Article Text

Abstract
Objective: To describe cases of lymphoma associated with anti-TNF therapy, identify risk factors, estimate the incidence and compare the risks for different anti-TNF agents.
Methods: A national prospective registry was designed (Research Axed on Tolerance of bIOtherapies; RATIO) to collect all cases of lymphoma in French patients receiving anti-TNF therapy from 2004 to 2006, whatever the indication. A case–control analysis was conducted including two controls treated with anti-TNF per case and an incidence study of lymphoma with the French population was used as the reference.
Results: 38 cases of lymphoma, 31 non-Hodgkin’s lymphoma (NHL) (26 B cell and five T cell), five Hodgkin’s lymphoma (HL) and two Hodgkin’s-like lymphoma were collected. Epstein–Barr virus was detected in both of two Hodgkin’s-like lymphoma, three of five HL and one NHL. Patients receiving adalimumab or infliximab had a higher risk than those treated with etanercept: standardised incidence ratio (SIR) 4.1 (2.3–7.1) and 3.6 (2.3–5.6) versus 0.9 (0.4–1.8). The exposure to adalimumab or infliximab versus etanercept was an independent risk factor for lymphoma in the case–control study: odds ratio 4.7 (1.3–17.7) and 4.1 (1.4–12.5), respectively. The sex and age-adjusted incidence rate of lymphoma was 42.1 per 100 000 patient-years. The SIR was 2.4 (95% CI 1.7 to 3.2).
Conclusion: The two to threefold increased risk of lymphoma in patients receiving anti-TNF therapy is similar to that expected for such patients with severe inflammatory diseases. Some lymphomas associated with immunosuppression may occur, and the risk of lymphoma is higher with monoclonal-antibody therapy than with soluble-receptor therapy.
Statistics from Altmetric.com
The risk of lymphoma is increased in several systemic autoimmune diseases, mainly Sjögren’s syndrome, systemic lupus erythematosus and rheumatoid arthritis (RA).1 In RA, the risk of non-Hodgkin’s lymphoma (NHL) is increased by twofold2 and that of Hodgkin’s lymphoma (HL) by threefold.3 Long-lasting inflammatory activity of RA is considered the main risk factor for lymphoma by its continuous stimulation of B cells.4
The effect of immunosuppressive drugs on the risk of lymphoma remains a matter of debate. To date, only the deleterious role of azathioprine has been demonstrated for both RA4 and Crohn’s disease (CD).5 Although withdrawal of methotrexate treatment can rarely induce a regression of Epstein–Barr virus (EBV)-associated lymphoproliferation,6 most recent reports did not find any increased risk of NHL in RA patients treated with methotrexate.7 8
Recent concerns about lymphoma have focused on therapy with anti-TNF drugs because of their profound immunoregulatory effect. However, anti-TNF therapy could reduce the inflammatory activity of the underlying disease, which is the main risk factor for lymphoma in RA.
In some cohorts of RA patients receiving anti-TNF therapy, the risk of lymphoma was no different to that for RA patients not receiving the therapy.7 9 10 11 However, these cohort studies were underpowered to investigate a difference between anti-TNF agents in terms of the risk of lymphoma.
We aimed to examine whether patients receiving anti-TNF agents have an increased risk of lymphoma and to compare the risks for different anti-TNF agents, describe the cases of lymphoma and their outcome, and identify the risk factors for lymphoma in patients receiving anti-TNF therapy.
Patients and methods
The French RATIO (Research Axed on Tolerance of bIOtherapies) registry was designed by a multidisciplinary group prospectively to collect all cases of lymphoma occurring in France, from 1 February 2004 to 31 January 2007, in patients who were receiving anti-TNF therapy, for whatever indication. The design has been described elsewhere.12 13 The reporting of this study conforms to the STROBE statement.14
Identification and validation of lymphoma cases
All cases reported to the 31 French pharmacovigilance regional centres of Agence Française de Sécurité Sanitaire des Produits de Santé (AFSSAPS), or pointed out directly to the companies producing anti-TNF commercially were collected. In addition, physicians from all the different French hospital centres involved either in the prescription of TNF blockers (ie, rheumatology, internal medicine, gastroenterology and dermatology departments) and/or in the management of lymphomas (ie, haematology or oncology centres), were directly required to report each newly diagnosed case). A direct mail reminder four times a year and several communications at congresses or in specialised press encouraged them to report cases.
