Article Text

Abstract
Objectives To evaluate the efficacy and safety of anti-vascular endothelial growth factor (VEGF) agents and corticosteroids for the treatment of macular oedema (ME) secondary to central retinal vein occlusion (CRVO).
Design Systematic review and network meta-analysis.
Participants Patients from previously reported randomised controlled trials (RCTs) comparing anti-VEGF and corticosteroids for the treatment of ME secondary to CRVO.
Methods Literature searches were conducted using PubMed, Medline, Embase, Cochrane Library and clinicaltrials.gov until March 2017. Therapeutic effects were estimated using the proportions of patients gaining/losing ≥15 letters, best-corrected visual acuity (BCVA) and central retinal thickness (CRT). Treatment safety was estimated using the proportions of adverse events, namely increased intraocular pressure (IOP), cataracts, vitreous haemorrhage (VH) and retinal tear. The software ADDIS (V.1.16.8) was used for analysis. Treatment effect and safety of different drugs could be ranked based on simulation.
Results Eleven RCTs comprising 2060 patients were identified. Regarding patients gaining ≥15 letters, aflibercept and ranibizumab were significantly more effective than sham/placebo at 6 months. Regarding patients losing ≥15 letters at 6 months, ranibizumab showed significant improvement compared with dexamethasone. Aflibercept, bevacizumab or ranibizumab showed greater improvements in BCVA than sham/placebo at 6 months. Intravitreal ranibizumab injection demonstrated greater CRT reduction than both sham and dexamethasone did. Dexamethasone had a higher risk of increased IOP than aflibercept and ranibizumab. Ranibizumab demonstrated a greater risk of cataracts than dexamethasone. Aflibercept and ranibizumab demonstrated low incidence of VH and retinal tear, respectively. Aflibercept had a slight advantage over ranibizumab as assessed by benefit–risk analysis.
Conclusions Anti-VEGF agents have advantages in the treatment of ME secondary to CRVO. Aflibercept and ranibizumab showed marked BCVA improvement and CRT reduction. Aflibercept may have a slight advantage over ranibizumab. The results of this study can serve as a reference for clinicians to provide patient-tailored treatment.
PROSPERO registration number CRD42017064076.
- central retinal vein occlusion (CRVO)
- macular edema
- anti-VEGF
- corticosteroid
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This meta-analysis included the most recent reports.
Strict inclusion and exclusion criteria were used to perform a comprehensive comparison of aflibercept, ranibizumab, bevacizumab, pegaptanib, dexamethasone and triamcinolone treatments.
Our data contained some biases that might have influenced our results. In the 11 literature included, three of them did not illustrate blinding of participants and two of them reported incomplete outcome data.
Detailed data at long-term follow-up time points are required to improve the accuracy and robustness of our findings.
The details of adverse events were not always reported in each study.
