Australians are not Meeting the Recommended Intakes for Omega-3 Long Chain Polyunsaturated Fatty Acids: Results of an Analysis from the 2011–2012 National Nutrition and Physical Activity Survey


Abstract
:1. Introduction
2. Results
2.1. Numbers of Subjects from the 2011–2012 NNPAS and the NNS 1995 Surveys
2.2. The 2011–2012 NNPAS PUFA, LA, LNA, and n-3 LCPUFA Intakes per Day
2.3. Comparison of the Median and Mean n-3 LCPUFA Intakes from the 2011–2012 NNPAS (Figure 1)
2.4. Comparison of n-3 LCPUFA Intakes to Recommended Intakes
2.4.1. The Proportion of Adult Female and Male (19+ Years) Meeting the Recommended Intakes (Table 3)
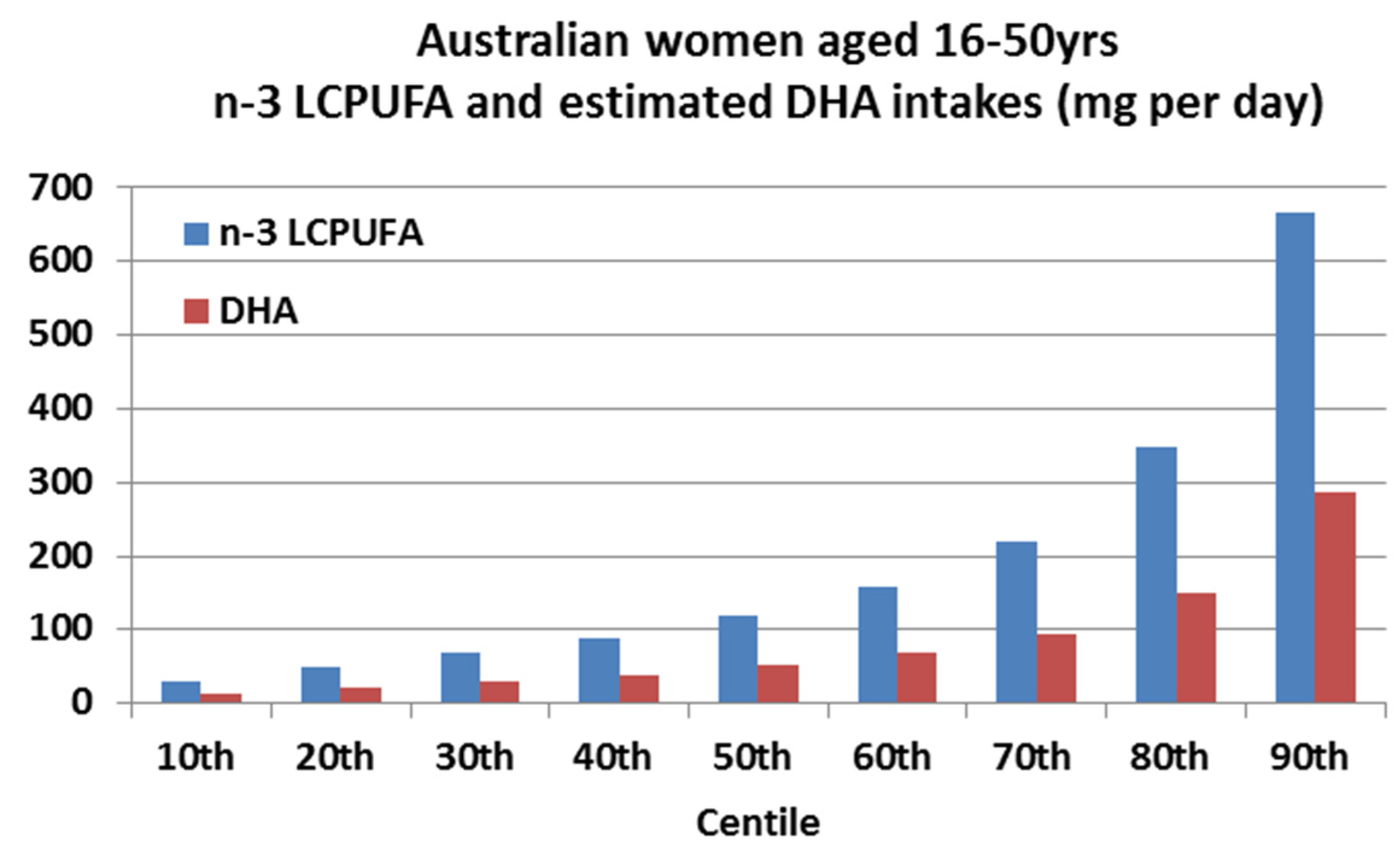
2.4.2. Adult Females of Childbearing Age (16–50 Years) n-3 LCPUFA and DHA Intakes across Centiles and Comparison to the ISSFAL Recommendations for DHA Intake (Figure 2)
2.5. Comparison of Adult Australian Intakes of food and the Respective n-3 LCPUFA in Those Foods
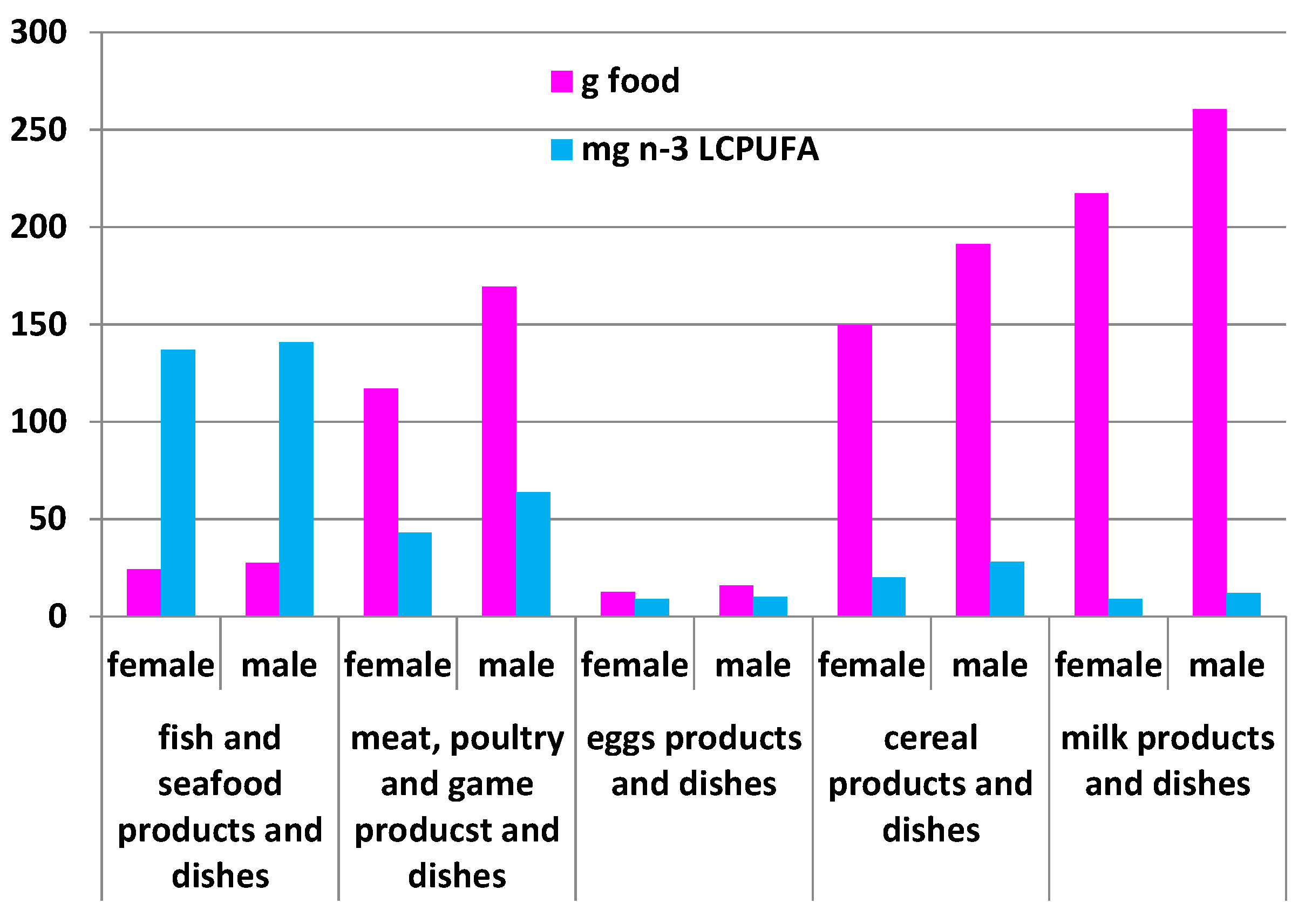