Validation of cases
Included in the RATIO registry were all cases (from all sources) with a validated diagnosis of lymphoma according to the International Classification of Diseases for Oncology (categories 9590–9599, 9650–9660, 9670–9680, 9690–9699, 9700–9709 and 9710–9719). An expert committee involving three experts of lymphoma (XM, OH, MR) validated cases by consensus on the basis of the detailed standardised case report form and additional documents (hospitalisation summary, histological results or others). The biopsy specimens of all validated cases were reviewed by the same haematopathologist (MR), to validate the diagnosis obtained by histopathology. In addition, this haematopathologist assessed all biopsy specimens for the presence of EBV, detected by Eber in situ hybridisation.
Risk of lymphoma for patients receiving anti-TNF therapy
A case–control study was performed.
Cases
Cases were all validated cases of lymphoma in the RATIO registry with a labelling indication for the use of anti-TNF treatment (ie, RA, spondyloarthropathy (SpA; ankylosing spondylitis (AS) or psoriatic arthritis), ulcerative colitis or CD, or psoriasis).
Controls
Lymphoma-free patients receiving anti-TNF treatment in a labelling indication were included from centres participating in the RATIO registry (thus from the same population source) in a global pool of controls. From that pool, we randomly selected patients for a database of controls reflecting the proportion of patients receiving each of the three anti-TNF drugs in France. Two controls per case were randomly matched by sex, age (within 5 years) and underlying inflammatory disease from this database of controls. We also used a second sample of controls randomly selected from the same database of controls, with the same matching criteria (second matching).
Incidence study
Incidence of lymphoma
We estimated the annual incidence rate of lymphoma in patients treated with anti-TNF therapy, adjusted for age and sex, with the French population as a reference (see supplementary file for details, available online only).
Statistical analysis
The number of cases of lymphoma in France during the study period determined the sample size. A descriptive analysis was performed for the whole sample. We identified the risk factors of lymphoma by both univariate and multivariate analysis (conditional logistic regression model). The standardised incidence ratio (SIR) was calculated for anti-TNF agent use as a whole and for agents used individually. We performed subgroup and sensitivity analyses (see supplementary file for details, available online only).
Compliance with research ethics standards
This study was authorised by the ethics committee of AP-HP, GHU Nord (Institutional Review Board of Paris North Hospitals, Paris 7 University, AP-HP; authorisation number 162–08). The registry was reported at clinicaltrials.gov (ClinicalTrials.gov Identifier: NCT00224562).
Results
Description of the cases
We collected data on 41 cases of lymphomas and 38 cases were validated. Among them, 31 were NHL (26 B cell and five T cell), five HL and two Hodgkin’s-like lymphoma. The characteristics of the cases are shown in table 1.
Characteristics of the 38 lymphoma cases
Biopsy specimens were reviewed for 36 cases (29 NHL, 5 HL and two Hodgkin’s-like lymphomas). EBV was detected in both of two Hodgkin’s-like lymphoma, three of five HL and one B-cell lymphoproliferation.
The underlying disease was RA in 27 cases, SpA in seven cases (AS in four cases and psoriatic arthritis in three cases), CD in three cases and primary Sjögren’s syndrome in one case. Secondary Sjögren’s syndrome was present in three of 27 patients with RA and lymphoma. All patients were HIV negative. Most patients (31/38) had received only one anti-TNF agent. The three patients with CD and lymphoma had previously received azathioprine.
Outcome
Three patients with low-grade NHL received no lymphoma-specific treatment and anti-TNF therapy was stopped. They remained with stable disease, without any progression or regression of the lymphoma (follow-up 19.8–37.0 months). Among the other patients, 29 received chemotherapy, three rituximab alone and two radiotherapy, and one died before receiving chemotherapy. At last follow-up (median follow-up 18.2 months), 16 cases were in remission, in three disease was stable without specific treatment of the lymphoma, in three disease relapsed, seven were still being treated and nine patients died (24%); four of 27 with B-cell NHL, two of five with T-cell NHL and three of seven with HL and Hodgkin’s-like lymphoma.