Introduction
Central retinal vein occlusion (CRVO), a common retinal vascular disorder, is characterised by dilated and tortuous retinal veins with haemorrhages in all four quadrants of the retina.1 2 CRVO can reduce vision severely,3 4 and its prevalence is estimated at 0.80 per 1000 persons, indicating that approximately 2.5 million adults are affected by CRVO globally.1 CRVO is caused by a combination of risk factors, including advanced age, atherosclerosis, hypertension, diabetes mellitus, thrombophilia, hyperlipidaemia, glaucoma and other vessel wall changes or haemodynamic abnormalities.5 6 Macular oedema (ME) is the most common complication in CRVO that can lead to impaired central vision,7 and ME secondary to CRVO is the second most common retinal vascular disease after diabetic retinopathy.1 8 9
The serious consequences of CRVO and its increasing prevalence make effective and widely applicable treatments necessary. Preventing ME and improving visual acuity (VA) are the two most important goals of treatment of ME secondary to CRVO. During the past several decades, various therapeutic approaches have been advocated for CRVO. The Central Vein Occlusion Study demonstrated that macular grid photocoagulation could decrease ME in patients with CRVO; however, it failed to improve VA when compared with that in the observation group.10 11 Although intravitreal corticosteroid agents (eg, triamcinolone acetonide injections and dexamethasone implants), which have anti-inflammatory, antiangiogenic and antioedematous properties,12 demonstrate some adverse events (AEs), they have been used to treat ME and improve VA in CRVO patients. Intravitreal triamcinolone has recently been shown to have a beneficial effect on ME secondary to CRVO and a preventive effect on neovascularisation.13–15 Kuppermann et al also reported that dexamethasone implants might be a potential treatment option for persistent ME.16
Vascular endothelial growth factor (VEGF) is a homodimeric protein that can stimulate vascular endothelial cell growth and induce vascular permeability.17 It plays a crucial role in the pathophysiology process of ME,18 and its levels were elevated in the ocular fluids of patients with CRVO.19 Therefore, several anti-VEGF agents, including aflibercept, ranibizumab, bevacizumab and pegaptanib, have been widely used for treating ME secondary to CRVO, because they significantly improve visual and anatomic outcomes in CRVO patients.20–23
Currently, intravitreal corticosteroid agents and intravitreal anti-VEGF agents are the common clinical therapies for ME secondary to CRVO. Nevertheless, these different drug treatment strategies have not been comprehensively compared, and there are no head-to-head trials or clear guidance to determine the best treatment strategy for CRVO patients. Therefore, a systematic review of randomised controlled trials (RCTs) is needed to indirectly compare the efficacies of anti-VEGF agents and intravitreal corticosteroids agents for treating ME secondary to CRVO.
A previous network meta-analysis of RCTs that examined CRVO treatments had mainly focused on the efficacy outcomes at 6 months and failed to include pegaptanib.24 In addition, it only considered the functional outcomes (eg, letters gained and VA improvement) as therapeutic effects without consideration of anatomical outcomes and AEs. Therefore, the current systematic review and network meta-analysis was performed to overcome the shortcomings of the previous study and to include data from the latest RCTs. In the present study, we aimed to indirectly compare the clinical efficacy and safety of aflibercept, ranibizumab, bevacizumab, pegaptanib, dexamethasone and triamcinolone for the treatment of ME secondary to CRVO. The clinical efficacy outcomes include best-corrected visual acuity (BCVA) improvement, central retinal thickness (CRT) reduction and the proportion of ≥15 letters gained or lost. The safety outcomes include the proportion of common AEs, such as increased intraocular pressure (IOP), cataracts, neovascular glaucoma and vitreous haemorrhage (VH). We hope that our findings will aid ophthalmologists in choosing the best treatment options for their patients.
Methods
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement, and the review was conducted and reported according to the PRISMA network meta-analysis (NMA) Checklist of items (see online supplementary appendix 1).25 26 We developed a systematic review protocol and registered it with PROSPERO (CRD42017064076). (Available from http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42017064076).
Supplementary file 1
Patient and public involvement
We used secondary data from peer-reviewed published articles, so no patients or public were not involved in this network meta-analysis.
Literature search
Literature searches were performed using five databases (Embase, Medline, Pubmed Central, Cochrane Library and ClinicalTrials.gov) to identify relevant articles published until the end of March 2017. The following terms were searched in each database: central retinal vein occlusion (CRVO), anti-VEGF agents, corticosteroids and RCTs. The full search strategies are described in online supplementary appendix 2. In addition, supplementary searches were performed to search for other relevant studies in the WHO International Clinical Trials Registry Platform, Google Scholar and other websites of professional associations. Language or study design restrictions were not used. When titles or abstracts or both fit our search terms, abstracts were reviewed to exclude irrelevant studies (eg, case reports, reviews or experimental treatments). We then carefully read all the remaining articles to determine if they contained data that were applicable to our study.
