Article Text

Abstract
Objective To explore perspectives among patients and rheumatologists on glucocorticoid (GC) therapy and European League Against Rheumatism (EULAR) recommendations on the management of systemic GC therapy in order to enhance implementation of the recommendations.
Methods Rheumatologists (from eight countries) and patients (from five countries) acquainted with GCs participated in separate meetings, during which positive and negative aspects of GC therapy were discussed and possible adverse events (AEs) were ranked for importance; in addition participants were asked to evaluate the published EULAR recommendations. The reports from these meetings and themes related to implementation of the recommendations were discussed during an international forum of the experts who had formulated the recommendations and patient participants.
Results In all, 140 patients (78% women; mean age 53 years; 61% patients with rheumatoid arthritis) and 110 rheumatologists (mean work experience 15 years) participated in the meetings. Osteoporosis, diabetes and cardiovascular diseases were ranked among the five most worrisome AEs by patients and rheumatologists. In both groups, there was agreement with most of the recommendations; the recommendations on GC information cards and GC use during pregnancy scored lowest. Ideas to improve implementation of the recommendations and a research agenda were generated.
Conclusion The patient and rheumatologist views on GCs corresponded to a large extent, reflected by concerns in both groups about osteoporosis, diabetes and cardiovascular diseases. Specific problems with the EULAR recommendations were identified and addressed to improve their implementation. This exercise shows that patient and rheumatologist perspectives should be included early in the process of formulating recommendations.
Statistics from Altmetric.com
Introduction
Glucocorticoids (GCs) have been widely used in inflammatory rheumatic diseases for almost six decades.1 2 The demonstration of disease-modifying potentials of low-dose GCs in rheumatoid arthritis (RA) has resulted in renewed discussion about risks and benefits.3,–,9 This debate led to the formation of the European League Against Rheumatism (EULAR) Task Force on GC therapy, which has published articles about nomenclature10 and safety11 of GC therapy. The Task Force concluded that low-dose GC therapy (≤7.5 mg prednisone or equivalent) is relatively safe, but that recommendations on management of GC therapy were lacking. Subsequently, EULAR evidence-based recommendations on the management of systemic low-dose to high-dose GC therapy in rheumatic diseases have been developed (table 1).12
European League Against Rheumatism (EULAR) evidence-based recommendations on systemic glucocorticoid therapy in rheumatic diseases12
Patients are also aware of the benefits and the risks of GC therapy, reflected in serious concerns about adverse events (AEs) and sometimes even refusal to take GC treatment.13,–,15 The perceptions and preconceptions of rheumatologists and patients can affect the usage of medication, including GC therapy,16 and may influence the implementation of the EULAR recommendations. Therefore, the aim of this study was to explore the general opinion of patients and rheumatologists towards GC therapy and the published recommendations in order to produce additional useful information for improving their implementation.
Methods
Scenario and questionnaire
To identify the opinions of patients and rheumatologists towards GC therapy and the EULAR recommendations, separate meetings were arranged for patients and rheumatologists in the rheumatology departments of university medical centres (see tables 2 and 3), following an agreed protocol devised for the purpose. In each country, one convenor organised the meetings for patients and rheumatologists. Each meeting started with a group discussion, in which positive and negative aspects of GC therapy were discussed, guided by a list of items to be raised by the convenor if they did not arise spontaneously. This included all the groups of AEs previously considered by the Task Force.11 Subsequently, the participants were asked to rank the 10 most worrisome AEs of GCs from a list with 37 items. The third task for the participants was to evaluate the published recommendations on the management of systemic GC therapy and rate their importance using a numerical rating scale (0–10). Medical terms were translated into patient-friendly wordings and the language of the host country was used.
Characteristics of patients (n=140)
Characteristics of rheumatologists (n=110)
Participants
Outpatients acquainted with chronic GC therapy were invited to participate in this project and to attend a patient meeting focused on GC therapy. Current use of GCs was not compulsory; but most patients used or had used GCs. Also rheumatologists from the participating university medical centres and surrounding non-university hospitals were invited by experts from the Task Force to attend the meetings (or sometimes to complete the questionnaire independently). No special preparation for the meetings was asked of the participants.
Data collection and interpretation
During the meetings discussion notes were taken of positive and negative aspects of GC therapy raised by the participating groups. These notes and scores on the questionnaire were summarised for each country.
During a Task Force meeting the results from the different countries were presented and discussed by rheumatologists and five patient participants. A consensus was reached on the broad themes that emerged, which is incorporated in the discussion section of this report and a research agenda was formulated.