Time occurrence of lymphoma with anti-TNF therapy
The median time from the onset of anti-TNF treatment and the first symptoms of lymphoma was 23.6 months. In five patients, lymphoma occurred, but anti-TNF therapy had been discontinued 6.1–44.1 months before. For these five patients, the last anti-TNF agent received was infliximab for three and adalimumab for two. As indicated in fig 1, the relation between the cumulative frequency of lymphoma and time from the onset of anti-TNF therapy appeared to be approximately linear for the first or last anti-TNF agent received and did not differ by drug received.
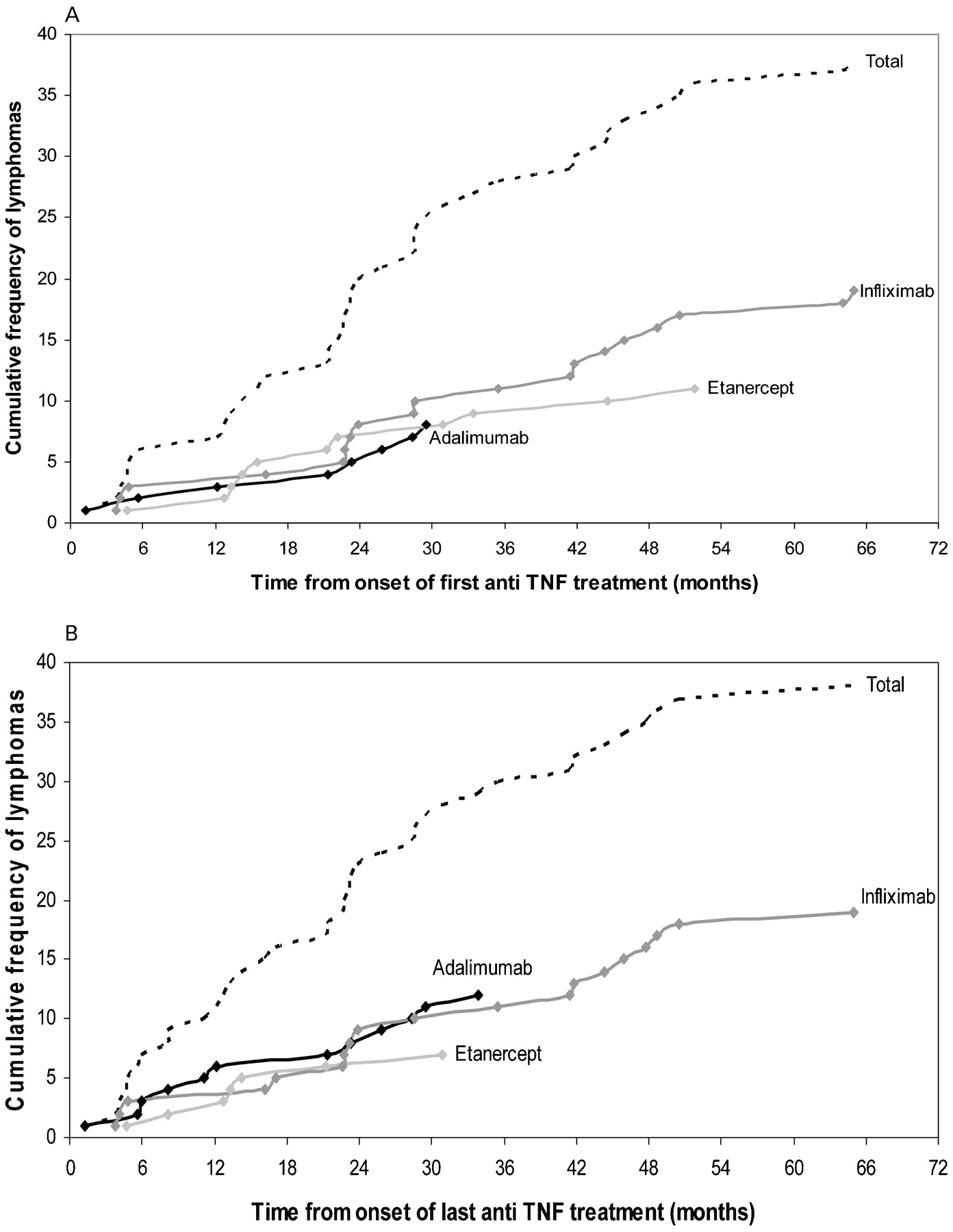
Time from onset of first and last anti-TNF treatment and first symptoms of lymphoma (months).
