Article Text

Abstract
A postal survey of 1024 UK GP practices showed the prevalence of medically unexplained severe fatigue over three months in 5–19 year olds to be 62/100 000. Cases were predominantly adolescent girls and were more likely to come from practices in less deprived areas, which could reflect consulting behaviours.
- CF, chronic fatigue
- CFS, chronic fatigue syndrome
- ME, myalgic encephalomyelitis
- prevalence
- primary care
- severe fatigue
- survey
Statistics from Altmetric.com
Although chronic fatigue in UK adult primary care patients is relatively common,1 there have been no comparative studies in children. Estimates of the prevalence of chronic fatigue syndrome (CFS) or CFS-like illness in children vary widely according to case definition and methodology and range from 2.7/100 0002 to 570/100 000,3 although they all suggest that the prevalence is lower than among adults.1
The diagnosis of CFS is one of exclusion. Although there are internationally accepted diagnostic criteria for CFS in adults,4 there are none for children. Most studies have applied adult criteria, although it has been suggested that three rather than six months of fatigue is more appropriate for children.5 There is also evidence from adult studies that CFS-like illnesses are given a variety of diagnostic labels by GPs.1,6 Given these considerations, estimating the prevalence of CFS-like illness in the primary care population requires a broad case definition in the absence of independent medical assessment. This paper reports a survey of cases of severe disabling fatigue of over three months in 5–19 year olds in primary care and the diagnoses given by the GP.
METHODOLOGY
In 2000 a postal survey of the 1024 practices in the MRC’s General Practice Research Framework (GPRF) was undertaken. Nurses reported the number of 5–19 year olds consulting their GP in 1999 with severe disabling fatigue for at least three months with a premorbid level of activity significantly reduced or impaired, including patients who had subsequently recovered. For each case, we obtained age, sex, GPs’ provisional diagnosis, the practice’s 5–19 year old population, and Jarman deprivation score. No patient identifiers were collected and practices remained anonymous to the researchers; ethical approval was not sought.
RESULTS
A total of 718 practices (70%) responded, reporting 542 patients; 444 practices had none and 274 had at least one; median number of cases per practice was 1 (range 1–17).
Age and sex were provided for 480 cases (88%) (fig 1); 316 were girls (66%) and the proportion increased with age: 50% (12/24) of 5–9 year olds, 62% (147/236) of 10–15 year olds, and 72% (155/214) of 16–19 year olds. The peak of cases was at 15 years of age (n = 78); in boys the number of older cases dropped sharply, whereas in girls the number remained high until 18.

Breakdown of reported cases by age and gender (n = 474).
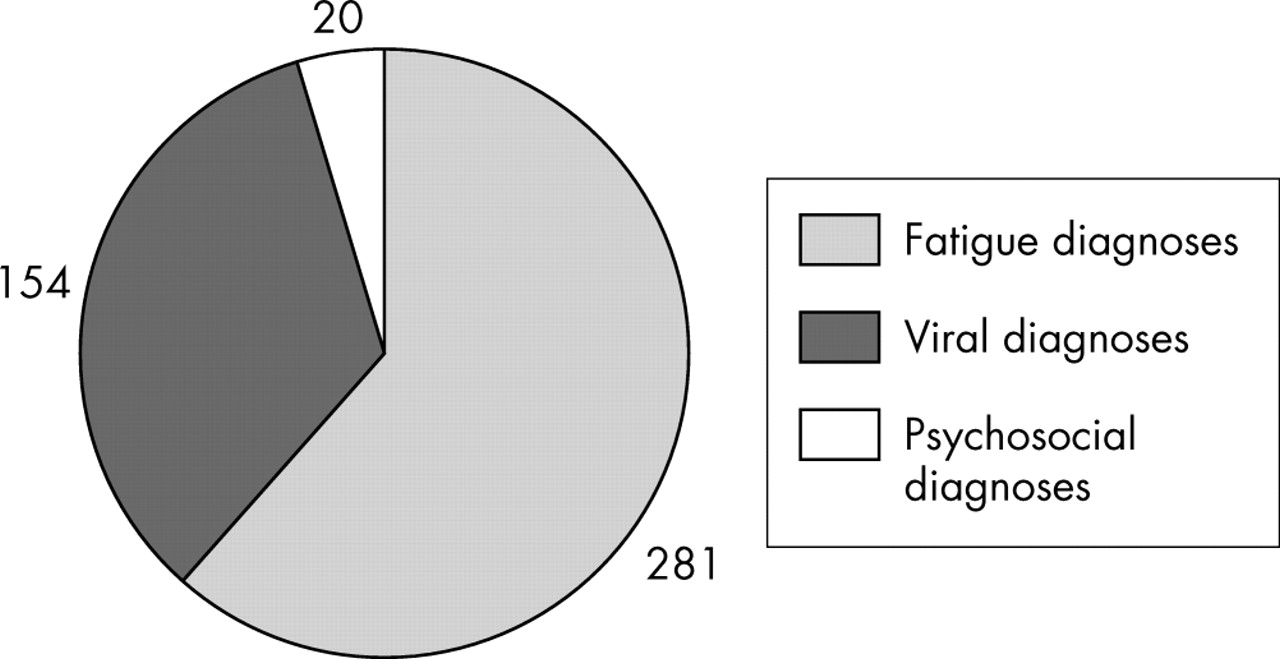