2.5.1. Comparison of the Amount of Food Eaten (g per Day) by Adult Australians and the Respective Amount of n-3 LCPUFA Intakes (mg per Day) from the 2011–2012 NNPAS (Figure 3)
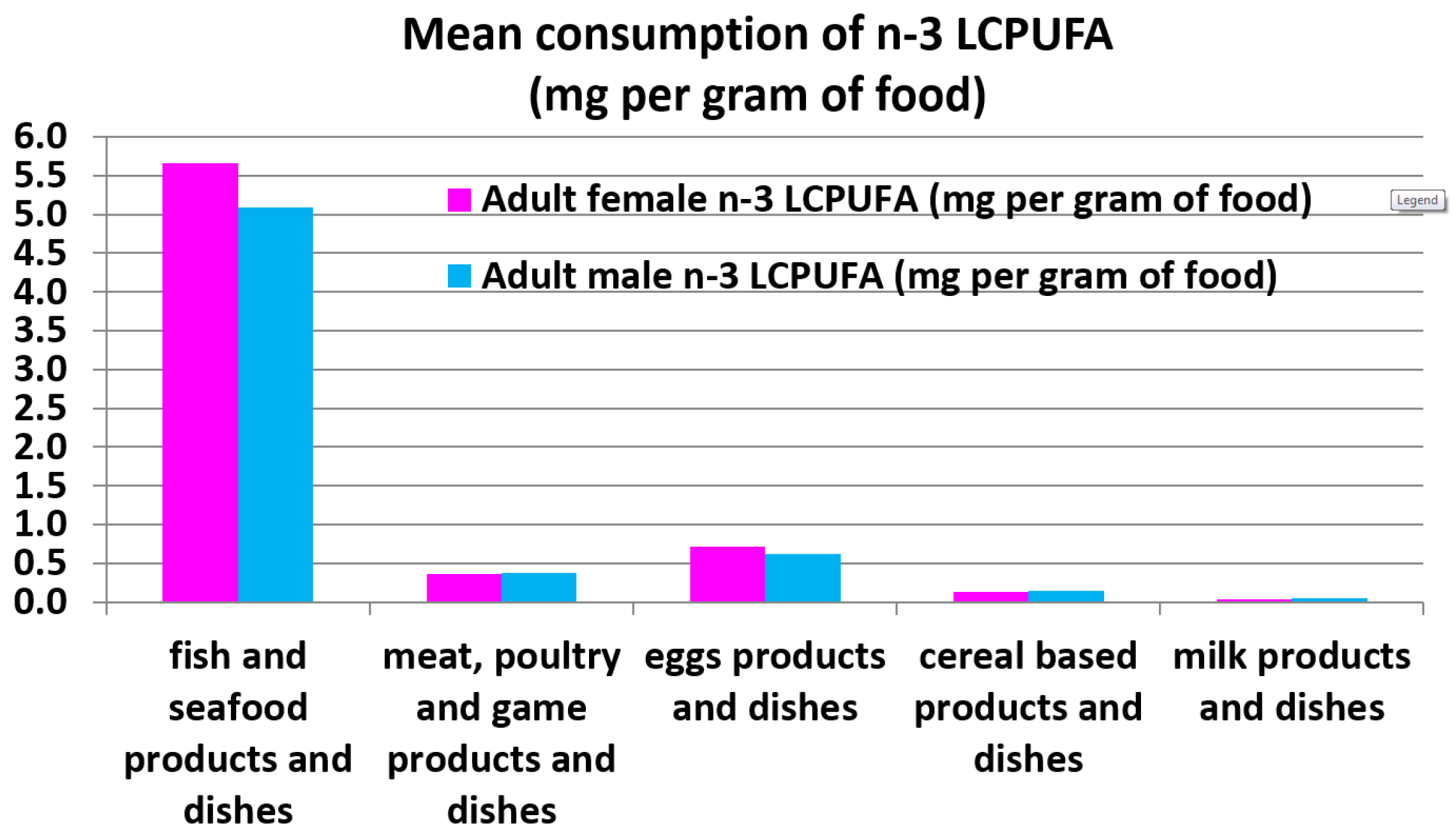
2.5.2. Comparison of the Adult Female and Male Mean Consumption n-3 LCPUFA Intakes (mg per g of Food) for the Various Food Groups (Figure 4)
2.6. Comparison of the 2011–2012 NNPAS and NNS 1995
2.6.1. Comparison of the PUFA Intakes from the Two Australian National Nutrition Surveys: NNS 1995 and 2011–2012 NNPAS (Figure 5)
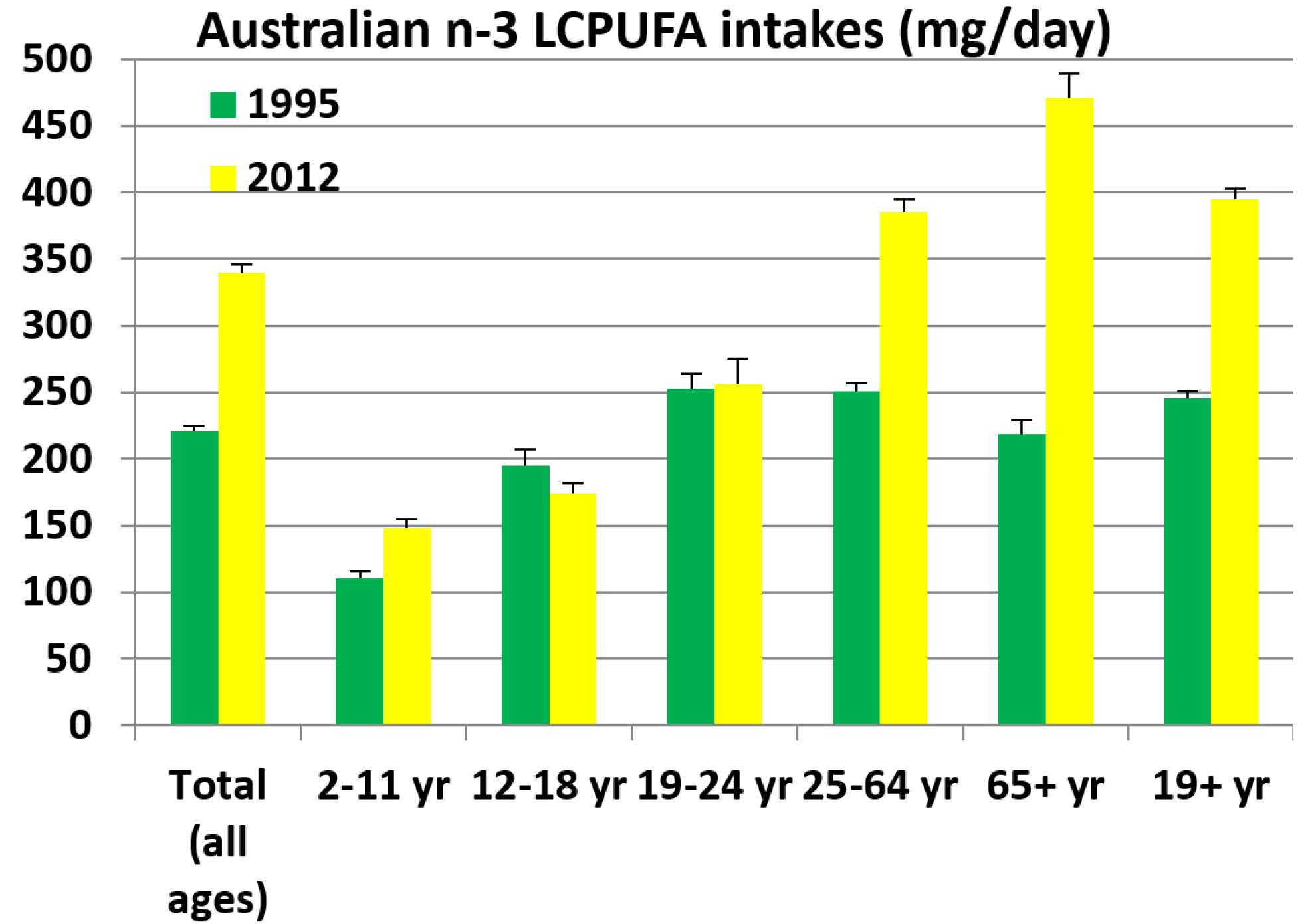
2.6.2. Comparison of the n-3 LCPUFA Intakes from the Two Australian National Nutrition Surveys: NNS 1995 and 2011–2012 NNPAS (Figure 6)
3. Discussion
4. Materials and Methods
4.1. The Australian Health Survey 2011-13 (AHS) Containing the 2011–2012 National Nutrition and Physical Activity Survey (2011–2012 NNPAS) Data from the Australian Bureau of Statistics (ABS)
4.2. NNS 1995 Survey Data
4.3. Confidential Unit Record Files (CURF)