Risk factors of lymphoma for patients receiving anti-TNF therapy
The case–control study involved 37 cases and 74 controls (as described in the Methods section, the patient treated for Sjögren’s syndrome was not included). The repartition of the three anti-TNF agents in the control group corresponded to that found in the country during the 2004–6 period, with 18% receiving adalimumab, 51% etanercept and 31% infliximab. The results of univariate analysis are given in table 2.
Risk factors of lymphoma for patients receiving anti-TNF agents (univariate analysis: main analysis and analysis restricted to RA patients)
On the multivariate analysis (table 3), two factors were independently associated with the occurrence of lymphoma in patients receiving anti-TNF therapy: anti-TNF treatment duration less than 2 years (odds ratio (OR) 3.30; 95% CI 1.17 to 9.30) and treatment with infliximab or adalimumab versus etanercept (OR 4.12; 95% CI 1.36 to 12.49 and OR 4.73; 95% CI 1.27 to 17.65, respectively). In the case–control study restricted to RA cases, only one factor was associated with the occurrence of lymphoma: treatment with infliximab or adalimumab versus etanercept (OR 6.68; 95% CI 1.90 to 23.54). The OR of adalimumab or infliximab versus etanercept were also very similar with the second matching and in subgroup and sensitivity analyses (fig 2).

Estimation of the standardised incidence ratio (SIR) for the risk of lymphoma according to underlying disease and the histological subtype of lymphoma. ADA, adalimumab; HL, Hodgkin’s lymphoma; INF, infliximab; NHL, non-Hodgkin’s lymphoma; RA, rheumatoid arthritis; SpA, spondyloarthropathy.
Risk factors of lymphoma for patients receiving anti-TNF agents (multivariate analysis: main analysis and analysis restricted to RA patients)
Incidence and risk of lymphoma for patients receiving anti-TNF therapy compared with the general population
The main analysis relied on a total number of 57 711 patient-years of use of anti-TNF therapy during the 2004–6 period, as the denominator of the incidence rate. The annual incidence rate of lymphoma adjusted for age and sex among patients receiving anti-TNF therapy, with the French population as a reference, was 42.1 (95% CI 6.9 to 77.2 per 100 000 person-years). The SIR was 2.4 (95% CI 1.7 to 3.2; p<0.001) (fig 3). For RA and SpA, the SIR was 2.3 (95% CI 1.6 to 3.3; p<0.001) and 1.9 (95% CI 0.9 to 4.0; p = 0.09), respectively.

{kind=link}
{kind=link}
{kind=link}
Sensitivity analysis of the results of the case–control analysis: odds ratios (OR) for the risk of being treated with adalimumab or infliximab rather than with etanercept in multivariate analysis. RA, rheumatoid arthritis.
As with the case–control study, the incidence of lymphoma for patients receiving anti-TNF therapy differed depending on the agent received. The incidence rates for patients receiving etanercept, adalimumab and infliximab were 15.3 (95% CI 0.0 to 45.6) per 100 000 person-years, 65.1 (95% CI 0.0 to 160.0) per 100 000 person-years and 69.1 (95% CI 0.0 to 150.4) per 100 000 person-years, respectively. The SIR were 0.9 (95% CI 0.4 to 1.8; p = 0.72), 4.1 (95% CI 2.3 to 7.1; p<0.001) and 3.6 (95% CI 2.3 to 5.6; p<0.001), respectively. We found a difference between etanercept and monoclonal-antibody therapy in the main analysis and in the sensitivity analyses (fig 3), even when we separately used the different estimates from independent sources, which gave very consistent adjusted incidence rates and SIR (see supplementary fig 1, available online only).
Discussion
This 3-year study is the first national prospective study recording all cases of lymphoma in patients receiving anti-TNF agents, whatever the underlying disease. This study allowed us to collect enough cases to differentiate between lymphoma risk by the use of anti-TNF agent. We found a higher incidence of lymphoma with the use of the two monoclonal-antibody agents (adalimumab and infliximab) than with the soluble-receptor agent (etanercept).
