Article Text

Abstract
Background: Rheumatoid arthritis (RA) is associated with increased cardiovascular mortality for reasons which are insufficiently understood. Chronic inflammation may impair vascular function and lead to an increase of arterial stiffness, an important determinant of cardiovascular risk.
Objective: To investigate the augmentation index (AIx) as a measure of arterial stiffness in patients with RA, free of cardiovascular disease or risk factors, by means of a matched cohort pilot study.
Method: Patients with a diagnosis of RA, aged 50 years or younger, were screened for the absence of clinical cardiovascular disease and risk factors, such as smoking, hypercholesterolaemia, hypertension, and excessive systemic steroid use. Suitable subjects were assessed by non-invasive radial pulse wave analysis to determine their AIx. These data were compared with those from healthy controls, matched closely for sex, age, mean peripheral blood pressure, heart rate, and height.
Results: 14 suitable patients (11 female; mean (SD) age 42 (6) years, mean RA duration 11 (6) years; mean C reactive protein 19 (15) mg/l, no clinical systemic rheumatoid vasculitis) and matched controls were identified. The RA group had a higher mean (SD) AIx and mean (SD) central blood pressure (BP) than the control group: AIx 26.2 (6.7) v 18.9 (10.8)%, p=0.028; mean central BP 91.3 (7.8) v 88.2 (8.9) mm Hg, p<0.0001, by two tailed, paired t test.
Conclusions: This preliminary study suggests that RA is associated with increased arterial stiffness and central BP, independently of clinically manifest cardiovascular disease or risk factors. This may contribute to the increased cardiovascular mortality in RA.
- arterial stiffness
- cardiovascular risk
- pulse wave analysis
- rheumatoid arthritis
- AIx, augmentation index
- BP, blood pressure
- CRP, C reactive protein
- DAS, disease activity score
- DPTI, diastolic pressure-time integral
- ESR, erythrocyte sedimentation rate
- LV, left ventricular
- PWA, pulse wave analysis
- PWV, pulse wave velocity
- RA, rheumatoid arthritis
- SPTI, systolic pressure-time integral
- Tr, time of return of the reflected wave
- VAS, visual analogue scale
Statistics from Altmetric.com
- AIx, augmentation index
- BP, blood pressure
- CRP, C reactive protein
- DAS, disease activity score
- DPTI, diastolic pressure-time integral
- ESR, erythrocyte sedimentation rate
- LV, left ventricular
- PWA, pulse wave analysis
- PWV, pulse wave velocity
- RA, rheumatoid arthritis
- SPTI, systolic pressure-time integral
- Tr, time of return of the reflected wave
- VAS, visual analogue scale
Most epidemiological studies report increased mortality for patients with rheumatoid arthritis (RA).1,2 As in the general population, cardiovascular disease is the single most common cause of death in rheumatoid patients, resulting in reported standardised mortality ratios ranging between 1.14 and 2.24. The reasons for this increased cardiovascular mortality are not clear. A number of the major cardiovascular risk factors are reported to be associated with RA, such as smoking3 and dyslipidaemias.4 RA manifestations, such as vasculitis,5 and RA treatment, such as corticosteroids6 have also been implicated in cardiovascular morbidity and mortality. Although epidemiological data have suggested an association between disease activity and cardiovascular mortality in RA,2,7 the cause of such a link is unclear. Specifically, few studies have looked directly at vascular structure and function in patients with RA.
