
Abstract
Background
Fast-track (FT) protocols accelerate patient's recovery and shorten hospital stay as a result of the optimization of the perioperative care they offer. The aim of this review is to examine the latest evidence for fast-track protocols when compared with standard care in elective colorectal surgery involving segmental colonic and/or rectal resection.
Materials and methods
All randomized controlled trials and controlled clinical trials on FT colorectal surgery were reviewed systematically. The main end points were short-term morbidity, length of primary postoperative hospital stay, length of total postoperative stay, readmission rate, and mortality. Quality assessment and data extraction were performed independently by two observers.
Results
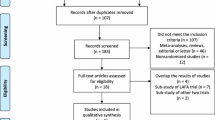
Eleven studies were eligible for analysis (four randomized controlled trials (RCTs) and seven controlled clinical trials (CCT)), including 1,021 patients. Primary hospital stay (weighted mean difference −2.35 days, 95% confidence interval (CI) −3.24 to −1.46 days, P < 0.00001) and total hospital stay (weighted mean difference −2.46 days, 95% CI −3.43 to −1.48 days, P < 0.00001) were significantly lower for FT programs. Morbidity was also lower in the FT group. Readmission rates were not significantly different. No increase in mortality was found.
Conclusions
FT protocols show high-level evidence on reducing primary and total hospital stay without compromising patients' safety offering lower morbidity and the same readmission rates. Enhanced recovery programs should become a mainstay of elective colorectal surgery.





Similar content being viewed by others


References
Arenal JJ, Benito C, Concejo MP, Ortega E (1999) Colorectal resection and primary anastomosis in patients aged 70 and older: prospective study. Eur J Surg 165(6):593–597
Bokey EL, Chapuis PH, Fung C, Hughes WJ, Koorey SG, Brewer D, Newland RC (1995) Postoperative morbidity and mortality following resection of the colon and rectum for cancer. Dis Colon Rectum 38(5):480–486 discussion 486–487
Retchin SM, Penberthy L, Desch C, Brown R, Jerome-D'Emilia B, Clement D (1997) Perioperative management of colon cancer under Medicare risk programs. Arch Intern Med 157(16):1878–1884
Basse PH, Whiteside TL, Herberman RB (2000) Use of activated natural killer cells for tumor immunotherapy in mouse and human. Methods Mol Biol 121:81–94
Kehlet H, Mogensen T (1999) Hospital stay of 2 days after open sigmoidectomy with a multimodal rehabilitation programme. Br J Surg 86(2):227–230
Anderson AD, McNaught CE, MacFie J, Tring I, Barker P, Mitchell CJ (2003) Randomized clinical trial of multimodal optimization and standard perioperative surgical care. Br J Surg 90(12):1497–1504
Basse L, Raskov HH, Hjort Jakobsen D, Sonne E, Billesbolle P, Hendel HW, Rosenberg J, Kehlet H (2002) Accelerated postoperative recovery programme after colonic resection improves physical performance, pulmonary function and body composition. Br J Surg 89(4):446–453
Delaney CP, Zutshi M, Senagore AJ, Remzi FH, Hammel J, Fazio VW (2003) Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional postoperative care after laparotomy and intestinal resection. Dis Colon Rectum 46(7):851–859
Fearon KC, Ljungqvist O, Von Meyenfeldt M, Revhaug A, Dejong CH, Lassen K, Nygren J, Hausel J, Soop M, Andersen J, Kehlet H (2005) Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 24(3):466–477
Gatt M, Anderson AD, Reddy BS, Hayward-Sampson P, Tring IC, MacFie J (2005) Randomized clinical trial of multimodal optimization of surgical care in patients undergoing major colonic resection. Br J Surg 92(11):1354–1362
Jakobsen DH, Sonne E, Andreasen J, Kehlet H (2006) Convalescence after colonic surgery with fast-track vs conventional care. Colorectal Dis 8(8):683–687
Kehlet H (2005) Fast-track colonic surgery: status and perspectives. Recent Results Cancer Res 165:8–13
Khoo C, Vickery C, Forsyth N, Vinall N, Eyre-Brook I (2007) A prospective randomised control trial (RCT) of multimodal perioperative management protocol in patients undergoing elective colorectal resection for cancer. Ann Surg 245:867–872
Polle SW, Wind J, Fuhring JW, Hofland J, Gouma DJ, Bemelman WA (2007) Implementation of a fast-track perioperative care program: what are the difficulties? Dig Surg 24(6):441–449
Senagore AJ, Duepree HJ, Delaney CP, Brady KM, Fazio VW (2003) Results of a standardized technique and postoperative care plan for laparoscopic sigmoid colectomy: a 30-month experience. Dis Colon Rectum 46(4):503–509
Senagore AJ, Madbouly KM, Fazio VW, Duepree HJ, Brady KM, Delaney CP (2003) Advantages of laparoscopic colectomy in older patients. Arch Surg 138(3):252–256
