Article Text

Abstract
Objective: To determine the efficacy of epidural corticosteroid injections for sciatica.
Methods: Three epidural injections (two day intervals) of 2 ml prednisolone acetate (50 mg) or 2 ml isotonic saline were administered to patients with sciatica presumably due to a disk herniation lasting 15–180 days. Self evaluation was the main judgment criterion at day 20. Patients who recovered or showed marked improvement were considered as success. Pain measured by VAS, the SLR test, Schober’s test, Dallas pain questionnaire, and the Roland-Morris index were evaluated at days 0, 5, 20, and 35. Only analgesics were authorised, patients requiring non-steroidal anti-inflammatory drugs (NSAIDs) before day 20 were considered as failure.
Results: 42 patients were included in the control group (CG), 43 in the steroid group (SG). On an intention to treat analysis 15/42 (36%) in the CG and 22/43 (51%) in the SG (p=0.15) were considered as success (difference 15.5%, 95% CI (−5.4 to 36.3)). Among the 48 failures, 14 patients (6 CG, 8 SG) required NSAIDs, 3 (2 CG, 1 SG) required surgery, and 7 (3 CG, 4 SG) other treatments. On analysis according to protocol, in 74 remaining patients 12/35 (34%) in the CG and 22/39 (56%) in the SG (p=0.057) were considered as success (difference 22.1%, 95% CI (0.0 to 44.2)). For all secondary end points intragroup improvement with time was significant, but intergroup differences were not.
Conclusion: The efficacy of isotonic saline administered epidurally for sciatica cannot be excluded, but epidural steroid injections provide no additional improvement.
- sciatica
- epidural injections
- corticosteroids
- saline
- CG, control group
- CI, confidence interval
- LOCF, last observation carried forward
- NSAIDs, non-steroidal anti-inflammatory drugs
- SG, steroid group
- SLR, straight leg rising
- VAS, visual analogue scale
Statistics from Altmetric.com
- CG, control group
- CI, confidence interval
- LOCF, last observation carried forward
- NSAIDs, non-steroidal anti-inflammatory drugs
- SG, steroid group
- SLR, straight leg rising
- VAS, visual analogue scale
A lthough sciatica is usually caused by a mechanical abnormality, pathophysiological considerations provide a sound rationale for local corticosteroid treatment: sciatica due to disk herniation resolves within one month in 70% of non-surgically-treated patients,1 while after one year as many as 90% of patients are improved2; several lines of evidence suggest that biochemical factors may contribute to sciatica3; magnetic resonance studies have demonstrated postgadolinium enhancement consistent with an inflammatory response.4 There is also evidence that this treatment should be started early to prevent persistent nerve root pain due to peripheral and central sensitisation.5
Epidural corticosteroid injections have been used as part of the non-surgical treatment of sciatica for nearly half a century and are widely used in everyday clinical practice. Numerous open studies found that they were beneficial in about 65% of cases,6 but from 13 prospective, randomised, controlled studies,7–19 convincing evidence is lacking. The most recent study, and the most convincing from a methodological point of view, found no significant functional benefit.10 But in that study injections were repeated after three and six weeks only if needed and more than two thirds of the patients received just one or two injections. We aimed at testing the effectiveness of three epidural corticosteroid injections at 48 hour intervals as it is the recommended method in France for inhospital management of common sciatica.20
METHODS
Trial design
The study was a multicentre, randomised, double blind, controlled clinical trial, conducted in five rheumatology departments of university hospitals in France from October 1997 to January 2000. Randomisation took place after written informed consent and baseline information were obtained from the study participants. The randomisation was generated from a table of random numbers, stratified according to study centres and balanced after every four. Opaque prenumbered envelopes contained the assignments.