Supplementary file 2
Article inclusion/exclusion criteria
In this network meta-analysis, studies were selected based on the following inclusion criteria: (1) The study was an RCT. (2) Ranibizumab, bevacizumab, aflibercept, pegaptanib dexamethasone or triamcinolone was used. (3) Subjects were adults (≥18 years) of either sex with ME secondary to CRVO. (4) Studies had to report at least one of the following outcomes: proportions of patients gaining/losing ≥15 letters (three lines) from baseline to 6 or 12 months, the mean change in BCVA from baseline to 6 or 12 months, the mean change in CRT from baseline to 6 or 12 months or the proportions of patients with AEs at 6 or 12 months. Studies that met any of the following criteria were excluded from our meta-analysis: (1) review article, (2) duplicate publication, (3) sufficient information not published (eg, full text not accessible, full text did not contain raw data or inconsistent or erroneous data provided) and (4) subjects with CRVO did not have ME prior to treatment.
Risk of bias assessment
The included studies were examined independently for biases by two authors using Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions.27 The following study characteristics were assessed for biases: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias) and other factors that contribute to biases (eg, extreme baseline imbalance, study design and trial stopped early because of data-dependent developments). The status of each of the above items was listed as ‘yes’ to indicate a low risk, ‘no’ to indicate a high risk or ‘unclear’ to indicate an unknown risk of bias.
Data extraction
The following information on study characteristics and clinical treatments were collected from all included studies:
Basic information
Name of first author, year of publication, design of trial, location of study, setting, follow-up time, clinical trial registration
Participants and criteria
Baseline characteristics (age, gender, baseline VA, baseline CRT, duration of ME, etc), inclusion criteria, exclusion criteria
Interventions
Different treatment groups and number of patients included
Outcomes
Primary outcomes, other outcomes, outcome assessment
Some data that were not reported in articles were published online at ClinicalTrials.gov or other meta-analyses. TQ and MZ carried out search and extracted data. If disagreements occurred, XX would check the data again.
Evaluation indicator
The indicators of treatment efficacy included the proportions of patients gaining/losing ≥15 letters from baseline to 6 or 12 months and the mean changes in BCVA and CRT. The safety indicators included the proportions of patients with various AEs.
Statistical analyses
Our analysis classified anti-VEGF agents and corticosteroids used in monotherapy as separate treatment nodes irrespective of their doses: aflibercept, ranibizumab, bevacizumab, pegaptanib, dexamethasone, triamcinolone and placebo or sham (ie, conventional therapy/usual care).
Network meta-analysis allows the integration of data from both direct and indirect evidence, and it can be used to estimate comparisons between pairs of treatments that have not been compared in individual studies.28 29 The network meta-analysis was performed within a Bayesian framework by using the Markov Chain Monte Carlo method.30 The measures of treatment effects were relative risk (RR) for dichotomous outcomes and the weighted mean difference for continuous outcomes. Bayesian statistical inference provides probability distributions for treatment effect parameters, with 95% credible intervals (95% CrI), which can be interpreted as a 95% probability that the parameter takes a value within the specified range.31 32 If 1.0 was not included in the 95% CrI, the results were considered statistically significant. Consistency analysis could be performed in the presence of similarity and homogeneity, and on this basis, it is possible to rank the effect of different treatment strategies. The higher ranking means the better the treatment is. But when considering the AE, the higher ranking means the more probability of AE. When performing this network meta-analysis, we relied on the assumptions of transitivity and consistency.33 The consistency of results was qualitatively examined if sufficient evidence was available. If both direct and indirect evidences existed, node-splitting and pairwise meta-analyses were used to evaluate the inconsistency of direct comparisons in indirect evidences in the network meta-analysis.34 In order to analyse the direct and indirect evidences in accordance with the split node, the node-splitting assessment is necessary. And p<0.05 indicates significant heterogeneity in this assessment.