4.4. Analysis of 2011–2012 NNPAS 24-h Recall Data
4.5. Comparison of n-3 LCPUFA to Recommended Intakes
4.6. Comparison of Adult Australian Mean Food Intake and the Respective n-3 LCPUFA Intakes
4.7. Comparisons of NNS 1995 and 2011–2012 NNPAS
5. Conclusions
Acknowledgments
Conflicts of Interest
Abbreviations
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three letter acronym |
| LD | linear dichroism |
References
- Meyer, B.J.; Mann, N.J.; Lewis, J.L.; Milligan, G.C.; Sinclair, A.J.; Howe, P.R.C. Dietary intakes and food sources of omega-6 and omega-3 polyunsaturated fatty acids. Lipids 2003, 38, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Connor, W.E. Importance of n-3 fatty acids in health and disease. Am. J. Clin. Nutr. 2000, 71, 171–175. [Google Scholar]
- Siscovick, D.S.; Raghunathan, T.E.; King, I.; Weinmann, S.; Wicklund, K.G.; Albright, J.; Bovbjerg, V.; Arbogast, P.; Smith, H.H.; Kushi, L.H.; et al. Dietary-intake and cell-membrane levels of long-chain n-3 polyunsaturated fatty-acids and the risk of primary cardiac-arrest. J. Am. Med. Assoc. 1995, 274, 1363–1367. [Google Scholar] [CrossRef]