Arterial stiffness is an independent risk factor of cardiovascular disease,8 and pulse pressure, a surrogate marker of increased arterial stiffness, is a powerful predictor of cardiovascular events.9 In addition increased vascular stiffness has important haemodynamic consequences. Large arteries are normally compliant structures, capable of buffering pressure changes that occur during the cardiac cycle to maintain constant tissue blood flow. The rate at which aortic pressure waves travel—the pulse wave velocity (PWV)—is determined in part by vascular stiffness. The forward going aortic pressure wave is reflected from the periphery and normally returns in diastole, thus serving to maintain coronary blood flow. As large arteries stiffen with age or disease processes, the PWV and the amplitude of the reflected wave both increase. The reflected wave then appears in the aorta during systole, augmenting central aortic pressure. Central peak systolic pressure is thus increased to a greater degree than peripheral systolic pressure as measured by conventional sphygmomanometry. The full arterial waveform therefore contains more information than is provided by the extremes of brachial BP and this includes information on arterial stiffness.10
Quantitative analysis of the arterial pressure waveform is now possible using the non-invasive technique of pulse wave analysis (PWA) by applanation tonometry.11 This allows accurate and reliable recording of radial and carotid pressure waveforms.12 By applying a validated transfer function, central aortic waveforms can be generated and central pressures determined.13–15 Augmentation of the central aortic pressure will thus provide an assessment of the stiffness of the arterial tree in its entirety and can be expressed numerically as the augmentation index (AIx).
We have assessed the function of large arteries in subjects with RA using PWA. This study aimed at determining arterial stiffness in RA, independently from other known cardiovascular risk factors.
PATIENTS AND METHODS
Patients
Subjects, aged between 18 and 50 years and attending the Royal National Hospital for Rheumatic Disease, Bath, UK, with a diagnosis of RA according to standard criteria,16 were invited to participate in this study, which had the approval of the Bath research ethics committee.
To determine the effect of RA on arterial stiffness in isolation, we applied the following exclusion criteria: a history of cardiovascular, cerebrovascular, or peripheral vascular disease; arterial hypertension or diabetes mellitus; hyperlipidaemia; renal or hepatic disease; and diseases characterised by chronic inflammation otherwise (for example, asthma, bronchiectasis, or inflammatory bowel disease). Furthermore, we excluded people, who presently smoked more than five cigarettes a day or had done so within the past 10 years; and patients, who were receiving 10 mg prednisolone equivalent a day or more; or who had received an intravenous or intramuscular bolus steroid injection within the previous six weeks.
Of 41 subjects with RA, aged 50 years or younger, 21 were suitable for further assessment, based on these exclusion criteria.
General assessment
Subjects were assessed for clinical characteristics of their RA (that is, disease duration, clinical features of systemic rheumatoid vasculitis, current medication, duration of morning joint stiffness in minutes, height, and patient derived visual analogue score (VAS) of current disease activity (0–100 mm)). Clinical assessment included further the examination of radial, carotid, and pedal arterial pulses; cardiac and carotid artery auscultation; and a 28 tender and 28 swollen joint count.17 Brachial blood pressure (BP) was determined in the left arm by a validated oscillometric technique (HEM-705CP; Omron Corporation, Japan).18 Venous blood for full blood count, erythrocyte sedimentation rate (ESR), C reactive protein (CRP), random plasma glucose, and serum cholesterol, and renal and liver function parameters was taken after PWA. Cases were removed from further analysis if the cardiovascular examination was clinically significantly abnormal, they had a BP>160/90 mm Hg as a mean of two measurements, a random plasma glucose of >7.8 mmol/l, a random serum cholesterol of 6.0 mmol/l, raised alanine aminotransferase (more than twofold), or a serum creatinine (>1.5-fold the upper limit of normal range). The modified disease activity score (DAS28),19 a validated composite score calculated from a 28 tender and 28 swollen joint count, ESR, and global health VAS (0–100 mm; 0 signifying best and 100 worst possible health), was determined, using the patient derived disease activity VAS instead of the global health VAS.20 Three of the 21 eligible patients had to be excluded from the study after the general assessment (aortic regurgitation, increased BP, and increased plasma glucose).