The data of the included studies were analysed using the STATA V.14 (StataCorp LP, College Station, Texas, USA)35 and the Aggregate Data Drug Information System (ADDIS V.1.16.8, Drugis, Groningen, NL).36 The risk of bias graph was drawn using Review Manager V.5.3.5 software. During data analysis, four parallel chains were used and 50 000 samples were obtained after a 20 000-sample burn-in in each chain.37 Convergence was assessed using the Brooks-Gelman-Rubin method. This method compares within-chain and between-chain variance to calculate the potential scale reduction factor (PSRF). A PSRF close to one indicates that approximate convergence has been reached.38
Results
Literature search results
The PRISMA flowchart of the selection process of studies included in this network meta-analysis is illustrated in figure 1. In total, 1032 articles were initially identified in our literature searches. Of these, 556 articles were potentially relevant and screened after duplicates had been removed. A title and abstract review eliminated an additional 508 articles. Full-text examinations excluded seven additional articles2 15 39–43 (seven studies) owing to various reasons. Finally, 41 articles20 23 44–82 (11 studies) were included in this systematic review and network meta-analysis. The specific literature of both included and excluded studies is shown in online supplementary appendix 3.
Supplementary file 3
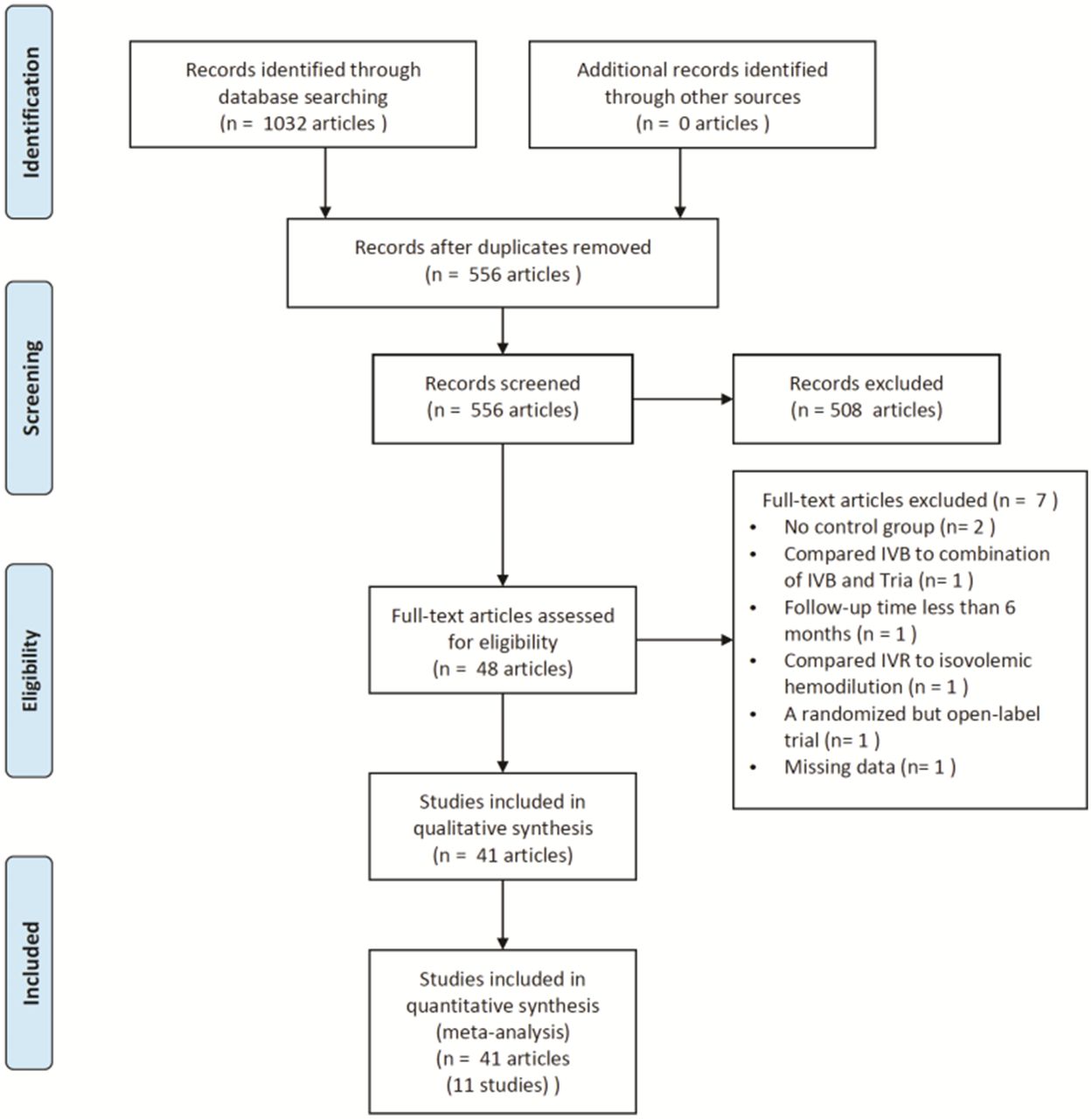
Study selection flow diagram. IVB, intravitreal bevacizumab injections.