Data analyses
Dosages of different GC preparations were converted into milligrams prednisone equivalent. Ranking scores for the 10 most worrisome AEs (the most worrisome AE received 10 points; the least worrisome 1 point) were summed for each country. In order to get equal weights for each country, we corrected for the different numbers of participants per country. Therefore the total score for AEs per country was recalculated in percentages of the total score for all AEs of all countries per group, being 100%. In the same way, the total agreement scores of the individual recommendations were corrected for the different number of participants per country. Also, analyses with equal weight for each participant were performed to check whether the way of analysing described earlier would lead to over-representation of countries with few participants. Data were analysed using SPSS V15.0 (SPSS, Chicago, Illinois, USA).
Results
Seven rheumatology departments of university medical centres from European countries and one from the USA took part in this study. Patients were recruited from five European countries. The characteristics of 140 patients and 110 rheumatologists involved are shown in tables 2 and 3. A total of 68% of patients were currently taking low-dose GC therapy (≤7.5 mg prednisone or equivalent), although some of them had experience with medium to high-dose therapy.10 The most frequent diagnosis was RA (61%), followed by systemic lupus erythematosus (11%). Although participating groups were encouraged to complete the entire exercise, which included group discussion, ranking of AEs and evaluation of the recommendations, this was not possible for the Slovakian patients. Because of long distances to the hospital, those patients were asked to complete the questionnaire after follow-up visits with their rheumatologists, instead of attending a separate meeting.
Group discussions on the effects of GC therapy
Meetings started with open-ended group discussions, in which participants introduced their ideas or experiences with GC therapy. During the patient meetings in particular, this resulted in statements, varying from very positive to negative. Examples of positive statements were as follows:
Five years ago I wasn't able to do anything. Then I started prednisone treatment and I noticed the effect within a day!
I live by virtue of it, would have died without.
When you get it, you feel like you're on top of the world. There's something happening in your body!
Negative feelings were also expressed by patients:
I do not notice any positive effect at all and I have joint inflammations all the time.
I don't have my own face anymore. (Concern about moon faces.)
All of a sudden I would find myself crying in front of the television. (Concern about mood disturbances.)
I frequently feel I have to ‘defend’ myself for my use of GC therapy, not only in front of family and friends but also to doctors such as the general practitioner.
These tablets taste bitter!
Ranking of most worrisome AEs of GC therapy
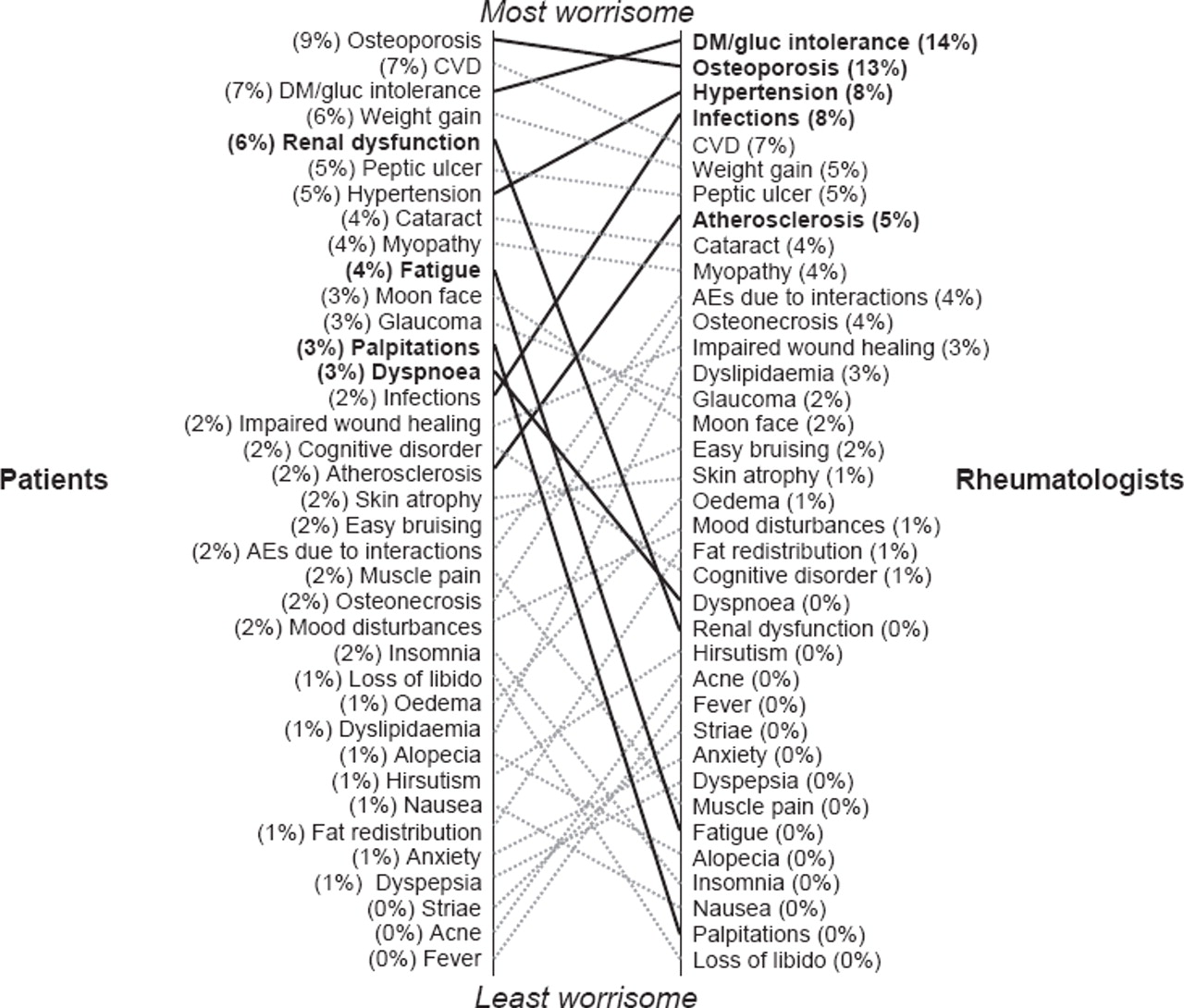