Three cohorts of RA patients have been used to compare treatment with anti-TNF agents and with classic disease-modifying antirheumatic drugs in terms of the risk of lymphoma;7 9 10 11 and did not find an increased risk with anti-TNF agents (relative risk of 1.0 (0.6 to 1.8),7 1.35 (0.82 to 2.11)9 and 1.11 (0.51 to 2.37)10) These studies failed to demonstrate a difference between the treatments in the risk of lymphoma due to insufficient power. Although the design of the RATIO study has some limitations, it is probably the only way (or at least the most powerful way) to investigate the difference in risk with the use of anti-TNF agents.
Our study may have some limitations: the denominator of the incidence rate was estimated only. However, because each firm evaluated the number of patient-years in the period for each anti-TNF agent, the difference in risk between agents we observed cannot be explained by different methodologies used for the different agents. Furthermore, in the sensitivity analyses, the different estimates from independent sources gave very consistent adjusted incidence rates and SIR (see supplementary fig 1, available online only).
Despite the different strategies used to identify all the cases in the whole country, we cannot exclude that some cases were missed. We made the assumption that reporting was equal with each biological agent. Actually, the reporting of adverse events could be lower in patients treated subcutaneously (ie, etanercept and adalimumab) outside the hospital. However, in France, subcutaneously treated patients are mandatorily seen by hospital physicians initially and yearly for renewal. Moreover, the lack of adverse event reporting is a main issue for minor side effects but not for life-threatening side effects, particularly lymphomas that are a major concern for physicians and patients regarding anti-TNF agents. Furthermore, the patients treated with anti-TNF agents who have lymphomas could be notified to RATIO by the anti-TNF agent prescriptor (rheumatologist, gastroenterologist, internist or others), by the oncohaematologist, or by the pharmacovigilance regional centre. Finally, we found that the risk of lymphoma was similar for adalimumab and infliximab, which share the same mechanism of action (different from that of etanercept), but adalimumab is a subcutaneous anti-TNF agent and infliximab is an intravenous anti-TNF agent.
Finally, the cumulative activity of the disease, known as a risk factor of lymphoma at least for RA patients,4 could be different among patients receiving the different anti-TNF agents. Indeed, disease in patients receiving therapy at the beginning of anti-TNF availability (before 2002), was probably more severe, and such patients received infliximab (the only anti-TNF agent available in France at that time) exclusively. However, patients with anti-TNF onset before 2002 did not have a higher risk of lymphoma than others (anti-TNF onset before 2002 versus others: OR 1.3 (95% CI 0.5 to 3.7); p = 0.60). Furthermore, the comparison between the type of drug used and risk was adjusted on the time from the onset of anti-TNF treatment (table 3). In addition, indirect markers of disease activity (median duration of the inflammatory underlying disease, percentage of patients treated with steroids, frequency of positive rheumatoid factor and anti-cyclic citrullinated peptide in RA patients) were not greater in patients treated with infliximab or adalimumab than in those treated with etanercept (data not shown). Finally, the impact of a putative difference in the duration of exposure and in disease activity depending on the year of introduction of the anti-TNF agent probably cannot explain the difference in incidence of lymphoma depending on the type of anti-TNF agent used, because we observed exactly the same increased risk of lymphoma for patients receiving infliximab, which was introduced in 1999, and adalimumab, which has been available since 2004, whereas the risk was lower with the use of etanercept, available in France from early 2003.
The strengths of this study are that our population of focus was the whole French population receiving anti-TNF therapy, whatever the indication for use, rather than a limited and selected population included in a specific cohort study. Furthermore, all cases were validated by an expert committee, and the biopsy specimens were centralised, reviewed by the same haematopathologist and tested for EBV.