Patients
Inpatients referred for sciatica were eligible if they had a first or recurrent episode of sciatica lasting for more than 15 and less than 180 days. Sciatica was defined as the presence of pain in one leg, radiating below the knee, with at least one nerve root compression sign (reproduction of radicular pain by raising the leg or distal paraesthesia or sensory, motor, or reflex deficits compatible with the radicular pain). Pain intensity had to be >30 mm on visual analogue scale (VAS).
Patients were excluded if they had: (a) symptoms requiring early surgical treatment (severe motor weakness, cauda equina syndrome, hyperalgic sciatica); (b) structural spinal deformities (scoliosis greater than 40°, spondylolisthesis); (c) symptoms from causes other than a herniated nucleus pulposus; (d) received any spinal injection in the past month; (e) undergone low back surgery, chemonucleolysis, or nucleotomy. Patients who were pregnant or had a known allergy to corticosteroids, or were being treated with tricyclic antidepressant drugs or lithium, were also excluded. So were patients compensated for loss of work, or patients out of work for more than one year.
Treatment and concomitant treatment
The patients received three epidural injections (at two day intervals) of either 2 ml prednisolone acetate (50 mg) or 2 ml isotonic saline by a lumbar interlaminar approach using loss of resistance technique, without fluoroscopic guidance.
Lumbar exercises and other spinal injections were not authorised during the study. Non-steroidal anti-inflammatory drugs (NSAIDs) were authorised only 20 days after the first injection. Non-opioid analgesics, bed rest, mild lumbar tractions, and lumbar belts were authorised.
Blinding
The doctors making the assessments were not the same doctors as those giving the injections. So the patient and the assessing doctor were both unaware of the treatment received.
Outcome measure
The primary outcome was binary: success/failure of the treatment at day 20. Patients rated the perceived degree of overall improvement or deterioration on a descriptive four item scale (recovery, marked improvement, slight improvement, or worse). Patients rating the improvement as “recovery” or “marked improvement” were considered as success. Patients rating the improvement as “slight improvement” or “worse” were considered as failure, as were patients requiring NSAIDs between day 0 and day 20. Pain on a VAS, the straight leg rising (SLR) test, Schober test, French validated versions of the Dallas pain questionnaire,21 and the Roland-Morris index22 were also assessed.
Follow up
The patients were re-evaluated five days after inclusion (after the last injection, before leaving the hospital) and as outpatients 20 and 35 days after the first injection. Each patient was examined by the same doctor throughout the trial. At each visit, information on the use of analgesics and NSAIDs was recorded.
Sample size
We a priori assumed that the success rate would be 70% in the experimental arm and 40% in the control group, thus considering that a difference in the group achieving success lower than 30% would not be clinically relevant. Considering a two sided test with α level of 5% and power of 80%, we therefore planned to recruit 43 patients in each group.
Statistical analysis
Analyses followed a prespecified plan. Data were analysed according to the intention to treat principle. Missing data were given a value by applying the LOCF procedure (last observation carried forward). An analysis according to protocol was also performed for the main end point excluding (a) subjects wrongly included; (b) subjects for whom data were not collected at day 20; and (c) subjects non-compliant with the assigned treatment.
Success rates were compared by a χ2 test, and a 95% confidence interval around the difference in success rates was also estimated. For continuous end points, the mean change from the baseline was estimated and the treatment effect was defined as the difference between these changes. Confidence intervals of these treatment effects were then estimated.
Data analyses were carried out with SAS (SAS institute Inc, Cary, NC).
Ethical approval
The protocol was approved by the ethics committee of Tours.
RESULTS
Study group
Between October 1997 and December 1999, 85 patients were enrolled in the study, 43 patients in the steroid group (SG), 42 in the control group (CG). The baseline characteristics were similar in the two groups (table 1). The large majority of the injections (89.5%) were performed at the L4-5 level, 7% at the L3-4 level, and 3.5% at the L5-S1 level.