Next, the participants were asked to pick the 10 most worrisome AEs out of a list of 37 possible AEs of GC therapy and rank them from most worrisome (10 points) to least worrisome (1 point). In general for both groups the chosen most worrisome AEs matched reasonably; osteoporosis, diabetes and cardiovascular diseases were ranked within the five most worrisome AEs by patients and rheumatologists (figure 1; supplementary figures 1–3). These three items received 23% of the total patient scores and 34% of the total rheumatologist scores. Moreover, in the rheumatologist group, the five most worrisome AEs got 50% of the total scores compared to 35% in the patient group, indicating that the patient scores were more distributed over all AEs. Analyses with equal weight for each participant gave similar results as analyses with equal weight for each country (data not shown).

Most worrisome adverse events. All adverse events ranked by patients (left) and rheumatologists (right). Scores are corrected for the different numbers of participants per country and expressed as percentages of total score per group (the scores per country were recalculated in percentages of the total score of all countries per group, being 100%). Discordant scores, defined as a difference of at least 3%, are depicted in bold type. CVD, cardiovascular disease; DM, diabetes mellitus; gluc, glucose.

Mean scores of recommendations. Mean scores of the European League Against Rheumatism (EULAR) evidence-based recommendations on the management of systemic glucocorticoid therapy in rheumatic diseases, including results of all participating countries. Scores are corrected for the different numbers of participants per country. Each spoke represents (a part of) a recommendation (see table 1).

{kind=link}
{kind=link}
{kind=link}
Mean scores of recommendations. Mean scores of the European League Against Rheumatism (EULAR) evidence-based recommendations on the management of systemic glucocorticoid therapy in rheumatic diseases. Scores are corrected for the different numbers of participants per country. Each spoke represents (a part of) a recommendation (see table 1). Scores for participating countries are visualised in coloured lines.
Concordance and differences in scoring of both groups are shown in figure 1. Striking differences were found for some AEs: patients scored renal dysfunction, fatigue, palpitations and dyspnoea as more worrisome compared to rheumatologists. However, rheumatologists scored diabetes, osteoporosis, hypertension, infections and atherosclerosis as more worrisome than patients.
Evaluation of the published EULAR recommendations on the management of systemic GC therapy in rheumatic diseases
Participants were asked to evaluate the EULAR evidence-based recommendations on the management of systemic GC therapy (table 1), using numerical rating scales from 0 to 10. There was agreement with most of the recommendations, indicated by the mean total score for all recommendations of 8.1 for patients and 7.8 for rheumatologists (figures 2 and 3; supplementary figures 4 and 5). The three (parts of) recommendations receiving the lowest scores, expressed as combined mean score of both groups and most criticism will be presented. These are recommendations 1c, 8 and 9 with mean scores of 7.0, 7.7 and 5.4, respectively.