Pulse wave analysis
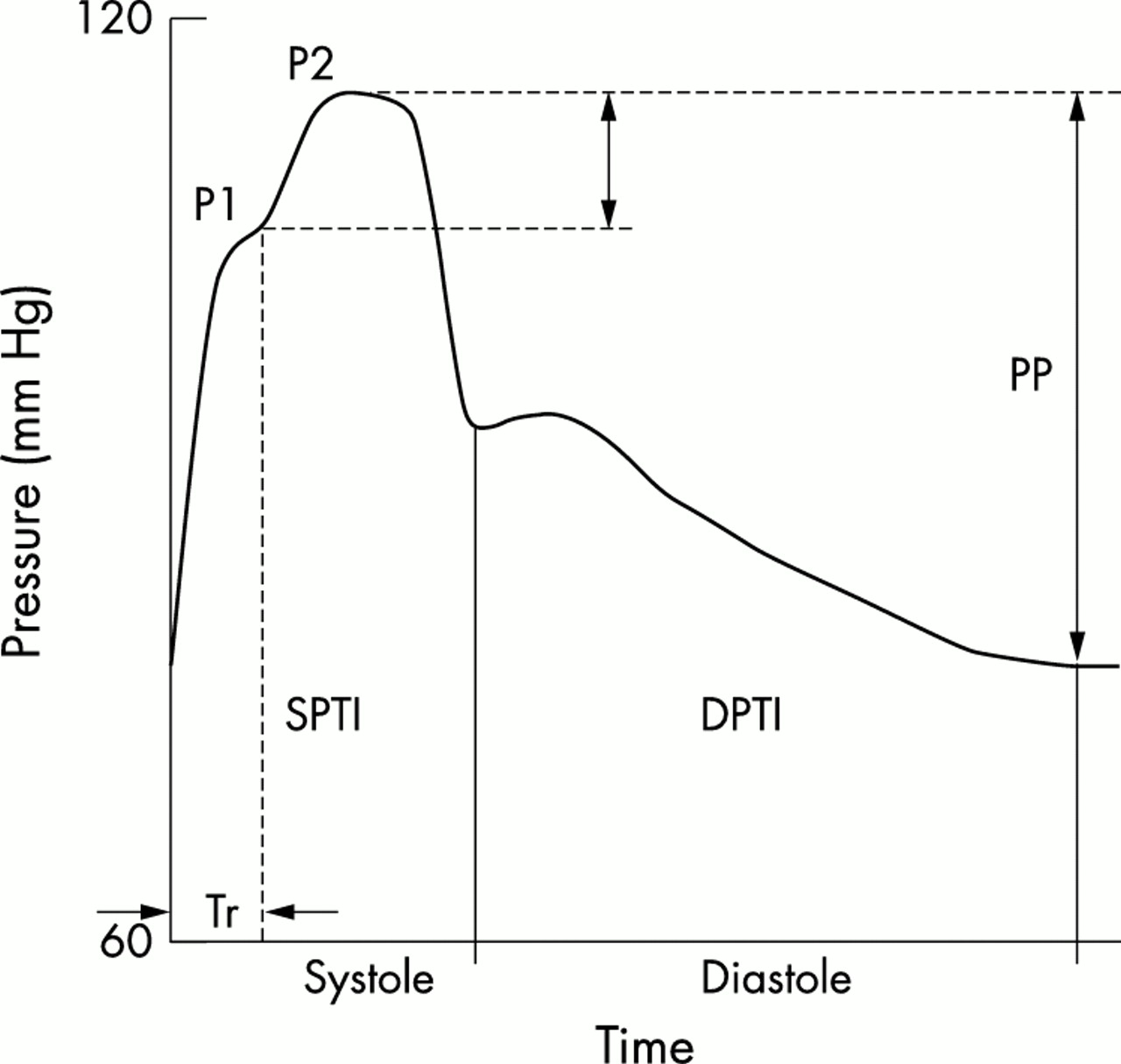
PWA of the patients with RA was performed by a single operator (RK) after appropriate training (by JRC) and as previously described.12 In brief, a hand-held tonometry probe (Millar pressure tonometer, PWV Medical, Sydney, Australia) was used to flatten the subject’s right radial artery. A laptop computer based PWA system (SphygmoCor, PWV Medical, Sydney, Australia) displayed a real time recording of the radial pulse waveform. After acquisition of 10–12 sequential waveforms, an averaged peripheral and the mathematically derived corresponding central aortic waveform, was generated. Recordings were discarded, if the systolic or diastolic variability of the pulse waveforms exceeded 5% or if the amplitude of the pulse waveform was less than 80 mV. The PWA software then further analysed the averaged central waveform for AIx, systolic and diastolic pressure-time integral (SPTI/DPTI), and time of return of the reflected wave (Tr) (fig 1). AIx was defined as the difference between the second (that is, augmented) and the first systolic pressure peak, expressed as a percentage of the pulse pressure. SPTI and DPTI represent the area under the curve during systole (reflecting systolic cardiac workload) and diastole, respectively. Tr was defined as the time interval between the foot of the pressure wave and the inflection point, which provides a measure of the time of travel of the reflected pulse wave. A mean of two readings was used for statistical analysis. Satisfactory PWA readings were acquired in 17 of the remaining 18 study subjects (intraclass correlation of duplicate measurements of AIx r2=0.852).

