by day 10 (human metapneumovirus 0%, influenza 4%, respiratory syncytial virus 5%, other virus 7%). Vomiting subsided most rapidly reaching the “less than 5% affected” level by day 5; fever reached this level at day 9, nasal congestion at day 13 and cough at day 15. The maximum duration of symptoms for human metapneumovirus in particular was very short: vomiting and earache 5 days, fever 7 days, tiredness 9 days, irritability 10 days. As with the other viruses, cough was the most persistent symptom, but remained a problem for more than 2 weeks in only 6% of children. About one in five parents (21.0%) re-consulted the general practitioner because of continuing concerns about the illness. Four children were referred to hospital.
Effect of antibiotic prescribing on parent-assessed outcome
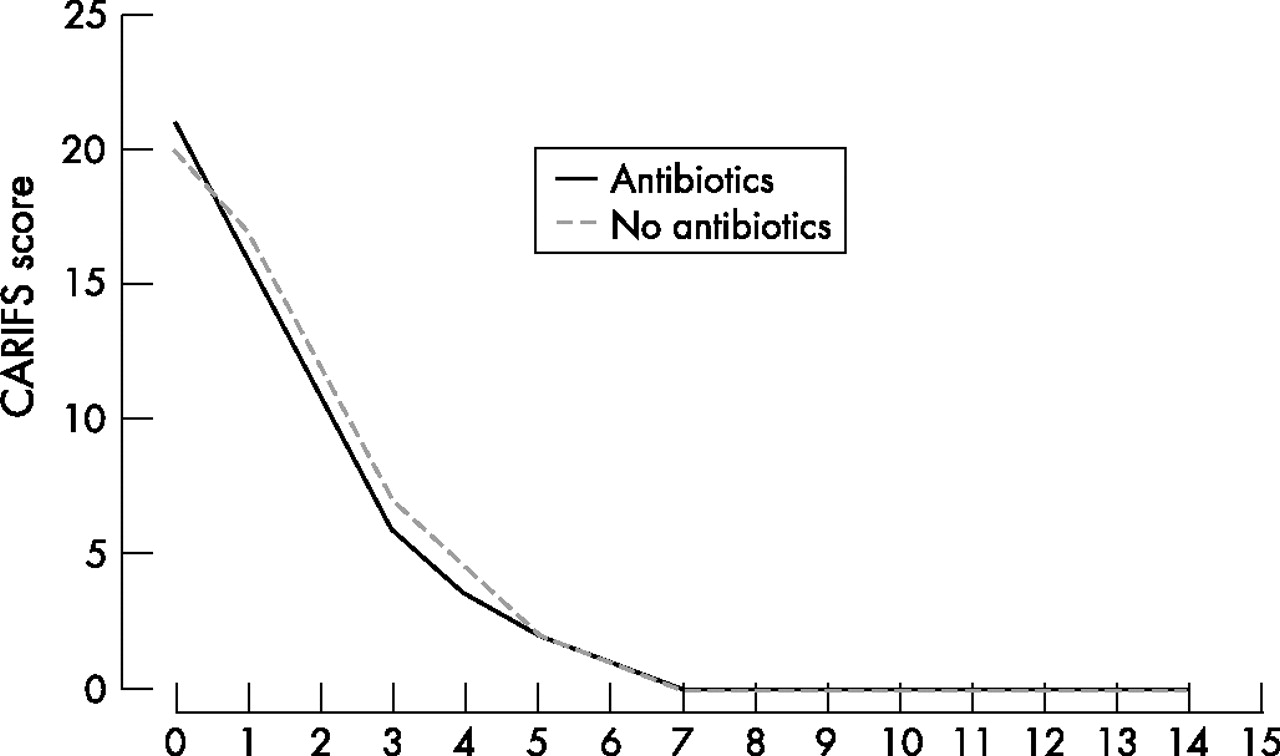
About a third of children were prescribed an antibiotic (139/408, 34.1%), usually amoxicillin. Prescribing was significantly more common with human metapneumovirus (44%) and respiratory syncytial virus (46%) than with influenza (24%, p = 0.03). The impact of prescribing on the severity of illness as assessed by the parent is shown in fig 2. Children prescribed antibiotics had a slightly higher CARIFS score at presentation (median 21 vs 20, Kruskal-Wallis, p = 0.06), but children recovered at the same rate whether or not they had been prescribed an antibiotic (Kruskal-Wallis, p = 0.67). There was no suggestion of a clinically important or statistically significant difference between viruses in this respect.

Duration and severity of illness (median (CARIFS score on each day following presentation) according to whether or not an antibiotic was prescribed at presentation.