Recommendation 1c
Recommendation 1c states: ‘If GCs are to be used for a more prolonged period of time, a ‘GC card’ is to be issued to every patient, with the date of commencement of treatment, the initial dosage and the subsequent reductions and maintenance regimens’.
Although most patients and rheumatologists in general agreed with the potential value of a GC information card, there were different ideas about the presumed purpose of the card and of this recommendation. Even though such a card is routinely issued in the UK, the feasibility of implementing this recommendation in other countries was doubted. Rheumatologists noted that issuing a GC card and keeping it updated would be time consuming and thus difficult to implement. Comments ranged from ‘this will be very useful’ to ‘we already register GC dosages in the medical files’. Patient attitudes towards GC cards also varied. Some definitely preferred to have such a card for emergency situations, especially when travelling, possibly even for all medications, while others did not see the value of it.
Recommendation 8
Recommendation 8 states: ‘All patients on GC therapy for longer than 1 month, who will undergo surgery, need perioperative management with adequate GC replacement to overcome potential adrenal insufficiency’.
Although most rheumatologists agreed with this recommendation, many of them mentioned the lack of scientific evidence for this item and the need for evidence-based perioperative GC schemes. One point of discussion was whether there is an increased risk of impairment of wound healing and infections at low dosages. Patients mentioned the advantage of taking additional GCs in the postoperative period, since it improved their disease control and hence accelerated postoperative recovery in their experience.
Recommendation 9
Recommendation 9 states: ‘GCs during pregnancy have no additional risk for mother and child’.
This recommendation was scored lowest of all by patients and rheumatologists. Patients noted their lack of knowledge and were rather suspicious towards the use of any medication during pregnancy. A substantial group of rheumatologists disagreed with the decisiveness of this recommendation. In their opinion GCs are not completely safe during pregnancy and safety depends on the dosage. They felt that GCs should only be prescribed if necessary and that GCs in general are associated with lower risks during pregnancy compared to other antirheumatic therapy.
Discussion
Group discussions on the effects of GC therapy
Many patients offered their own experiences with the use of GCs, of which some were surprising. For example, the clear negative attitude towards the patients' GC therapy from close family, friends and doctors (except the prescribing rheumatologist), reflected the poor image of this class of drugs.13,–,16 Many patients felt that they frequently needed to defend themselves for their use of GCs; they did so by explaining the medical need for these drugs.
Ranking of most worrisome AEs of GC therapy
This exercise especially emphasised the differences between the perspectives of patients and rheumatologists. Rheumatologists integrated their clinical and epidemiological knowledge about the frequency of occurrence of a specific AE with their ideas about the potential clinical impact of various AEs. Therefore, AEs known to be very rare, although serious, were in general not scored as very worrisome. Patients, however, weighed the severity of an AE largely without knowledge of the chance of occurrence and integrated in the weighing their own experiences with GCs and their own concerns about this medication. As previously reported in the literature, very rare AEs considered by them to be serious, such as renal dysfunction, or AEs experienced by themselves or acquainted patients, were scored as very worrisome.17 This influenced the given answers to our questions and the outcomes of this exercise.
Evaluation of the published EULAR recommendations on the management of systemic GC therapy in rheumatic diseases
Most comments concerned the appropriateness of the recommendations for higher doses of GC therapy. The literature search performed for the recommendations yielded almost exclusively studies on low to medium dosages, indicating that the recommendations are appropriate for this dose range.10 12 General linguistic problems were also addressed and the formulation of some recommendations was commented upon. For instance, some rheumatologists noticed that some recommendations were formulated more like a statement than a recommendation. Statements usually correspond with a strong advice and, in their opinion, this did not fully fit the purpose of providing (just) a tool for better use and management of GC therapy. This indicated that the phrasing as a statement could have resulted in the higher levels of disagreement for recommendations 1c, 8 and 9.
Another frequently made comment was that several recommendations, although agreed upon in principle, were considered vague in terms of implementation. For instance, almost all participants agreed that information should be given regarding GC management (recommendation 1b), but there was no consensus on what information to give. Patients, in addition, highlighted that they would not be able to absorb all information at one visit before start of treatment. The same problem applied to recommendation 5 on monitoring of potential AEs of GC therapy. Evidence-based guidelines on which AEs to monitor, how to monitor them and in what frequency are needed.