{kind=link}
Representative ascending aortic pressure-time curve, as determined by PWA. The AIx is defined as the difference between the second and first systolic peak (P2 − P1), expressed as a percentage of the pulse pressure. AIx is usually negative in young healthy subjects, about zero at the age of 35, and becomes increasingly positive thereafter. The SPTI and DPTI represent the area under the curve during systole and diastole, respectively. Tr is the time interval from start of systole until the beginning of the augmented wave—that is, the time of travel of the augmented wave.
Control subjects
Healthy controls were recruited from staff of the Royal National Hospital for Rheumatic Diseases and volunteers of the Wales Heart Research Institute in Cardiff. All participants gave informed consent. Inflammatory parameters, such as ESR and CRP, were not determined in the control group, unless inflammatory disease was clinically suggested.
Matching of cases and controls
We aimed to match the cases and controls for the following physiological variables, based on multiple regression analysis data of PWA data by Hayward and Kelly21: sex, mean peripheral arterial pressure (± 3 mm Hg), heart rate (± 3 beats/min), body height (± 4 cm), and age (± 5 years). Controls had to be the same sex as the patients. Cases were removed from statistical analysis if more than two of the other variables differed by more than the above ranges between the case and control. Matching of cases and controls was performed by one investigator (IRH), who was unaware of the results of the PWA.
Suitable matched controls were identified for 14 patients with RA. An average 1.0 (SD 0.8) of the variables mean arterial pressure, heart rate, height, and age was outside the target range for matching of cases and controls. All matched control subjects were clinically free of inflammatory disease.
Statistical analysis
The haemodynamic parameters AIx, SPTI, DPTI, and Tr of eligible cases and controls were compared by two tailed, paired t test, accepting a significance level of p<0.05. The correlation of AIx with the key RA parameters, disease duration, and the modified (28 joint) DAS28,19 was calculated as the Pearson’s correlation coefficient r2.
RESULTS
Characteristics of patients with RA and controls
The 14 patients had on average late and deforming RA (table 1). As indicated by the DAS28 values20 most had evidence of active disease, although mean CRP and ESR values were only modestly raised. Extra-articular RA features were noted in only two patients (both had rheumatoid nodules and one additional mild Sjögren’s syndrome). A minority was receiving regular low dose prednisolone (up to 7.5 mg/day).
Characteristics of the patients with RA. Values represent means unless stated otherwise
Table 2 shows the relevant matching and haemodynamic parameters of RA and healthy control subjects. There was no significant difference between the groups for age, heart rate, height, serum cholesterol, peripheral diastolic BP and peripheral pulse pressure by two tailed, paired t test. Statistically significant differences, however, were found for peripheral systolic and mean BP (table 2), both being higher in the control group.
Matching and haemodynamic parameters of patients with RA and matched healthy controls. Values represent means unless stated otherwise. p Values were determined by two tailed, paired t test. Only p values <0.05 are displayed
Pulse wave analysis
The mean (SD) AIx was significantly higher in the RA group than in the control group: 26.2 (6.7) v 18.9 (10.8)%, p=0.028. The mean central BP was also significantly higher in the RA group than in the controls: 91.3 (7.8) v 88.2 (8.9) mm Hg, p<0.0001, by two tailed, paired t test (table 2).