Characteristics and outcomes of included studies
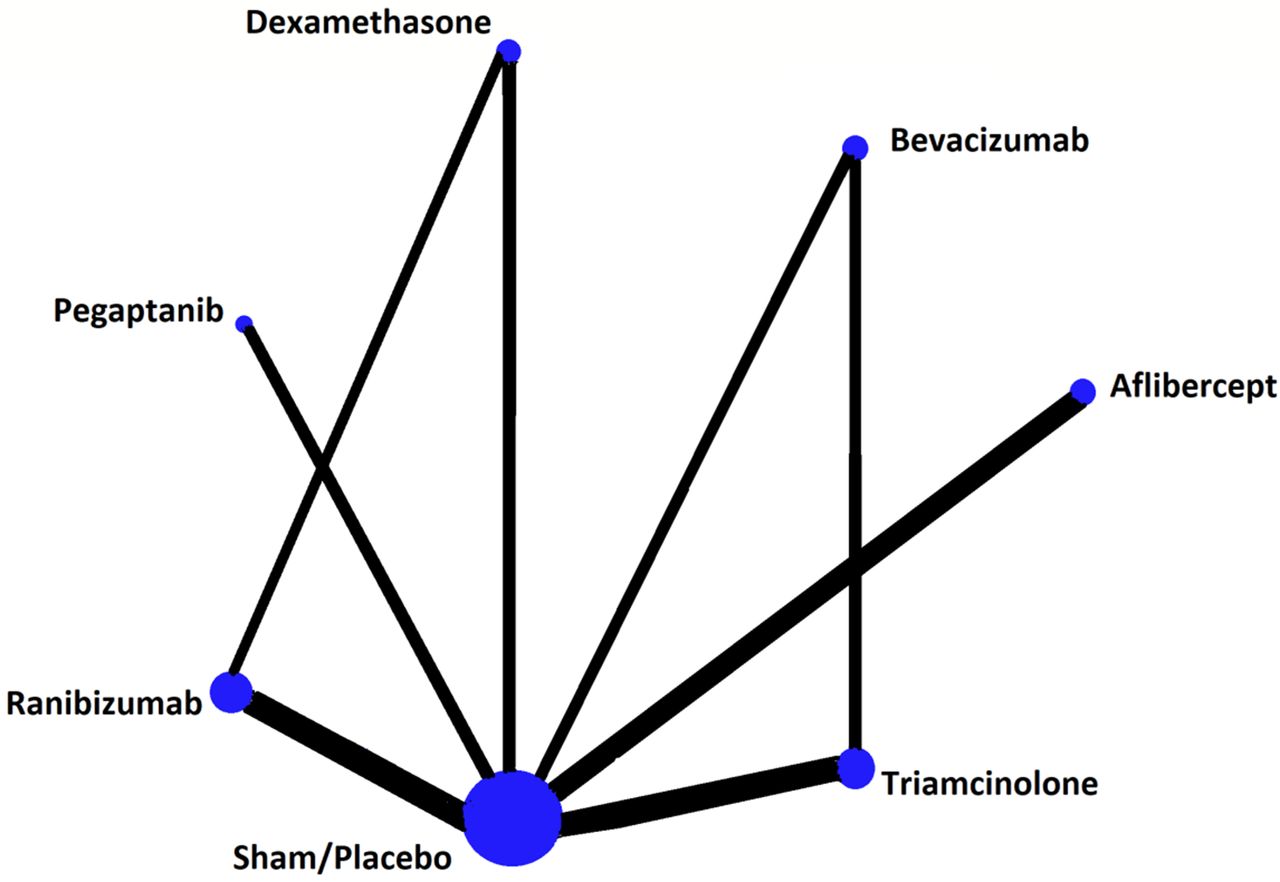
Eleven studies comprising 2060 patients with ME secondary to CRVO were included in this meta-analysis. A network graph was constructed to show the network of eligible comparisons for the network meta-analysis (figure 2). Briefly, the follow-up duration was at least 6 months and the patients’ ages and gender distributions did not vary significantly among different drug treatment groups. The median sample size was 174 individuals (range 29–437). The main characteristics of the 11 included studies are presented in table 1. The detailed study results are presented in online supplementary appendix 4.
Supplementary file 4

Network graph of all treatment comparisons for all studies. Each node represents one drug. The size of nodes is proportional to the number of randomised participants (sample size). Lines represent direct comparisons within randomised controlled trials, and the width of the lines is proportional to the number of trials comparing each pair of treatments.
Study characteristics of the 11 randomised controlled trials enrolled
Methodological quality of included studies
The biases of the 11 included studies were assessed using the Cochrane Collaboration’s tool as listed in online supplementary appendix 5. Each risk of bias item is expressed as a percentage across all included studies in figure 3. In terms of methodological quality, three trials (27.3%) had a high risk of bias.
Supplementary file 5

Risk of bias graph: review authors’ judgements about each risk of bias item are presented as percentages across all included studies.
Efficacy of interventions on the proportions of patients with gaining/losing ≥15 letters at 6 or 12 months