However, most of the recommendations received a reasonable level of agreement and were endorsed by most of the rheumatologists and patients. The content of a few recommendations was more subject to discussion. The three recommendations receiving the lowest scores and most criticism are presented in the results section of this article. In response, suggestions for implementation are given below.
Suggestion for implementation of recommendation 1c on the use of GC cards
Many patients on GC therapy are unaware of the need for GC action in emergency situations and during intercurrent illness.18 In the UK, the use of a small GC card has been successfully implemented in daily practice; the pharmacist who hands the medication to patient fills it out. Although the value of this arrangement has not been studied, it can provide important information in case of emergencies and in consultations with other doctors. Good patient education and doctor information about the purpose of GC cards and discussion with pharmacists on how to increase feasibility could improve the use of GC cards.
Suggestion for implementation of recommendation 8 on perioperative GC schemes
Although further research is needed to obtain information on the incidence of adrenal insufficiency and adequate ways of preventing it, the key message of this recommendation is awareness of the possibility of adrenal insufficiency.19 20 If there is a risk of adrenal insufficiency, the benefit of adequate GC replacement seems to outweigh the risk. The issue of whether improved perioperative disease control (using GCs) aids postoperative recovery requires further investigation.
Suggestion for implementation of recommendation 9 on use of GCs during pregnancy
Available research shows that rheumatic diseases can increase the risk of pregnancy problems and that GC therapy has no proven additional risk. The recommendation should be seen as a rule of thumb for low-dose to medium-dose GC therapy with very low risks of AEs for mother and child, outweighing the risk of stopping clinically indicated GC therapy, especially compared to other immunosuppressive treatments.21 22 In the setting where immunosuppressive therapy is indicated during pregnancy, GCs would be the safest option.
General lessons from the exercises
The group discussions and evaluations showed that perspectives of patients and rheumatologists correspond to a large extent, reflected by high concerns about osteoporosis, diabetes and cardiovascular diseases in both groups. Their views on some of the published recommendations differ; this could influence acceptance and thus implementation of recommendations. The comments clearly indicated that sometimes literature to support the recommendations is limited. Therefore, a research agenda was formulated (see supplementary table 1).
Ideally, patients and rheumatologists should be involved in the process of formulating recommendations from the start. Patients should be given the opportunity to introduce items that are of great importance for them, to refine the recommendations and to comment on drafts. The importance of phrasing should not be underestimated. For broad implementation it is necessary that most rheumatologists accept the recommendations, which could be impeded by linguistic problems, leading to misinterpretation. This could be prevented by promoting a preliminary evaluation of recommendations by patients and medical specialists of different countries before their final publication. This also would ensure that the recommendations do not conflict with national guidelines. The potential value of this extra step in the development of recommendations clearly has been shown by the results of the present exercise.
Nevertheless, it is not fully certain that the 250 participants in this project are a good representation of the whole international group of rheumatologists and patients with a rheumatic disease. Co-operation of more countries in this project would have been interesting, but because of feasibility this exercise was limited to five countries for patients and eight for rheumatologists. However, this is the first paper analysing in a systematic way the perspectives of rheumatologists and patients on glucocorticoid therapy.
Finally, it will be valuable to educate rheumatologists and patients on the recommendations. For rheumatologists it is essential that the recommendations are being correctly interpreted in order to promote implementation. At the same time patients appreciated being informed about benefits and risks of GC therapy (recommendation 1a and 1b), although it was felt that this information should preferably be given over time, in small steps.
Conclusion
The views of patients and rheumatologists on GCs corresponded to a large extent, reflected by concerns in both groups about osteoporosis, diabetes and cardiovascular diseases. Specific problems with the EULAR recommendations were identified and addressed to improve their implementation. This exercise shows that the perspectives of patients and rheumatologists should be included early in the process of formulating recommendations.
Acknowledgments
We would like to thank Ilse Masselink, occupational therapist at the University Medical Center Utrecht, The Netherlands and Greet Esselens, nurse specialist at University Hospitals KU Leuven in Belgium for their involvement in organising and chairing the patient meetings.
References
Supplementary materials
Web Only Data ard.2009.114579
Files in this Data Supplement:
Footnotes
-
Funding This exercise was financially supported by EULAR (‘Implementation of the recommendations on the management of systemic glucocorticoid therapy in rheumatic diseases, including patients’ perspectives'; project 2007–07).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.