
Abstract
Background
HIV testing is cost-effective in unselected general medical populations, yet testing rates among those at risk remain low, even among those with regular primary care. HIV rapid testing is effective in many healthcare settings, but scant research has been done within primary care settings or within the US Department of Veteran’s Affairs Healthcare System.
Objectives
We evaluated three methods proven effective in other diseases/settings: nurse standing orders for testing, streamlined counseling, and HIV rapid testing.
Design
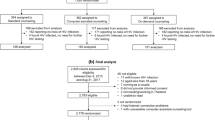
Randomized, controlled trial with three intervention models: model A (traditional counseling/testing); model B (nurse-initiated screening, traditional counseling/testing); model C (nurse-initiated screening, streamlined counseling/rapid testing).
Participants
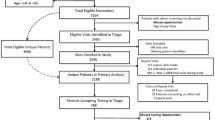
Two hundred fifty-one patients with primary/urgent care appointments in two VA clinics in the same city (one large urban hospital, one freestanding outpatient clinic in a high HIV prevalence area).
Measurements
Rates of HIV testing and receipt of results; sexual risk reduction; HIV knowledge improvement.
Results
Testing rates were 40.2% (model A), 84.5% (model B), and 89.3% (model C; p = <.01). Test result receipt rates were 14.6% (model A), 31.0% (model B), 79.8% (model C; all p = <.01). Sexual risk reduction and knowledge improvement did not differ significantly between counseling methods.
Conclusions
Streamlined counseling with rapid testing significantly increased testing and receipt rates over current practice without changes in risk behavior or posttest knowledge. Increased testing and receipt of results could lead to earlier disease identification, increased treatment, and reduced morbidity/mortality. Policymakers should consider streamlined counseling/rapid testing when implementing routine HIV testing into primary/urgent care.

Similar content being viewed by others

References
Palella FJ Jr, Deloria-Knoll M, Chmiel JS, et al. Survival benefit of initiating antiretroviral therapy in HIV-infected persons in different CD4+ cell strata. Ann Intern Med. 2003;138(8):680–681.
Anastos K, et al. Women’s interagency HIV study collaborative study group: risk of progression to AIDS and death in women infected with HIV-1 initiating highly active antiretroviral treatment at different stages of disease. Arch Intern Med. 2002;162(17):1973–1980.
Centers for Disease Control (US). HIV and AIDS—United States, 1981–2001. MMWR. 2001;50:430–434.
Gandhi NR, et al. Delayed presentation for HIV care among veterans: an opportunity for intervention. (Annual meeting, 13th Conference on Retrovirus and Opportunistic Infections, Denver, 2006).
Sanders GD, Bayoumi AM, Sundaram V, et al. Cost-effectiveness of screening for HIV in the era of highly active antiretroviral therapy. N Engl J Med. 2005;352:570–85.
Centers for Disease Control (US). Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMRW. 2006;55(14):1–17.
Simmons E, Roberts M, Ma M, et al. Routine testing for HIV in the United States: the intersection between recommendations and practices. AIDS Patient Care STDS. 2006;20(2):79–83.
Wenrich MD, Carline JD, Curtis JR, et al. Patient report of HIV risk screening by primary care physicians. Am J Prev Med. 1996;12(2):116–122.
Spielberg F, Branson BM, Goldbaum GM, et al. Overcoming barriers to HIV testing: preferences for new strategies among clients of a needle exchange, a sexually transmitted disease clinic, and sex venues for men who have sex with men. JAIDS. 2003;32(3):318–327.
Melnyk KAM. Barriers: a critical review of recent literature. Nurs Res. 1998;37:196–201.
Centers for Disease Control (US). Revised guidelines for HIV counseling, testing, and referral. MMWR. 2001;50(19):1–57.
Rothman RE, Lyons MS, Haukoos JS. Preventive care in the emergency department: should emergency departments conduct routine HIV screening? A systematic review. Acad Emerg Med. 2003;10(3):278–285.
Kelen GD, Shahan JB, Quinn TC. Emergency department-based HIV screening and counseling: experience with rapid and standard serologic testing. Ann Intern Med. 1999;33:147–55.
Centers for Disease Control (US). Technical guidance on HIV counseling. MMWR. 1993;42(2):5–9.
Centers for Disease Control (US). HIV counseling, testing and referral standards and Guidelines. Atlanta, GA: US Department of Health and Human Services, Public Health Service.