Baseline characteristics of 85 patients with sciatica randomly assigned to receive placebo (control) or epidural corticosteroids (steroids). Data are shown as means (SD) or number (%) of patients
Withdrawals
On analysis according to protocol 11 patients were excluded (fig 1): two did not satisfy the inclusion criteria, four did not receive the three epidural injections (one because of failure after the second injection, one for cauda equina syndrome after the first injection, two for side effects after the first or second injection), five were lost from follow up before day 20 (three for failure).

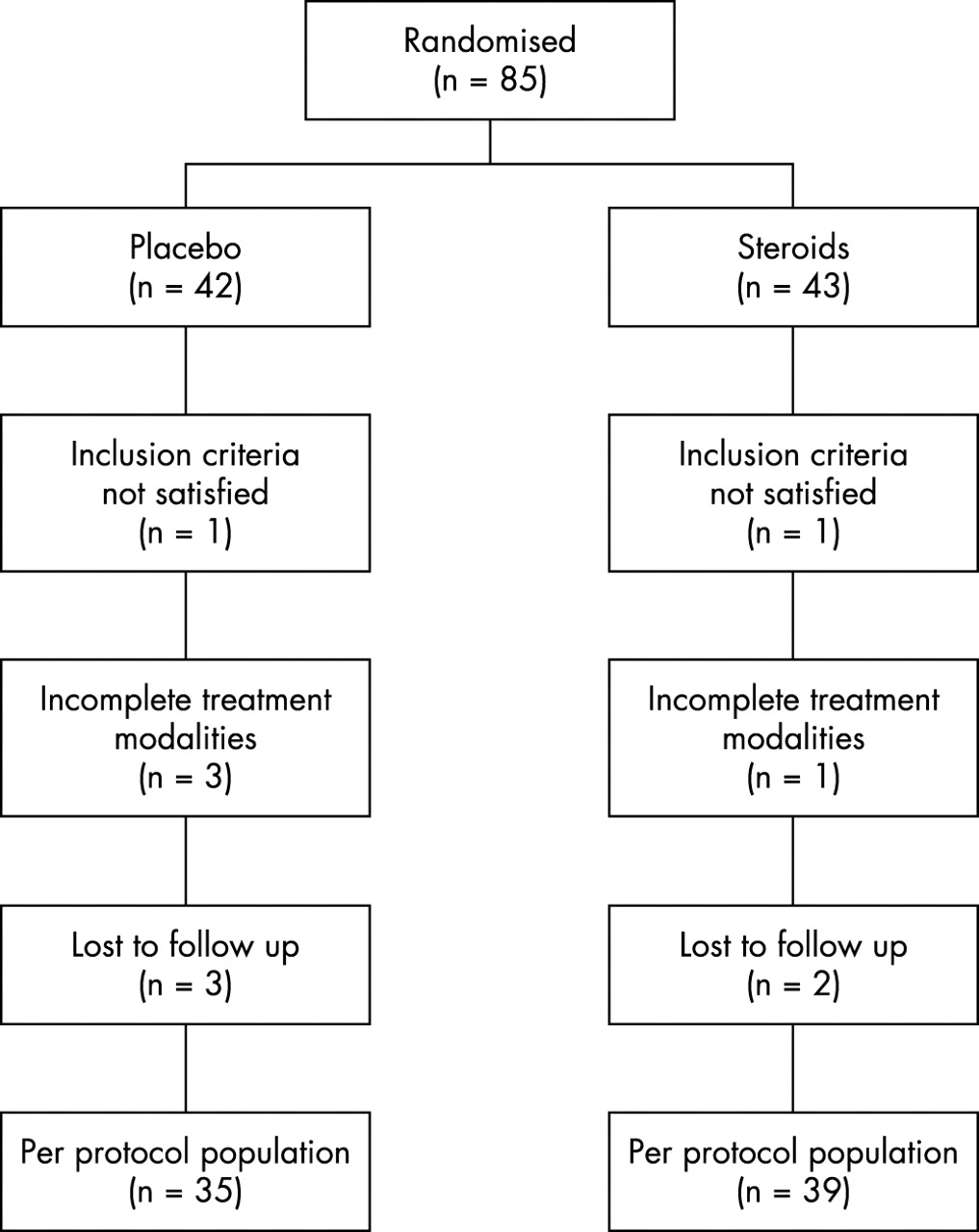{kind=link}
Trial profile.