Effect of antibiotic prescribing on temperature
Figure 3 shows Kaplan-Meier plots for time to recovery from fever according to infecting virus. Again, there is no suggestion of a clinically important or statistically significant effect of antibiotics except in children with influenza. In the non-antibiotic group, a significant number of the children display delayed recovery (log-rank, p = 0.02). By day 7 all children in the antibiotic group had recovered, but there was a significant tail (of about one in five children) in the non-antibiotic group with persistent fever. The statistical significance of this difference in time to recovery between the antibiotic and non-antibiotic groups remained after adjustment for age, sex, initial severity and duration of illness (Cox proportional hazards model, p = 0.05).

{kind=link}
{kind=link}
{kind=link}
Time to resolution of fever (days from consultation) according to virus detected and antibiotic prescribing. hMPV, human metapneumovirus; RSV, respiratory syncytial virus.
DISCUSSION
Molecular diagnostic technology and the collection of nasopharyngeal aspirates allowed us to identify a cause of infection for a substantially higher proportion of children than in previous community-based studies and to show clearly that the majority of children with respiratory infection “more than a simple cough or cold” for whom the general practitioner would consider prescribing an antibiotic have an identifiable viral aetiology. Whilst we cannot exclude co-infection with bacteria, we found that the prescribing of antibiotics made no difference to the overall time course of illness. One of the criticisms of negative results in previous trials of antibiotics in community-acquired respiratory infections has been that those children at the severe end of the spectrum have been excluded because of lack of physician treatment equipoise. One of the strengths of our observational design has been to identify those children with more severe respiratory infection and to allow the doctor to prescribe as they saw fit. Consequently our findings help underpin the existing guidance that suspected lower respiratory infections in the community are predominantly viral and, in the absence of any significant respiratory difficulty indicating a need for hospital admission, are self-limiting and do not require antibiotics.
What is already known on this topic
-
UK general practitioners continue to prescribe antibiotics to children with respiratory infections despite guidelines to avoid their use in “simple coughs and colds”.
-
Parents are more likely to request antibiotics in the absence of a clear diagnosis and prognosis.
What this study adds
-
77% of children in primary care with “more than a simple cold” have an identifiable viral aetiology.
-
Parent-reported symptoms resolved at very similar rates irrespective of viral aetiology and antibiotic use.
-
Antibiotics may reduce the duration of fever in children infected with influenza which could reflect an increased risk of secondary bacterial infection for such children.
Our results also confirm that it is not possible to diagnose the cause of cough and fever in children on the basis of clinical symptoms alone. The technology is now available to make a firm microbiological diagnosis in primary care for the two most common viruses identified, which could give general practitioners and parents more confidence in avoiding antibiotic prescribing. However, the time course of the infection was remarkably similar whatever the aetiology: most children were better 1 week after presentation, less than 2 weeks after onset of illness. So giving parents an accurate prognosis may be more important than an accurate diagnosis. An additional strategy to reduce antibiotic prescribing suggested by our results could be vaccinating children for influenza.
Our specific observation that antibiotics were associated with a significant reduction in duration of fever in influenza is consistent with reports of a 10–17% secondary bacterial infection rate in children following influenza infection.11,12 Influenza virus precipitates secondary bacterial infection by causing destruction of the respiratory epithelium and promoting bacterial adherence.13,14 Current clinical guidelines for managing pandemic influenza recommend antibiotics, neuraminidase inhibitors and rapid influenza tests.15 Our observation merits a trial of the early (before secondary bacterial infection is apparent) use of antibiotics in children with influenza.
Acknowledgments
The authors acknowledge the efforts of the research nurses involved in this study: Susan Bates, Sarah Bryson, Sarah Burton, Sarah Chadwick, Gill Dunn, Susan Elsom, Fiona Goddard, Geraldine Jewell, Helen Lambourne, Pauline Marshall, Diane McLeod, Angela Roome, Susan Rous, Judy White and Wendy Willmore; and also David Griffiths for laboratory support and Susan Smith for administrative support. The authors also wish to thank all the physicians and nurses in the OXCIS network of surgeries for recruiting the children into this study and the children and parents who participated
CONTRIBUTORS
AH, RMW, DC and DM obtained funding for the study. AH co-ordinated the recruitment of children, biological sampling and data collection. AB performed and DC supervised the microbiological work. AT served on the steering committee overseeing the conduct of the study. RP performed and AH and DM supervised the data analysis. AH and DM wrote the manuscript and all authors made contributions to the redrafting. AH is guarantor for the paper.
REFERENCES
Footnotes
-
Published Online First 16 March 2007
-
Funding: The research was funded by the UK Medical Research Council as part of a programme grant in childhood infection in primary care (G0000340).
-
Competing interests: None declared.
-
Ethics: The study was approved by the Oxford Research Ethics Committee
Linked Articles
- Précis
- Atoms