- De Lorgeril, M.; Salen, P.; Martin, J.L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean diet, traditional risk factors and the rate of cardiovascular complications after myocardial infarction—Final report of the Lyon diet heart study. Circulation 1999, 99, 779–785. [Google Scholar] [CrossRef] [PubMed]
- GISSI-Prevenzione Investigators. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: Results of the GISSI-Pevenzione trial. Lancet 1999, 354, 447–455. [Google Scholar]
- Simopoulos, A.P. Essential fatty acids in health and chronic disease. Am. J. Clin. Nutr. 1999, 70, 560–569. [Google Scholar]
- Von Schacky, C.; Angerer, P.; Kothny, W.; Theisen, K.; Mudra, H. The effect of dietary omega-3 fatty acids on coronary atherosclerosis—A randomised, double-blind, placebo-controlled trial. Ann. Int. Med. 1999, 130, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Sinn, N.; Milte, C.; Howe, P.R.C. Oiling the brain: A review of randomised controlled trials of omega-3 fatty acids in psychopathology across the lifespan. Nutrients 2010, 2, 128–170. [Google Scholar] [CrossRef] [PubMed]
- Parletta, N.; Milte, C.M.; Meyer, B.J. Nutritional modulation of cognitive function and mental health. J. Nutr. Biochem. 2013, 24, 725–743. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand including Recommended Dietary Intakes; Australian Government Department of Health and Ageing: Canberra, Australia, 2006. [Google Scholar]
- Howe, P.; Meyer, B.J.; Record, S.; Baghurst, K. Dietary intake of long-chain n-3 polyunsaturated fatty acids: Contribution of meat sources. Nutrition 2006, 22, 47–53. [Google Scholar] [CrossRef] [PubMed]
- International Society for the Study of Fatty Acids and Lipids (ISSFAL). PUFA Recommendations. Available online: http://www.issfal.org/statements/pufa-recommendations (accessed on 15 December 2015).