Even though the overall risk of lymphoma in RA patients treated with anti-TNF therapy does not appear to differ greatly from what is expected in a population of patients with inflammatory diseases,1 2 3 the risk differs depending on the anti-TNF drug used (higher risk with monoclonal anti-TNF therapy, adalimumab and infliximab). This difference in risk depending on agent was found in the case–control study and was confirmed in the comparison of incidence with the general population, which supports the robustness of this finding. A meta-analysis assessing cancers in randomised controlled trials using monoclonal anti-TNF therapy, adalimumab and infliximab, in RA patients revealed 10 cases of lymphoma (four in randomised phases of trials and six in extension phases) in treated groups (3493 patient-years) and none in placebo groups (1512 patient-years).15 The same analysis of randomised controlled trials with etanercept of 2484 patient-years with etanercept treatment and 1072 patient-years with control therapy revealed two cases of lymphoma with etanercept therapy and none with control therapy.16 Finally, cases of hepatosplenic T-cell lymphoma have been described in adolescents and young adults with CD treated with monoclonal antibodies and azathioprine combined (10 cases with infliximab17 and three cases with adalimumab.18)
The absence of an intrinsic increased risk of lymphoma in SpA patients makes this population an ideal model for assessing the anti-TNF-related risk of lymphoma.19 In our study, no significant increase in the risk of lymphoma was observed in patients receiving anti-TNF therapy for SpA. However, no definitive conclusion can be drawn from our data based on a very few cases of lymphoma in SpA patients. Some of the cases we observed reinforce the likelihood of a causal role of anti-TNF therapy in the risk of lymphoma. In one patient with AS who never received other immunosuppressors, including methotrexate, EBV-associated Hodgkin’s-like lymphoma developed after treatment with infliximab. We observed three cases of EBV-induced lymphoproliferation: two cases of EBV-associated Hodgkin’s-like lymphomas with infliximab treatment (one with RA, one with AS described above) and one case of EBV-associated B-cell NHL in a patient with RA treated with adalimumab. These three cases demonstrate that lymphomas similar to post-transplant lymphoproliferative disease may occur, even rarely, with anti-TNF treatment. In the literature, one case of EBV-associated lymphoproliferation in a patient with RA treated with etanercept regressed after withdrawal of the drug.20 Another case of hypopharynx mucosa-associated lymphoid tissue lymphoma not associated with EBV regressed spontaneously after the withdrawal of infliximab.21
The pathophysiological mechanism inducing a higher risk of lymphoma in patients receiving anti-TNF therapy remains unclear. A direct action of TNF or anti-TNF on B cells was hypothesised, but no increase in survival or apoptosis with TNF or infliximab treatment was found.22
Actually, in inflammatory diseases and especially RA, the three anti-TNF agents may have opposite effects: a beneficial effect due to the decrease in activity of the disease and a deleterious effect due to immunomodulatory activity, which may concern EBV-associated lymphoma but also more classic lymphoma. The mechanism of action of this deleterious effect is still unknown but could be related to T-cell control of viruses such as EBV or of other mechanisms of lymphomagenesis. This T-cell control may require integrity of membrane TNF, which is upregulated in activated T cells. Some studies suggest a higher efficacy of anti-TNF monoclonal-antibody treatment than TNF-soluble receptor therapy for inhibiting membrane TNF signalling,23 which could lead to a decreased immune surveillance of different mechanisms of lymphomagenesis.
In conclusion, the two to threefold overall increased risk of lymphoma in patients receiving anti-TNF therapy does not appear to differ greatly from what is expected in a population of such patients with severe inflammatory diseases. However, some lymphomas associated with immunosuppression may occur in such patients. The incidence of lymphoma is higher with monoclonal-antibody agents than with the soluble receptor. This may be due to a difference of targeting membrane TNF, leading also to a difference of effectiveness in some diseases such as CD or granulomatous diseases.
