Article Text

Abstract
Objectives Susceptibility to spondyloarthritis (SpA) is largely genetically determined. To understand increasingly complex genetic associations, one approach is to study epistasis or genetic interactions. Several associations between HLA antigens and SpA including HLA-B27 have been reported. In this study, we investigated epistasis between common HLA class I risk antigens in ankylosing spondylitis (AS), the most typical form of SpA.
Methods In 154 patients with AS and 5584 controls, HLA class I antigens were analysed for association with AS. Biological interaction was analysed by investigating whether the effects of the risk factors combined departed from additivity.
Results Apart from the association with HLA-B27, we found an association between HLA-B60 and AS (OR 1.8; 95% CI 1.2 to 2.8). This was confirmed in a meta-analysis (OR 2.2; CI 1.8 to 2.8). While 18.2% of AS patients had both HLA-B27 and HLA-B60, this combination was found in only 0.4% of controls. Using AS patients without HLA-B27 and HLA-B60 as a reference, the relative risk (RR) for disease in HLA-B27−/HLA-B60+ patients was 1.2 (95% CI 0.3 to 4.1). For HLA-B27+/HLA-B60− the RR was 69 (95% CI 40 to 111) but increased to 342 (95% CI 147 to 708) in HLA-B27+/HLA-B60+ patients. For the interaction, the relative excess risk due to interaction was 251, the attributable proportion was 0.8 and the synergy index was 4.7. The interaction was confirmed in an independent cohort.
Conclusions There is a strong epistatic interaction between HLA-B60 and HLA-B27 in AS susceptibility. As a result, individuals with the HLA-B27+/HLA-B60+ genotype are at a very high risk of developing AS.
- Ankylosing Spondylitis
- Gene Polymorphism
- Epidemiology
Statistics from Altmetric.com
Studies of disease concordance in twins and families of patients with ankylosing spondylitis (AS), the most typical form of spondyloarthritis (SpA), show that susceptibility to disease is largely due to genetic factors. As for many other common polygenic diseases in the last 2 decades, many new genetic risk factors have been discovered. At the moment, more than 10 genetic loci have been implicated in susceptibility to SpA1 and as technology to perform genetic studies is becoming more accessible it is likely that this number will continue to grow.
Unfortunately, little is known of the biological mechanisms underlying the genetic associations and genetic testing has yet to make an impact on the management of common polygenic rheumatic diseases. HLA-B27 testing is a clear exception. HLA-B27 as a risk factor for AS was discovered before introduction of molecular typing techniques. Although it is not known what the role of HLA-B27 is in pathogenesis, HLA-B27 testing may aid in the diagnosis of early stages of AS.2 Despite the fact that 85%–95% of Caucasian AS patients are HLA-B27 positive, only a small proportion of the 8% of HLA-B27 positive individuals in the population go on to develop disease. This indicates that although HLA-B27 is indeed important for the inheritance of AS, HLA-B27 by itself is not sufficient for development of disease.
To understand increasingly complex genetic association data, one approach is to study epistasis or interaction of genetic risk factors. This could provide insights into factors acting in concert in pathogenesis as well as identify individuals with a high risk of disease and those who are unlikely to develop the disease.
Modelling studies suggest that HLA-B27 is only a part of the genetic risk in the HLA region and various studies have been published on other HLA antigens as potential genetic risk factors for AS and SpA.1 ,3 ,4 Therefore, in this study, we investigated the presence of interaction between common HLA class I risk antigens in AS, the most typical SpA subtype with the strongest association with HLA-B27.
Patients and methods
Patients and controls
Cases consisted of 154 unrelated Caucasoid patients with AS diagnosed according to the modified New York Criteria attending the outpatient clinical of the Leiden University Medical Centre in Leiden, The Netherlands. Patients were found by retrospective review of patient files with HLA typing done for diagnostic purposes. All patients gave their consent to the treating physician. This non-interventional retrospective study was performed in accordance with the Dutch patient data protection law, the ‘Wet Bescherming Persoonsgegevens’.
The average age of AS patients was 43 years (range 16–66 years) and 71% of patients were male subjects (table 1). The control group consisted of 5584 randomly selected, unrelated, healthy Dutch Caucasoid blood donors.