Podore PC, Throop EB (1999) Infrarenal aortic surgery with a 3-day hospital stay: a report on success with a clinical pathway. J Vasc Surg 29(5):787–792
Tovar EA, Roethe RA, Weissig MD, Lloyd RE, Patel GR (1998) One-day admission for lung lobectomy: an incidental result of a clinical pathway. Ann Thorac Surg 65(3):803–806
Pritts TA, Nussbaum MS, Flesch LV, Fegelman EJ, Parikh AA, Fischer JE (1999) Implementation of a clinical pathway decreases length of stay and cost for bowel resection. Ann Surg 230(5):728–733
Wind J, Polle SW, Fung Kon Jin PH, Dejong CH, von Meyenfeldt MF, Ubbink DT, Gouma DJ, Bemelman WA (2006) Systematic review of enhanced recovery programmes in colonic surgery. Br J Surg 93(7):800–809
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17(1):1–12
Basse L, Thorbol JE, Lossl K, Kehlet H (2004) Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum 47(3):271–277 discussion 277–278
Bradshaw BG, Liu SS, Thirlby RC (1998) Standardized perioperative care protocols and reduced length of stay after colon surgery. J Am Coll Surg 186(5):501–506
Hjort Jakobsen D, Sonne E, Basse L, Bisgaard T, Kehlet H (2004) Convalescence after colonic resection with fast-track versus conventional care. Scand J Surg 93(1):24–28
Kariv Y, Delaney CP, Senagore AJ, Manilich EA, Hammel JP, Church JM, Ravas J, Fazio VW (2007) Clinical outcomes and cost analysis of a “fast track” postoperative care pathway for ileal pouch-anal anastomosis: a case control study. Dis Colon Rectum 50(2):137–146
Nygren J, Hausel J, Kehlet H, Revhaug A, Lassen K, Dejong C, Andersen J, von Meyenfeldt M, Ljungqvist O, Fearon KC (2005) A comparison in five European Centres of case mix, clinical management and outcomes following either conventional or fast-track perioperative care in colorectal surgery. Clin Nutr 24(3):455–461
Raue W, Haase O, Junghans T, Scharfenberg M, Muller JM, Schwenk W (2004) ‘Fast-track’ multimodal rehabilitation program improves outcome after laparoscopic sigmoidectomy: a controlled prospective evaluation. Surg Endosc 18(10):1463–1468
Stephen AE, Berger DL (2003) Shortened length of stay and hospital cost reduction with implementation of an accelerated clinical care pathway after elective colon resection. Surgery 133(3):277–282
Wichmann MW, Eben R, Angele MK, Brandenburg F, Goetz AE, Jauch KW (2007) Fast-track rehabilitation in elective colorectal surgery patients: a prospective clinical and immunological single-centre study. Aust N Z J Surg 77(7):502–507
Kehlet H, Buchler MW, Beart RW Jr, Billingham RP, Williamson R (2006) Care after colonic operation—is it evidence-based? Results from a multinational survey in Europe and the United States. J Am Coll Surg 202(1):45–54
Lassen K, Hannemann P, Ljungqvist O, Fearon K, Dejong CH, von Meyenfeldt MF, Hausel J, Nygren J, Andersen J, Revhaug A (2005) Patterns in current perioperative practice: survey of colorectal surgeons in five northern European countries. BMJ 330(7505):1420–1421
Maessen J, Dejong CH, Hausel J, Nygren J, Lassen K, Andersen J, Kessels AG, Revhaug A, Kehlet H, Ljungqvist O, Fearon KC, von Meyenfeldt MF (2007) A protocol is not enough to implement an enhanced recovery programme for colorectal resection. Br J Surg 94(2):224–231
Kehlet H (2008) Fast-track colorectal surgery. Lancet 371(9615):791–793
Basse L, Jakobsen DH, Bardram L, Billesbolle P, Lund C, Mogensen T, Rosenberg J, Kehlet H (2005) Functional recovery after open versus laparoscopic colonic resection: a randomized, blinded study. Ann Surg 241(3):416–423
King PM, Blazeby JM, Ewings P, Franks PJ, Longman RJ, Kendrick AH, Kipling RM, Kennedy RH (2006) Randomized clinical trial comparing laparoscopic and open surgery for colorectal cancer within an enhanced recovery programme. Br J Surg 93(3):300–308
MacKay G, Ihedioha U, McConnachie A, Serpell M, Molloy RG, O'Dwyer PJ (2007) Laparoscopic colonic resection in fast-track patients does not enhance short-term recovery after elective surgery. Colorectal Dis 9(4):368–372
Andersen J, Hjort-Jakobsen D, Christiansen PS, Kehlet H (2007) Readmission rates after a planned hospital stay of 2 versus 3 days in fast-track colonic surgery. Br J Surg 94(7):890–893
Hammer J, Harling H, Wille-Jorgensen P (2008) Implementation of the scientific evidence into daily practice—example from fast-track colonic cancer surgery. Colorectal Dis 10(6):593–598
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gouvas, N., Tan, E., Windsor, A. et al. Fast-track vs standard care in colorectal surgery: a meta-analysis update. Int J Colorectal Dis 24, 1119–1131 (2009). https://doi.org/10.1007/s00384-009-0703-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-009-0703-5