- Koletzko, B.; Cetin, I.; Brenna, J.T.; the Perinatal Lipid Intake Working Group. Consensus Statement: Dietary fat intakes for pregnant and lactating women. Br. J. Nutr. 2007, 98, 873–877. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 4363.0.55.001-Australian Health Survey: Users’ Guide, 2011–2013. Comparisons with 1995 NNS. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/FB554091B09E8C05CA257CD2001E3214?opendocument (accessed on 3 February 2016).
- Papanikolau, Y.; Brooks, J.; Reider, C.; Fulgoni, V.L. U.S. adults are not meeting recommended levels for fish and omega-3 fatty acid intake: Results of an analysis using observational data from NHANES 2003–2008. Nutr. J. 2014, 13, p. 31. Available online: http://www.nutritionj.com/content/13/1/31 (accessed on 15 December 2015). [CrossRef] [PubMed]
- Nakamura, Y.; Ueshima, H.; Okuda, N.; Miura, K.; Kita, Y.; Okamura, T.; Turin, T.C.; Okayama, A.; Rodriguez, B.; Curb, J.D.; et al. Relation of dietary and other lifestyle traits to difference in serum adiponectin concentrations of Japanese in Japan and Hawaii: The INTERLIPID Study. Am. J. Clin. Nutr. 2008, 88, 424–430. [Google Scholar] [PubMed]
- Hino, A.; Adachi, H.; Toyomasu, K.; Yoshida, N.; Enomoto, M.; Hiratsuka, A.; Hirai, Y.; Satoh, A.; Imaizumi, T. Very long chain n-3 fatty acids intake and carotid atherosclerosis. An epidemiological study evaluated by ultrasonography. Atherosclerosis 2004, 176, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Fayet-Moore, F.; Baghurst, K.; Meyer, B.J. Four models including fish, seafood, red meat and enriched foods to achieve Australian dietary recommendations for the n-3 LCPUFA for all life-stages. Nutrients 2015, 7, 8112–8126. [Google Scholar] [CrossRef] [PubMed]
- Bucher, H.C.; Hengstler, P.; Schindler, C.; Meier, G. n-3 polyunsaturated fatty acids in coronary heart disease: A meta-analysis of randomized controlled trials. Am. J. Med. 2002, 112, 298–304. [Google Scholar] [CrossRef]
- Wen, Y.T.; Dai, J.H.; Gao, Q. Effects of omega-3 fatty acid on major cardiovascular events and mortality with coronary heart disease: A meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Nestel, P.; Clifton, P.; Colquhoun, D.; Noakes, M.; Mori, T.A.; Thomas, B. Indications for omega-3 long chain polyunsaturated fatty acid in the prevention and treatment of cardiovascular disease. Heart Lung Circ. 2015, 24, 769–779. [Google Scholar] [CrossRef] [PubMed]
- James, M.; Sullivan, T.R.; Metcalf, R.G.; Cleland, L.G. Pitfalls in the use of randomized controlled trials for fish oil studies with cardiac patients. Br. J. Nutr. 2014, 112, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Krauss, R.M.; Eckel, R.H.; Howard, B.; Appel, L.J.; Daniels, S.R.; Deckelbaum, R.J.; Erdman, J.W., Jr.; Kris-Etherton, P.; Goldberg, I.J.; Kotchen, K.A.; et al. AHA dietary guidelines: Revision 2000: A statement for healthcare professionals from the Nutrition Committee of the American Heart Association. Circulation 2000, 102, 2284–2299. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Harris, W.S.; Appel, L.J. Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Circulation 2002, 106, 2747–2757. [Google Scholar] [CrossRef] [PubMed]