Complications
Clinically significant side effects occurred in three subjects in the CG and two patients in the SG (p=0.676): headache in the days after injections in four cases (two in each group), thoracic pain during the injection in one case (in the CG).
Response to treatment
On an intention to treat analysis at day 20 the groups did not differ significantly with respect to the primary outcome: 15/42 (36%) patients in the CG and 22/43 (51%) in the SG (p=0.15) were considered as success (difference 15.5%; 95% confidence interval (CI) for the difference −5.4 to 36.3). We calculated the number of patients needed to treat to achieve one more success with epidural corticosteroids than with saline; this was 6.5. Among the 48 failures, 14 patients (six in the CG and eight in the SG) required NSAIDs, three required surgery (two in the CG and one in the SG), two required chemonucleolysis (one in each group) and five (two in the CG and three in the SG) other routes of corticosteroids administration.
At the end of the study (day 35), 20/42 (48%) patients in the CG and 21/43 (49%) in the SG (p=0.91) were considered as success (difference 1.2%; 95% CI for the difference −20.0 to 22.5).
On analysis according to protocol, at day 20, in the 74 remaining patients, 12/35 (34%) in the CG and 22/39 (56%) in the SG (p=0.057) were considered as success (difference 22.1%; 95% CI for the difference 0.0 to 44.2).
For secondary end points, intragroup improvement at day 20 was seen for pain on a VAS (mean (SD): CG −17.4 (28.5) mm, p<0.001 and SG −28.3 (28.8) mm, p<0.001), but there was no significant difference between the two groups (p=0.082). The same qualitative conclusions were drawn for other secondary end points (table 2) such as the Schober test, SLR test, daily living, work-leisure and anxiety-depression subscales of the Dallas pain questionnaire, Roland-Morris index: intragroup improvement with time was statistically significant, but intergroup differences were not. At day 5, just after the third injection (table 3), and at day 35, at the end of the study (table 4) there was a marked improvement from baseline for all secondary end points, but no significant difference between the two groups. Surprisingly, the only significant difference between the two groups at day 20 and day 35 was the social interest score of the Dallas pain questionnaire.
Secondary end points 20 days after enrolment and change from baseline values according to treatment group
Secondary end points five days after enrolment and changes from baseline values according to treatment group
Secondary end points 35 days after enrolment and changing from baseline values according to treatment group
DISCUSSION
In this randomised double blind clinical trial we administered three epidural injections (at two day intervals) of prednisolone or isotonic saline to patients with sciatica presumably due to a herniated nucleus pulposus. For the main judgment criterion (self evaluation at day 20) as for secondary end points, intragroup improvement with time was statistically significant, but intergroup differences were not.