There was no significant difference between the other PWA parameters—that is, SPTI, DPTI, and Tr. There was a weak correlation of AIx with RA disease duration: r2=0.39, p< 0.03. In comparison, AIx did not correlate significantly with age or DAS28—that is, disease activity, of rheumatoid patients (r2= 0.11, p=0.24; r2=0.21, p=0.14, respectively). Similarly, correlation with ESR and CRP was poor (r2=0.17, p=0.18; r2=0.04, p=0.52, respectively).
DISCUSSION
RA is associated with increased cardiovascular mortality,1,2 for reasons that are insufficiently understood. There is evidence of increased prevalence of known cardiovascular risk factors, such as smoking and hyperlipidaemia, in patients with RA.3,4 The influence of the inflammatory process of RA itself on cardiovascular mortality has been suggested by epidemiological studies,2,7 but the mechanisms behind this are not clear.
Here we provide the first preliminary evidence that RA is associated with an increase in arterial stiffness as assessed by non-invasive PWA. Subjects with RA, selected for the absence of clinical cardiovascular disease and risk factors, had significantly increased augmentation of their central aortic pressure waveform, relative to their pulse pressure (AIx), and an increased mean central BP compared with that of well matched healthy controls.
These data indicate that non-invasively determined AIx and central BP may be a sensitive marker of early cardiovascular dysfunction in patients with RA. The AIx, as measured by PWA, reflects predominantly the stiffness of large and medium sized arteries.10 Abnormalities in these arteries may result from functional abnormalities, such as endothelial dysfunction, as well as structural changes, such as atherosclerosis. We have recently shown, both in animals and man, that the endothelium derived nitric oxide in part directly regulates large artery stiffness in vivo.22,23 Further support for this comes from studies in patients free of clinical vascular disease with conditions known to impair endothelial function, such as diabetes mellitus or hypercholesterolaemia, in which the augmentation index has been shown to be increased relative to control subjects matched closely for peripheral BP.24,25
There is good evidence, however, that arterial stiffness is not only a marker of cardiovascular dysfunction but also an independent risk factor for cardiovascular disease.8 Increased AIx and central BP can be expected to contribute to increased cardiac after-load, which may result in maladaptive functional and/or structural cardiac change, such as diastolic dysfunction and left ventricular (LV) hypertrophy, respectively, both known to be independent risk factors for cardiac morbidity and/or mortality.26,27 When the same method was used as in our study, AIx was shown to be correlated with LV mass in patients undergoing haemodialysis,28 and with relative wall thickness in healthy people.29 Interestingly, in the latter study the LV mass did not correlate with the AIx, suggesting that LV geometry may be affected by large arterial vessel stiffness before absolute ventricular size. Abnormalities in almost any cardiac structure have been described in patients with RA. However, even when the cardiac morphology is echocardiographically normal, subjects with RA who have no cardiovascular symptoms may show impaired diastolic function,30,31 indicating that diastolic dysfunction may be one of the first detectable cardiovascular abnormalities in this disease. As this study indicates, AIx as measured by PWA, may also be an early marker of cardiovascular dysfunction and future studies should examine its relationship with diastolic dysfunction in rheumatoid disease.