Acknowledgments
The authors thank all the clinicians who actively participated in the RATIO registry: Abitbol (Paris), Allanore (Paris), André (Clermont-Ferrand), Ardizzone (Mulhouse), Bergman (Paris), Azais (Poitiers), Bachelez (Paris), Bardet (Orléans), Beau (Poitiers), Bergman (Paris), Belmatoug (Clichy), Berthelot (Nantes), Blasco (Barbois), Bonnet (Limoges), Bouhnik (Clichy), Bourgarit (Paris), Bouvard (Angers), Bressot (Chalon sur Saone), Briançon (Aix les Bains), Brocq (Nice), Cadiot (Reims), Castela (Nice), Visanica (Metz), Combert (La Rochelle), Couret (Valence), Cuillerier (Dreux), Dalle (Lyon), Dasilva (Elbeuf), Debandt (Aulnay sous Bois), Debourdeau (Lyon), Depernet (Langers), Dereure (Montpellier), Descamps (Paris), Duriez (Saint-Brieuc), Fach (Bergerac), Fain (Bondy), Fautrel (Paris), Filippi (Nice), Fior (Bondy), Flourie (Lyon), Fulpin (Marseille), Gaborit (Orange), Gaudin (Grenoble), Gendre (Paris), Ghringhelli (Bordeaux), Gillet (Nancy), Goupille (Tours), Grados (Amiens), Grosclaude (Uriage), Gueit (Rouen), Guillaume (Colmar), Guyot (Roubaix), Heresbach (Rennes), Hoen (Besançon), Houvennagel (Lomme), Beguinot (Reims), Jang-Guyro (Briançon), Jardin (Privas), Justum (Caen), Laharie (Bordeaux), Lambotte (Le Kremlin-Bicêtre), Lecompte (Nancy), Leparc (Boulogne-Billancourt), Lequen (Pau), L’Hirondel (Caen), Liné (Soissons), Lioté (Paris), Lucht (Saint Etienne), Maillefert (Dijon), Marguerie (Berck), Maqub (Arles), Marteau (Paris), Martin (Saint-Brieuc), Mehadaoui (Evreux), Melac-Ducamp (Nevers), Meyer (Paris), Miceli (Le Kremlin-Bicêtre), Michelet (Rennes), Morel (Montpellier), Nocent (Bayonne), Novel (Dijon), Pallot Prades (Saint-Etienne), Pham (Marseille), Piroth (Dijon), Perdriger (Rennes), Pertuiset (Pontoise), Petitou (Bigorre), Pouplin (Rouen), Puechal (Le Mans), Pujol (Clermont Ferrand), Rouidi (Dreux), Sacchi (Mantes-La Jolie), Saindenberg (Clichy), Salmon (Paris), Schaeverbeke (Bordeaux), Solau-Gervais (Lille), Sordet (Strasbourg), Sprunk (Bourg en Bresse), Taillan (Monaco), Thevenot (Laon), Thorel (Lorient), Ulmann (Marseille), Vernhes (Libourne), Wendling (Besançon), Zarnitsky (Le Havre), Zabraniecki (Toulouse), Zeller (Paris). The authors are also grateful to GR Auleley, J Deligne and C Blum-Boisgard from the RSI for providing data to validate the denominator estimate of the incidence rate we used, P Grosclaude from the Francim for providing the French annual incidence rate of lymphoma by 5-year age and sex class in 2005, the AFSSAPS and the regional pharmacovigilance centres for their contribution to the exhaustiveness of the RATIO registry. The authors also thank C Roy and G Baron for the statistical analysis, and N Nicolas, S Makhlouf and A Djemoui for their help in collecting and preparing the validation of the cases.
REFERENCES
Supplementary materials
Web Only Data 69/2/400
Files in this Data Supplement:
Footnotes
▸ Additional supplementary files and supplementary fig 1 are published online only at http://ard.bmj.com/content/vol69/issue2
For numbered affiliations see end of article
Funding The RATIO was supported by a research grant from Institut National pour la Santé et la Recherche Médicale (INSERM) (Réseau de recherche clinique 2003 and 2006) and by an unrestricted grant from Abbott, Schering Plough and Wyeth. The pharmaceutical companies (Abbott, Schering Plough and Wyeth) had no role in the design and conduct of the study, collection, management, analysis and interpretation of the data, preparation, review, or approval of the manuscript.
Competing interests Declared. XM received consulting and/or talk honorarium from Abbott, Schering Plough, UCB and Wyeth. TS received consulting and/or talk honorarium from Abbott, Schering Plough and Wyeth. ML received consulting and/or talk honorarium from Abbott, Schering Plough and UCB.
Ethics approval This study was authorised by the ethics committee of AP-HP, GHU Nord (Institutional Review Board of Paris North Hospitals, Paris 7 University, AP-HP; authorisation number 162–08).
The first two authors contributed equally to the work.
Contributors: Conception and design: XM, FT, DS, ML, PR. Acquisition of data: XM, HB, MB, JMB, PG, DH, AM, TS, DS, ML, OH, MR. Analysis and interpretation of data: XM, FT, PR. Drafting the article and revising it critically for important intellectual content: XM, FT, PR. Final approval of the version to be published: XM, FT, HB, MB, JMB, PG, DH, AM, TS, DS, ML, OH, MR, PR. XM, FT and PR had full access to the data in the and take responsibility for the integrity of the data and the accuracy of the data analysis. The main analyses were independently performed by two academic statisticians.
Provenance and Peer review Not commissioned; externally peer reviewed.