Characteristics of 154 ankylosing spondylitis patients in the study
HLA typing
All patient and controls underwent full HLA class I typing by complement-dependent cytotoxicity tests or by DNA-based technique using sequence-specific oligonucleotides (Invitrogen, Washington, DC, USA). To use uniform data, the HLA results obtained by DNA techniques were translated to their serological specificities.5
Statistical analysis
Sample size calculations were based on detecting an association at an OR of 2.0 at a confidence of 95% and a power of 90% for an antigen with prevalence of at least 6%–12% in controls. In Dutch Caucasoid blood donors, the following HLA class I antigens have a prevalence of more than 6%: the HLA-A specificities A1, A2, A3 and A24; the HLA-B specificities B7, B8, B18, B27, B35, B44, B51, B60 and B62; and the HLA-C specificities Cw2, Cw3, Cw4, Cw5, Cw6 and Cw7.6 For such an association, the calculated number of controls and patients is around 5000 and 150, respectively. In theory, larger number of patients and controls are needed to detect associations for less frequent antigens or to detect less strong associations. Differences in antigen frequencies between patients and controls were analysed by χ2 test.
Meta-analysis
PubMed, Web of Science, EMBASE, COCHRANE, CINAAHL, ScienceDirect, Wiley and HighWire databases were searched for studies describing HLA-B60 (known as HLA-B*40:01) in cases or controls. The search term for PubMed was: ‘HLA-B60 OR HLA-B*4001 AND ankylosing spondylitis’. A study was included in the analysis if: (1) it described the frequency of HLA-B60 in cases of Caucasoid patients with AS according to the Modified New York Criteria compared with controls; (2) contained original data; (3) was published in a peer-reviewed journal; and (4) was written in English. Under the assumption that the strength of genetic association may vary between populations, the random effect model was used for meta-analysis. The overall or pooled estimate of OR was obtained by the DerSimonian and Laird method in the random effect model. The pooled OR in the meta-analysis was calculated by weighing individual ORs by the inverse of their variance. Statistical calculations were done using Meta-analysis In eXcel V.1.7.7
Interaction
For interaction between two antigens associated with AS, HLA-B27 and HLA-B60, patients and controls were recategorised into four strata: HLA-B27 positive or negative and HLA-B60 positive or negative. With the disease risk in the HLA-B27 negative and HLA-B60 negative stratum as the reference, the ratio of the increase of risk for disease, the relative risk (RR), for the stratum with HLA-B60 but not HLA-B27 was calculated. Similarly, the RR was calculated for patients with HLA-B27 without HLA-B60. The sum and product of the increases in RR together with the background effect were then compared with the RR of the combined joint effect, that is, the RR for AS with HLA-B27 and HLA-B60 relative to the RR of AS without HLA-B27 or HLA-B60. The estimated prevalence of AS in The Netherlands is 0.4%. This justifies a rare disease assumption thereby equating ORs with RRs.
Interaction, defined as the deviation from additivity, was evaluated by three measures: relative excess risk due to interaction (RERI), the attributable proportion (AP) due to interaction and the synergy index. These measures indicate significant interaction if they differ from 0 (RERI and AP) or 1 (synergy index). RERI can be interpreted as the excess risk due to interaction relative to the risk without exposure. AP is interpreted as the AP of disease that is due to interaction among persons with both exposures. The synergy index can be interpreted as the excess risk from exposure (to both exposures) when there is interaction, relative to the excess risk from exposure (to both exposures) without interaction. To obtain the parameter estimates needed for calculating these three measures, a logistic regression model was fitted.8 The Statistical Package for the Social Sciences (SPSS), V.18.0 (SPSS, Chicago, Illinois, USA), was used to analyse the data. In all tests, p values less than 0.05 were considered significant.
Results
In 154 patients with AS and 5584 controls, we studied the association with disease for common HLA class I antigens. As expected, more patients with AS were HLA-B27 positive as compared with controls (OR 81.4 (95% CI 49.8 to 134.3)) (table 2). In addition, an association was found for HLA-B60. In AS patients, 20.1% was HLA-B60 positive compared with 12.1% of controls. This gave a significant association with an OR of 1.8 (95% CI 1.2 to 2.8). In our cohort, no other association with common HLA antigens and AS was found (data not shown).