- Bimbo, A.P. The Evolution of Fish Oils to Omega 3 Fatty Acids and a Global Consumer Market of US$25 Billion; West Virginia University Research Corporation Forum Linking Innovation, Industry, and Commercialization Dean’s Open Forum on Innovation and Entrepreneurship Davis College of Agriculture, Natural Resources & Design: Morgantown, WV, USA, 25 April 2013. [Google Scholar]
- Farquharson, A.L.; Metcalf, R.G.; Sanders, P.; Stuklis, R.; Edwards, J.R.M.; Gibson, R.A.; Cleland, L.G.; Sullivan, T.R.; James, M.J.; Young, G.D. Effect of dietary fish oil on atrial fibrillation after cardiac surgery. Am. J. Cardiol. 2011, 108, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Makrides, M.; Gibson, R.A. Long-chain polyunsaturated fatty acid requirements during pregnancy and lactation. Am. J. Clin. Nutr. 2000, 71, 307S–311S. [Google Scholar] [PubMed]
- Sattar, N.; Berry, C.; Greer, I.A. Essential fatty acids in relation to pregnancy complications and fetal development. Br. J. Obstet. Gynaecol. 1998, 105, 1248–1255. [Google Scholar] [CrossRef] [PubMed]
- Innis, S.M.; Friesen, R.W. Essential n-3 fatty acids in pregnant women and early visual acuity maturation in term infants. Am. J. Clin. Nutr. 2008, 87, 548–557. [Google Scholar] [PubMed]
- Meyer, B.J.; Onyiaodike, C.C.; Brown, E.A.; Jordan, F.; Murray, H.; Nibbs, R.J.B.; Sattar, N.; Lyall, H.; Nelson, S.M.; Freeman, D.J. Maternal plasma DHA levels increase prior to 29 days post-LH surge in women undergoing frozen embryo transfer: A prospective, observational study of human pregnancy. J. Clin. Endo. Metab. 2016, in press. [Google Scholar] [CrossRef] [PubMed]
- Cosatto, V.F.; Else, P.L.; Meyer, B.J. Do pregnant women and those at risk of developing post-natal depression consume lower amounts of long chain omega-3 polyunsaturated fatty acids? Nutrients 2010, 2, 198–213. [Google Scholar] [CrossRef] [PubMed]
- Ollis, T.E.; Meyer, B.J.; Howe, P.R.C. Australian food sources and intakes of omega-6 and omega-3 polyunsaturated fatty acids. Ann. Nutr. Metab. 1999, 43, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Health Survey. Available online: http://www.abs.gov.au/australianhealthsurvey (accessed on 15 December 2015).
- Bliss, R.M. Researchers produce innovation in dietary recall. Agric. Res. 2004, 52, 10–12. [Google Scholar]
- Australian Bureau of Statistics. 4363.0.55.001-Australian Health Survey: Users’ guide, 2011–2013. 24-h Dietary Recall. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/0D6B1FE95EAB8FF3CA257CD2001CA113?opendocument (accessed on 15 December 2015).