How might RA cause increased arterial stiffness? RA is characterised by chronic inflammation with an increase of acute phase response proteins, such as CRP and fibrinogen. Both these proteins have been shown to be predictors of future cardiovascular and cerebrovascular events in apparently healthy man32,33 and are strongly suspected to have a pathogenic role in cardiovascular disease.34 Acute systemic inflammation has been shown to lead to reversible endothelial dysfunction in man using forearm blood flow plethysmography.35 Furthermore, chronic systemic vasculitis has been reported to impair endothelial function (as determined by brachial artery ultrasound) in vessels distant from the clinically inflamed sites, which improves after therapeutic suppression of the inflammatory process.36 This raises the possibility of a subclinical systemic vasculitis as a mechanism for increased arterial stiffness in rheumatoid patients. Finally, there is emerging morphological evidence of early atherosclerosis in rheumatoid subjects free of clinical cardiovascular disease and major risk factors. Two independent matched case-control studies found increased carotid intima-media thickness, an ultrasonographic parameter strongly associated with coronary atherosclerosis and cardiovascular risk,37 in rheumatoid subjects. Furthermore, carotid intima-media thickness correlated with disease duration.38,39
In this study we also found a significant correlation of AIx with RA disease duration (which was greater than with age), but not with disease activity parameters, such as CRP or DAS28. This suggests that the increased arterial stiffness in our patients reflected the cumulative inflammatory disease process rather than the degree of acute systemic inflammation. As our patients had, on average, late and deforming disease, it would seem likely that the increased AIx represents structural and probably early atherosclerotic rather than functional arterial change, despite their relatively young age. However, the number of patients in our study was relatively small and the median CRP level was relatively low (14 mg/l), both of which may explain the apparent lack of correlation between AIx and CRP. A further possible explanation may be that the effect of systemic inflammation on the functional (and potentially reversible) proportion reflected in the AIx—that is, endothelial dysfunction, may be masked or attenuated once structural atherosclerotic change is established. It should therefore prove interesting to determine arterial stiffness parameters, such as the AIx, in subjects with early RA, who are free of cardiovascular disease or risk factors. This would also seem timely as recent epidemiological evidence suggests that cardiovascular mortality may already be increased during the earlier years of inflammatory polyarthritis.40
Our study has some important limitations. We took great care to exclude subjects with known cardiovascular risk factors, including excessive steroid use6 and overt systemic rheumatoid vasculitis,5 which resulted in a relatively small sample size. Therefore the findings of this study will need confirmation in larger studies that should also seek to control for other aspects of the disease. For example, we cannot exclude the possibility that a reduced level of exercise, a frequent consequence of RA and recognised cardiovascular risk factor, might have contributed to our results. Additionally, the majority of our RA study group were receiving treatment with methotrexate, which may lead to hyperhomocysteinaemia, a further cardiovascular risk factor.41 However, folic acid supplementation, taken by eight of the 10 study subjects receiving methotrexate, may prevent hyperhomocysteinaemia during methotrexate treatment in RA,42 and a recent prospective study suggests that methotrexate treatment reduces overall and cardiovascular mortality in rheumatoid patients.43 Finally, a number of physiological variables are known to influence AIx: it is lower in men and inversely correlated with height and heart rate.21,44 It correlates positively with age and peripheral BP.11,21 In this study we achieved good matching between the RA and control groups for all these variables, except for systolic and mean peripheral BP, which were significantly higher in the control group. As a consequence, the AIx of our control group might have been higher than could be expected under better matching conditions; thus underestimating the true difference between the two groups.
In conclusion this matched cohort pilot study provides the first evidence that patients with RA have increased vascular stiffness and central BP. As our study subjects were free of cardiovascular disease and risk factors, we suggest that the inflammatory process associated with RA is responsible for our findings. A combination of structural and functional vascular changes, including endothelial dysfunction, may provide a possible mechanism for both atherosclerosis and LV dysfunction and hypertrophy. We suggest that the increased arterial stiffness and central BP contribute to the observed increased cardiovascular mortality and morbidity in subjects with RA. Larger studies are now warranted to confirm our findings and determine the relative contribution of rheumatoid disease and treatment variables to arterial stiffness.
Acknowledgments
This study was supported by the Research and Development Committee of the Royal National Hospital for Rheumatic Diseases, Bath. RK is currently an Arthritis Research Campaign (ARC), UK Clinical Research Fellow. JRC is supported by the British Heart Foundation. DRB is a recipient of an ARC programme grant, and the Royal National Hospital for Rheumatic Diseases is supported by an ARC Integrated Clinical Arthritis Centre Award.