Numerous open studies of epidural corticosteroid injections for sciatica due to disk herniation found a beneficial effect in about 65% of cases.6 Thirteen prospective, randomised, controlled studies7–19 have been carried out, but comparisons among them are difficult because: (a) only six studies included more than 20 patients in each group; (b) symptom duration ranged from a few weeks to several months or years; (c) other differences included the volume injected, the injection route, and the number of injections. Of these 13 studies, five found that epidural corticosteroid injections were effective,8,9,12,15,19 with duration of pain relief ranging from seven days to one month, and no effect beyond one month. None suggested that the injections were associated with a reduced need for surgical treatment. In the remaining eight randomised studies, there were no differences between the group treated by epidural corticosteroids. and the CG.7,10,11,13,14,16–18 Not surprisingly the most recent study is also the one with the best methodology,10 but failed to find a difference in favour of corticosteroids. Indeed this study did not find a difference in favour of corticosteroids on the primary outcome criterion (Oswestry score). However, the treatment used in this study differed from standard rheumatological practice in France in a number of ways, including the corticosteroid used (methylprednisolone 80 mg), the interval between injections (three weeks), and the number of injections (the mean number for each patient was only 2.1). The optimal number of injections has not yet been defined and some patients improve only after the second or third injection, but it is unlikely that increasing the number of injections beyond three provides any additional benefits.6 In France, for inhospital management of common sciatica, three corticosteroid injections at two day intervals are recommended.20
Only patients from the university hospital were included in our study, and this might have meant selection of patients with more serious disease. However, in these patients the use of conservative treatment, with drugs used to treat general symptoms, failed, and so epidural injections were justified. Patients were excluded if they had symptoms from causes other than herniated nucleus pulposus, and no imaging technique was required to identify the cause of sciatica. Possibly, the cause of the sciatica might have varied in the group, but at this stage of conservative treatment, imaging techniques are not required in common clinical practice.
The main judgment criterion we chose was particularly strong as success combined self evaluated recovery or marked improvement with no NSAID requirement before day 20. But for all other secondary end points (pain on VAS, Schober test, SLR test, Dallas pain questionnaire, Roland-Morris index) intergroup differences were not statistically significant.
Many patients with sciatica improve over time without specific treatment. However, the improvement of pain on VAS between baseline and day 5, although not significant (p=0.058), was relatively important (>20 mm in both groups) and probably not the effect of time as the mean duration of sciatica before injections was more than 40 days. The same tendency was seen at days 20 and 35. So it remains possible that both groups improved as a result of the epidural injection, and we cannot exclude the efficacy of epidural injections of any product, including isotonic saline through a volume or a “washout effect” within the epidural space. As in the Carette study,10 the placebo we chose may have some efficacy, and subcutaneous injections would probably be a better placebo.
The natural history of sciatica is such that most patients improve over time, which may hide the treatment effect. A study of nerve-root injections found a statistically significant difference between steroids and local analgesic (bupivacaine), but the patients involved were referred to a spine surgeon after failure of a complete course of non-operative management, so improvement over time was probably minimised, and the treatment effect easier to demonstrate.23 This kind of patient may be more suitable for testing the effectiveness of epidural corticosteroid injections.
Our study did not require fluoroscopic control of the site of injection. Epidurography to check the position of the needle has been recommended based on a report that 40% of injections done without epidurography missed the epidural space.24 But another study found that 93% of lumbar epidural injections were correctly placed within the epidural space when assessed by fluoroscopy.25 However, epidurography is not common practice, and in our study the epidural space was probably equally missed in the two groups. The volume injected is usually 1–5 ml, although some authors use 10 ml or more. In our study the volume injected (2 ml) was small, which may be not sufficient. But injections of 8 ml in the Carette study10 did not demonstrate additional efficacy. Our inclusion criteria did not require any imaging demonstration of the herniated disk, and the response to epidural corticosteroid injections may vary given the location of disc herniation (central, posterolateral, far lateral), the presence of underlying spinal stenosis, and the possibility of multilevel disc herniations. But in common practice, and in the absence of warning signs for serious conditions, imaging techniques such as computed tomography scan or magnetic resonance imaging are only recommended when surgical treatment is needed.
The observed difference on the main judgment criterion was not statistically significant. Possibly it might have been with a greater number of patients. But we studied the required number of patients for an expected difference of 30% between the compared treatments, and a smaller difference would have less or no clinical relevance.
In conclusion, we cannot exclude the efficacy of isotonic saline administered epidurally for sciatica, but epidural corticosteroid injections provide no additional improvement.
Acknowledgments
This study was supported by a grant from PHRC 1995, Ministry of Health, France.
REFERENCES
Footnotes
-
The authors are members of the spine group of the French Rheumatology Society.