- McLennan, W.; Podger, A. National Nutrition Survey, Selected Highlights, Australia; Government Publishing Service: Canberra, Australian, 1997. [Google Scholar]
- Australian Bureau of Statistics. 4324.0.55.002–Microdata: Australian Health Survey: Nutrition and Physical Activity, 2011–2012. Introduction. Available online: http://abs.gov.au/AUSSTATS/[email protected]/Lookup/4324.0.55.002Main+Features12011-12 (accessed on 15 December 2015).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Category | 2011–2012 NNPAS sample | NNS 1995 Sample | ||||
|---|---|---|---|---|---|---|
| Female | Male | Total | Female | Male | Total | |
| All ages | 6451 | 5702 | 12,153 | 7242 | 6616 | 13,858 |
| 2–11 years | 857 | 854 | 1711 | 950 | 971 | 1921 |
| 12–18 years | 535 | 566 | 1101 | 522 | 564 | 1086 |
| 19–24 years | 360 | 326 | 686 | 575 | 485 | 1060 |
| 25–64 years | 3506 | 3046 | 6552 | 4137 | 3694 | 7831 |
| ≥65 years | 1193 | 910 | 2103 | 1058 | 902 | 1960 |
| ≥19 years | 5059 | 4282 | 9341 | 5770 | 5081 | 10,851 |
| Age Category and Gender | PUFA (g) | LA (g) | LNA (g) | n-3 LCPUFA (mg) |
|---|---|---|---|---|
| Total F | 9.5 ± 0.1 | 7.8 ± 0.06 | 1.2 ± 0.01 | 335 ± 9 |
| Total M | 11.4 ± 0.1 | 9.4 ± 0.08 | 1.4 ± 0.01 | 346 ± 9 |
| 2–11 F | 7.1 ± 0.1 | 5.9 ± 0.12 | 0.9 ± 0.02 | 138 ± 10 |
| 2–11 M | 8.2 ± 0.2 | 6.8 ± 0.13 | 1.0 ± 0.02 | 158 ± 11 |
| 12–18 F | 9.6 ± 0.2 | 8.1 ± 0.22 | 1.2 ± 0.03 | 133 ± 7 |
| 12–18 M | 11.5 ± 0.3 | 9.6 ± 0.22 | 1.4 ± 0.03 | 213 ± 15 |
| 19–24 F | 10.1 ± 0.3 | 8.5 ± 0.28 | 1.2 ± 0.04 | 175 ± 14 |
| 19–24 M | 13.4 ± 0.5 | 11.2 ± 0.42 | 1.6 ± 0.06 | 346 ± 36 |
| 25–64 F | 10.2 ± 0.1 | 8.3 ± 0.09 | 1.3 ± 0.02 | 378 ± 14 |
| 25–64 M | 12.4 ± 0.1 | 10.2 ± 0.12 | 1.5 ± 0.02 | 395 ± 14 |
| ≥65 F | 9.1 ± 0.2 | 7.2 ± 0.13 | 1.2 ± 0.03 | 494 ± 26 |
| ≥65 M | 10.5 ± 0.2 | 8.4 ± 0.17 | 1.4 ± 0.03 | 441 ± 24 |
| ≥19 F | 9.9 ± 0.1 | 8.0 ± 0.07 | 1.2 ± 0.01 | 390 ± 11 |
| ≥19 M | 12.1 ± 0.1 | 9.9 ± 0.10 | 1.5 ± 0.02 | 401 ± 12 |
| Recommended Intakes for Females 19+ Years | Females 19+ Years (n = 5059) | No Supplements (n = 4054, 75%) | With Supplements (n = 1005, 25%) |
|---|---|---|---|
| >430 mg per day * | n = 1126 (22%) | n = 446 (11%) | n = 673 (67%) |
| >500 mg per day # | n = 1001 (20%) | n = 386 (9.5%) | n = 613 (61%) |
| Recommended Intakes for Males 19+ Years | Males 19+ Years (n = 4282) | No supplements (n = 3625, 85%) | With supplements (n = 657, 15%) |
| >500 mg per day # | n = 844 (20%) | n = 399 (11%) | n = 368 (56%) |
| >610 mg per day * | n = 702 (16%) | n = 326 (9%) | n = 302 (46%) |
© 2016 by the author; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, B.J. Australians are not Meeting the Recommended Intakes for Omega-3 Long Chain Polyunsaturated Fatty Acids: Results of an Analysis from the 2011–2012 National Nutrition and Physical Activity Survey. Nutrients 2016, 8, 111. https://doi.org/10.3390/nu8030111
Meyer BJ. Australians are not Meeting the Recommended Intakes for Omega-3 Long Chain Polyunsaturated Fatty Acids: Results of an Analysis from the 2011–2012 National Nutrition and Physical Activity Survey. Nutrients. 2016; 8(3):111. https://doi.org/10.3390/nu8030111
Chicago/Turabian StyleMeyer, Barbara J. 2016. "Australians are not Meeting the Recommended Intakes for Omega-3 Long Chain Polyunsaturated Fatty Acids: Results of an Analysis from the 2011–2012 National Nutrition and Physical Activity Survey" Nutrients 8, no. 3: 111. https://doi.org/10.3390/nu8030111