Associations of HLA-B27 and HLA-B60 with ankylosing spondylitis (AS) in Caucasians
Literature was searched for additional cohorts studying an association of HLA B60 with AS. Two articles were found describing a total of three Caucasoid populations of AS cases. One cohort was typed by PCR (HLA-B*40:01)9 and two by means of serology (HLA-B60).4 In all studies, HLA-B60 was a modest risk factor for AS with ORs between 2.2 and 2.9 in line with the results in our cohort (figure 1).

Meta-analysis of frequencies of HLA-B60 (HLA-B*40:01) in ankylosing spondylitis (AS) patients and controls from previously published studies and the present study. No, number of individuals. *In the article the same control population was used for the two patient populations; #data published in this article.
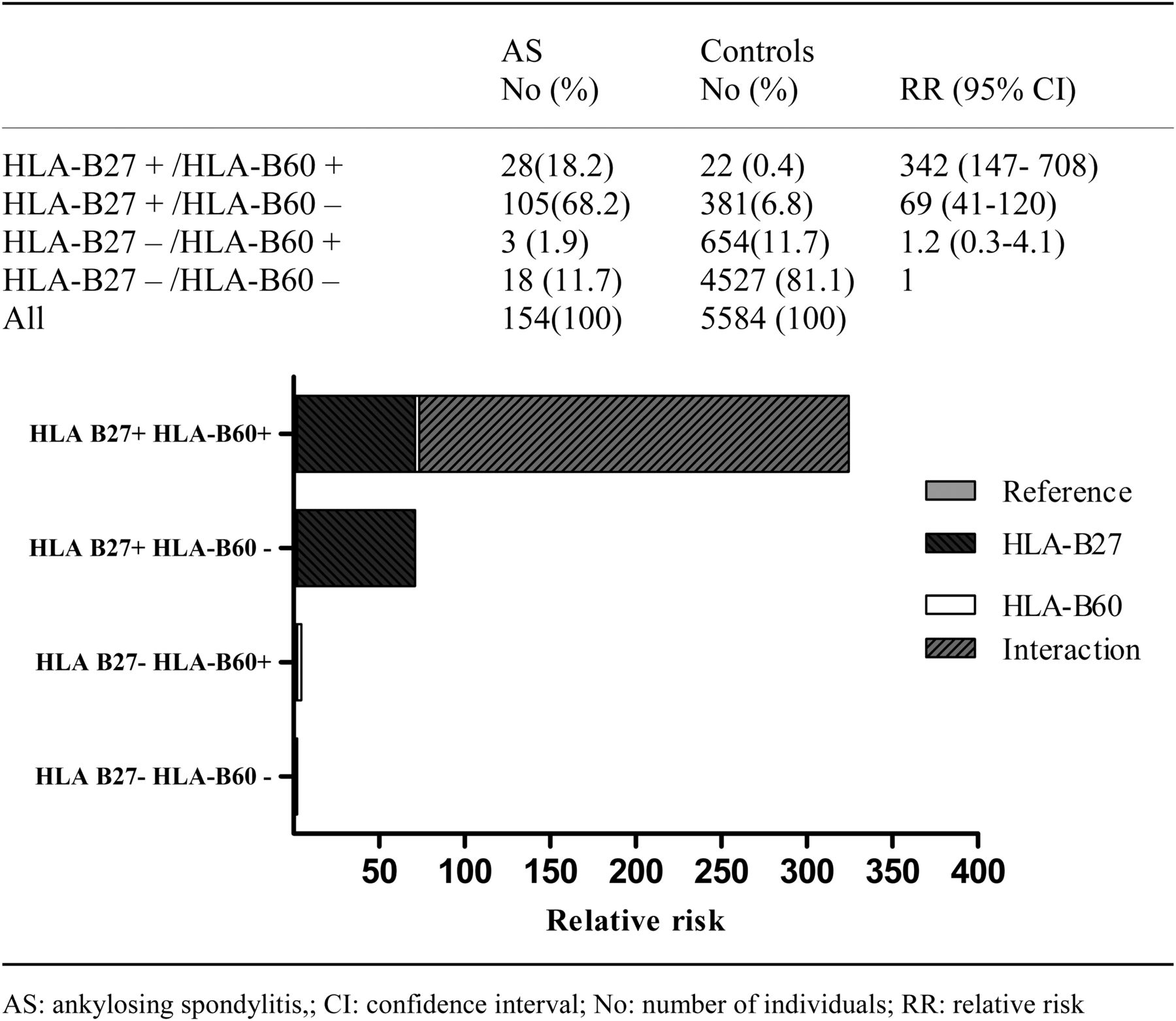
Next, we investigated the interaction between HLA-B27 and HLA-B60 in AS susceptibility. HLA-B27 positivity without HLA-B60 positivity was found in 68.2% of patients compared with 6.8% of controls. Remarkably, while 21.3% of patients carried both HLA-B27 and HLA-B60 (HLA-B27+/HLA-B60+), this combination was found in only 0.4% of controls. These data indicate that in contrast to HLA-B27 positivity alone, the combination of both HLA-B27 and HLA-B60 positivity is very rarely seen in controls.
With HLA-B27−/HLA-B60− as the reference, the RR for HLA-B27+/HLA-B60− was 69 (85% CI 41 to 120). The RR of HLA-B27−/HLA-B60+ was only 1.2 (95% CI 0.3 to 4.1). However, when a patient carried both HLA-B27 and HLA-B60 (HLA-B27+/HLA-B60+), the RR was 342 (95% CI 147 to 708).