A clinical member of the research team (RWIC) reviewed 468 cases (86%) with known diagnosis to identify cases where medical or psychiatric diagnoses (other than CFS/ME) might explain the fatigue.4 In 13 cases (2.7%) the diagnosis provided a likely medical explanation for the fatigue. In the remaining 455 cases it did not. These cases were grouped as: fatigue diagnoses (n = 281; 62%) (chronic fatigue (CF), CFS, fatigue/severe fatigue syndrome, fatigue, lethargy, malaise, ME, CFS/ME, fibromyalgic CFS, and fibromyalgia); viral diagnoses (viral infection, post-viral fatigue) (n = 154; 34%); and psychosocial diagnoses (depression, bullying, family factors) (n = 20; 4%) (fig 2). Overall 234 cases (51%) were diagnosed with CFS, ME, CF, or severe fatigue syndrome.
{kind=link}
{kind=link}
Provisional diagnoses given by GP (n = 455).
Prevalence was calculated using the 5–19 year old population given by 496 practices. Practices reporting over six cases with no diagnosis were excluded from the denominator. Excluding cases with diagnoses explaining the fatigue and those with no diagnosis, there were 410 cases in a population of 655 668, a prevalence of medically unexplained fatigue of 0.062% (95% CI 0.056 to 0.069).
In 341 of these cases we have age information: 18 (5%) were 5–9 years old, 88 (26%) were 10–14 years old, and 235 (69%)15–19 years old.
There was no difference in deprivation scores among responding and non-responding practices (z = −0.604; p = 0.546; NS), but responders had a lower total practice population than non-responders (z = −2.68; p = 0.007) (median = 6500 (IQR = 4005–10 108) v median = 7501 (IQR = 4450–11 200)).
Comparison of practices with and without cases showed those with cases had a higher total practice population (z = −6.640; p < 0.001) (median = 8381 (IQR = 5000–11 475) v median = 5740 (IQR = 3500–8800)) and were more likely to be in less deprived areas than those without cases (z = −3.977; p < 0.001) (median = 4 (IQR = −7 to 13) v median = 8 (IQR = −1 to 19)).
DISCUSSION
This study was a retrospective cross-sectional survey with no validation of the diagnostic information given or clinical assessment of cases and a broad case definition. The cases nevertheless had similar characteristics to cases of childhood CFS previously described, with a predominance of girls and peak prevalence in adolescence.7 A recent adult primary care study suggests only one third of patients with over six months of fatigue met the CDC CFS criteria,6 and although over half of our sample were given fatigue diagnoses, it is likely that only some are cases of CFS if validated against established criteria. The prevalence of medically unexplained severe fatigue of over three months in 5–19 year olds in primary care of 62/100 000 is likely to be an underestimate, as smaller practices with fewer cases were more likely to participate, but nevertheless is similar to school surveys reporting 70/100 0008 and health professional reported studies9 reporting 47.9/100 000, but substantially lower than self-reported community surveys reporting 570/100 000.3
The association of cases with practices in less deprived areas could reflect differing underlying prevalence rates, but might also indicate a difference in consulting behaviour.
Acknowledgments
The authors wish to thank Dr Madge Vickers, Jeanette Martin, and Nicola Fasey of the GPRF for their support and assistance with this study as well as all the practice nurses participating in the survey.
Footnotes
-
Funding: the research was funded by a grant from the Community Fund
-
Competing interests: none declared