Rhew DC, Goetz MB, Shekelle PG. Evaluating quality indicators for patients with community-acquired pneumonia. Jt Comm J Qual Improv. 2001;27(11):575–590.
Phillips BR, LI Backus, JP Halloran, et al. Caring for veterans with HIV disease. Fiscal Year 2002 Report, Center for Quality Management in Public Health, Public Health Strategic Health Care Group, Department of Veterans Affairs, March, 2003.
US Department of Veterans Affairs, Public Law 100–322, Section 124: Testing for HIV (Human Immunodeficiency Virus) and Informed Consent. 1988.
Robson J, Boomla K, Fitzpatrick S, et al. Using nurses for preventive activities with computer assisted follow-up: a randomized controlled trial. BMJ. 1989;298:433–436.
Centers for Disease Control (US). Notice to readers: approval of a new rapid test for HIV antibody. MMWR. 2002;51(46):1051–1052.
Gerbert B, Bronstone A, McPhee S, et al. Development and testing of an HIV-risk screening instrument for use in health care settings. Am J Prev Med. 1998;15:103–113.
Mirand AL, Beehler GP, Kuo CL, et al. Explaining the de-prioritization of primary prevention: physicians’ perceptions of their role in the delivery of primary care. BMC Public Health. 2003;3:15.
Tudor-Hart J. Practice nurses: an underused resource. BMJ. 1985;290:1162–1163.
Spitzer WO, Sackett DL, Sibley JC, et al. The Burlington randomized trial of the nurse practitioner. N Engl J Med. 1974;290:251–256.
Gonzalez JJ, Ranney J, West J. Nurse-initiated health promotion prompting system in an internal medicine residents’ clinic. South Med J. 1989;82:3.
Stone EG, Morton SC, Hulscher ME, et al.. Interventions that increase use of adult immunization and cancer screening services: a meta-analysis. Ann Intern Med. 2002;136:641–651.
Centers for Disease Control (US). HIV counseling, testing and referral standards and guidelines. Atlanta, GA: US Department of Health and Human Services, Public Health Service, 1994;1–15.
Centers for Disease Control (US). Advancing HIV prevention. Interim Technical Guidance for Selected Interventions. Atlanta, GA: US Department of Health and Human Services, Public Health Service. 2003.
Spielberg F, Kurth A, Gorbach PM, et al. Moving from apprehension to action: HIV counseling and testing preferences in three at-risk populations. AIDS Educ Prev. 2001;13(6):524–540.
Center for Disease Control (US). Current trends: additional recommendations to reduce sexual and drug abuse-related transmission of human T-lymphotropic virus type III/lymphandenopathy-associated virus. MMWR. 1986;3:152–155.
Centers for Disease Control (US). Perspectives in disease prevention and health promotion: public health service guidelines for counseling and antibody testing to prevent HIV infection and AIDS. MMWR. 1987;36:509–515.
Centers for Disease Control (US). Guidelines for national human immunodeficiency virus case surveillance, including monitoring for human immunodeficiency virus infection and acquired immunodeficiency syndrome. MMWR. 1999;48131–28.
Molitor F, Bell RA, Truax SR. Predictors of failure to return for HIV test result and counseling by test site type. AIDS Educ Prev. 1999;11(1):1–13.
Josefson D. Rapid HIV testing urged in the United States. BMJ. 1998;316:1037.
Kassler WJ, Dillon BA, Haley C, et al. On-site, rapid HIV testing with same-day results and counseling. AIDS. 1997;8:1045–1051.
Kroc K, Kendrick S, Withum D, et al. Rapid HIV testing in an emergency department. Available at: http://www.cdc.gov/hiv/topics/testing/resources/abstracts/rt-emergency.htm Accessed September 12, 2006.
Farmham PG, Gorsky RD, Holtgrave DR, et al. Counseling and testing for HIV prevention: costs, effects, and cost-effectiveness of more rapid screening tests. Public Health Rep. 1996;111:44–53.
Metcalf CA, Douglas JM, Malotte CK, Cross H, Dillon BA, Paul SM, et al. Relative efficacy of prevention counseling with rapid and standard HIV testing: a randomized controlled trial (RESPECT-2). STDS. 2005;32:130–138.
Kamb ML, Fishbein M, Douglas JM, et al. Efficacy of risk-reduction counseling to prevent human immunodeficiency virus and sexually transmitted diseases: a randomized controlled trial. JAMA. 1998;280:1161–1167.