In our study, the risk for AS in HLA-B27+/HLA-B60+ exceeded both the product and the sum of the risks in HLA-B27−/HLA-B60+ and HLA-B27+/HLA-B60− (figure 2). In a logistic regression model, HLA-B27+/HLA-B60+ and HLA-B27 positivity were both an independent risk factor for AS (p<0.0001) but HLA-B60 itself was not (p=0.8) (data not shown). Calculated interaction measures show a strong departure from additivity of the two risk factors combined (HLA-B27+/HLA-B60+) with a RERI of 251 (95% CI 102 to 400), AP of 0.8 (95% CI 0.7 to 0.9) and a synergy index (S) of 4.7 (95% CI 3.1 to 7.0) (figure 2).

{kind=link}
{kind=link}
Interaction between HLA-B60 and HLA-B27 in ankylosing spondylitis (AS) susceptibility with contribution of the different genes to the relative risk (RR) marked. No, number of individuals.
Subtracting data from of a published study of 284 British AS patients and 5926 controls9 followed by reanalysis confirmed the interaction between HLA-B27 and HLA-B60 (RERI 571 (95% CI 211 to 931), AP 0.7 (95% CI 0.6 to 0.9), S 3.6 (95% CI 2.2 to 5.9)). In this cohort, 11.3% of AS patients had the HLA-B27+/HLA-B60+ genotype compared with only 0.3% of controls. With HLA-B27−/HLA-B60− as the reference, the RR for HLA-B27−/HLA-B60+, HLA-B27+/HLA-B60− and HLA-B27+/HLA-B60+ were 3.4 (95% CI 1.0 to 12.4), 180 (95% CI 103 to 318) and 656 (95% CI 299 to 1440), respectively.
Discussion
Our study is the first to show epistasic interaction between two HLA antigens in AS susceptibility. HLA-B27 is the prototypical genetic risk factor for AS. In this study, HLA-B60 is confirmed as a modest risk factor for AS.
What is striking in the results is that the combination of both HLA-B27 and HLA-B60 positivity (HLA-B27+/HLA-B60+ genotype) was very rare in controls with a prevalence of just 0.4% while it was found in 18.2% of patients with AS. Moreover, having both HLA-B27 and HLA-B60 increased risk for AS far more than the effect of the two separate antigens would suggest. Indeed, strong interaction was demonstrated between HLA-B27 and HLA-B60.
The biological mechanism of the interaction is to be investigated. HLA-B27 is one of the best studied HLA antigens. The peptides presented by HLA-B27 have been studied extensively as well as the leukocyte receptors (eg, killer immunoglobulin receptor and leukocyte immunoglobulin-like receptors) that bind to different forms of HLA-B27. Based on analysis of known HLA ligands, the peptide binding motif of HLA-B60 is clearly different from HLA-B27.10 It is not known if HLA-B60 can form homodimers like HLA-B27 and as of yet there are no activating leukocyte receptors known that bind both HLA-B60 and HLA-B27.11
Both HLA-B27 and HLA-B60 are common HLA antigens with a phenotype frequency of more than 5%. A limitation of many studies, including this study, is that the sample size generally does not permit reliable analysis of less common HLA class I antigens. Therefore, additional associations and possible interactions within the major histocompatibility complex (MHC) locus remain to be analysed in SpA. For rare antigens, a large number of patients and controls is required and direct human leukocyte antigen (HLA) typing can be time consuming and therefore costly. An alternative to address the problem is HLA imputation from single-nucleotide polymorphism (SNP) data from genome-wide association studies.12
Although interaction measured on the additive scale has been argued to be better correlated with biological interaction than when measured on the multiplicative scale, several issues on the ideal way to calculate interaction continue to be discussed in the literature. For instance, Kalilani and Atashili have expressed concerns that directly substituting ORs for risk ratios in assessing interaction measured on the additive scale may sometimes give misleading results (for instance, when the incidence of a disease is high).13 Using their proposed modified formula for calculating measures of interaction, we recalculated the interaction effect for HLA-B27 and HLA-B60 and found similar results (RERI 99, AP 0.7, S 2.9).
A potential limitation of the results of our study is that in the Dutch population HLA-B60 appears to be more common than in some other Caucasian population. HLA-B60 is found in 12.1% of Dutch controls, in approximately 12% of Belgians, 6% of Austrians and 4.6% of French.14 This could mean that, while in our cohort the HLA-B27/HLA-B60 genotype was present in almost 20% of AS patients, this genotype may be less common in other AS populations. In addition, one study reported that HLA-B60 is a risk factor for HLA-B27 negative AS in Taiwan Chinese, suggesting that the effect of HLA-B60 on AS susceptibility is different in non-European patients.15
Early diagnosis of AS can be difficult. Studies have shown that on average the delay in diagnosis is more than 7 years after onset of symptoms. This means that for patients involved proper treatment is also delayed for many years. Currently several cohort studies are under way investigating new diagnostic algorithms and new technologies such as MRI scanning to improve this situation. For a disease where the genetic background is that important, genetic testing should play a more prominent role in diagnosis. HLA-B27 testing is helpful given that the prevalence of HLA-B27 is very high in AS but as less than 5% of the general population with HLA-B27 will develop AS, there is a need for improvement.
Our study shows that a detailed analysis may improve prediction based on HLA-B alone, underlining the need for appropriate cohorts to define genetic risk.
As the prevalence of the HLA-B27/HLA-B60 genotype is much lower in AS than for HLA-B27 alone, the diagnostic value of testing for the HLA-B27/HLA-B60 genotype is to be studied in a prospective study. Nevertheless, our study shows that as a result of the interaction between HLA-B60 and HLA-B27 individuals with the HLA-B27/HLA-B60 genotype are at a very high risk of developing AS. Therefore, finding an individual with the HLA-B27/HLA-B60 genotype should prompt a very careful analysis for symptoms and signs of SpA.
References
Footnotes
-
Correction notice This article has been corrected since it was published Online First. The author name Désirée M van de Heijde has been amended to Désirée M van der Heijde.
-
Contributors FAvG, WV, DLR: Data acquisition; FAvG, WV, DLR, REMT: Interpretation of data; FAvG, SB, TWJH: Conception and design of study; DvdH, REMT; all authors: Drafting the article or revising it critically for important intellectual content and final approval of the version to be published.
-
Funding REMT work is supported by an NWO-ZonMW VICI grant from the Dutch Organisation for Scientific Research.
-
Competing interest None.
-
Provenance and peer review Not commissioned; externally peer reviewed.