Sanders GD, Anaya H, Asch S, et al. Cost effectiveness of rapid HIV testing with streamlined counseling [abstract]. Proceedings of the 4th International AIDS Society Conference on HIV Pathogenesis, Treatment and Prevention, Sydney, Australia; July 22–25, 2008.
Acknowledgments
The authors would like to thank Genia Williamson, Leslie Lange, Brenda Rue, Alicia Alcantara, Jamie Feld, Anne Taylor, and Jesse Dwyer for assistance in the development of this manuscript.
This research reported here was supported by the Department of Veterans Affairs, Veterans Health Administration, Health Services Research and Development Service, Project number IIR 04–023. Dr. Asch is the principal investigator at the VA Greater Los Angeles Healthcare System. The views expressed in this article are those of the author(s) and do not necessarily represent the views of the United States Department of Veterans Affairs. The Veterans Health Administration supported this study but had no input in the design or reporting or decision to submit this paper for publication. HIV rapid tests were donated by Orasure Technologies. The opinions expressed in this manuscript are solely the authors’ and do not necessarily reflect those of the US Department of Veterans Affairs. This study was reviewed and sanctioned by a US Department of Veterans Affairs Internal Review Board process.
Conflict of Interest Statement
The first author owns stock in a biotechnology company that develops biotechnological products, one of which is a rapid test for diagnosing the HIV virus. The first author also received an unrestricted grant to support dissemination of research results from two HIV rapid testing device manufacturers, and this grant supported author no. 8 as well. Author no. 4 has received both honoraria and grant support in the past 3 years.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1: 2007 United States Department of Veteran’s Affairs Federally Mandated Pre-HIV Counseling Elements
The meaning, sensitivity and specificity of the HIV tests.
The potential social ramifications of a positive test result.
Policies and guidelines for confidentiality of the test results.
Policy on non-discrimination in health care services for patients with HIV infection and the health care services available in the VA.
Policy and guidelines on disclosure to public health authorities.
Policy on disclosure to spouse and/or sexual partner.
Measures to be taken for prevention of HIV transmission.
Information relative to authorized disclosures, either with or without consent of HIV test or treatment records.
Appendix 2: Composite Variable: HIV Knowledge
-
1.
One can get HIV by having sexual intercourse with an infected person without using a condom.
-
2.
One can get HIV by sharing drug needles with an infected person.
-
3.
An HIV-infected woman can infect her unborn child.
-
4.
One is not likely to get HIV using public facilities, such as buses and telephones.
-
5.
One is not likely to get HIV by kissing an HIV-infected person on the cheek.
-
6.
Not only homosexuals need to worry about contracting AIDS.
-
7.
People who are HIV-positive are easy to pick out of a crowd even if they have not developed AIDS.
-
8.
One is not likely to get HIV by attending school with an HIV-infected person.
-
9.
HIV-infected individuals could look and feel fine and be unaware that they could still spread the disease.
-
10.
AIDS is not just a gay man’s disease.
-
11.
Women are not at very low risk of getting HIV.
-
12.
One is not likely to get HIV using public toilets.
-
13.
One is not likely to get HIV from an animal or mosquito bite.
Appendix 3: Composite Variable: Sexual Risk
-
1.
What are your chances of getting infected with HIV?
-
2.
With how many casual sex partners have you engaged in high-risk sex?
-
3.
Have you had sex with this casual partner within the past 12 months?
-
4.
During the last 12 months, with how many people have you had sexual intercourse?
-
5.
Have you engaged in any of the following behaviors in the past 12 months?
Had sex with a partner who at the time was any of the following: another man (for male respondents), a man who has had sex with other men (for female respondents), a person who has injected non-prescription drugs, a person who has tested HIV-positive for HIV/AIDS?
OR:
Have you used any of the following substances in the past 12 months: injected non-prescription drugs, or used marijuana, cocaine, or hallucinogens (e.g., LSD mushrooms)?
Rights and permissions
About this article
Cite this article
Anaya, H.D., Hoang, T., Golden, J.F. et al. Improving HIV Screening and Receipt of Results by Nurse-Initiated Streamlined Counseling and Rapid Testing. J GEN INTERN MED 23, 800–807 (2008). https://doi.org/10.1007/s11606-008-0617-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-008-0617-x