The improvement of VA was the most important functional measure of treatment efficacy. The proportions of patients gaining ≥15 letters were considered the primary outcome in many included studies. Table 2 shows the RR and 95% CrI in the proportions of patients gaining and losing ≥15 letters from baseline for all possible comparisons at 6 months using the consistency model.
Network meta-analysis results in ≥15 letters gained (lower part) and lost (upper part) at 6 months
In terms of the proportions of patients gaining ≥15 letters, aflibercept (RR 6.97, 95% CrI 1.73 to 29.70), bevacizumab (RR 6.23, 95% CrI 0.76 to 59.04), dexamethasone (RR 1.22, 95% CrI 0.24 to 5.85), pegaptanib (RR 1.54, 95% CrI 0.18 to 13.37), ranibizumab (RR 6.04, 95% CrI 1.15 to 29.10) and triamcinolone (RR 6.97, 95% CrI 1.73 to 29.70) are more likely to have a positive effect in treatment of CRVO than sham/placebo treatment at 6 months. Among them, aflibercept and ranibizumab were significantly superior to the sham/placebo group. Ranibizumab was significantly superior to dexamethasone (p=0.04, 95% CrI 0.00 to 0.09) in terms of the proportions of patients losing ≥15 letters. Table 3 shows the rank probabilities of these drugs for the treatment of CRVO according to the proportions of patients gaining ≥15 letters at 6 months, while table 4 shows the rank probabilities of the proportions of patients losing ≥15 letters at 6 months.
Ranking based on simulations for gaining ≥15 letters at 6 months
Ranking based on simulations for losing ≥15 letters at 6 months
Because some specific data were not extracted or reported, the outcomes of the proportions of patients gaining/losing ≥15 letters at 12 months did not involve all drugs. Table 5 shows the RR and 95% CrI in proportions of patients gaining and losing ≥15 letters from baseline for all possible comparisons at 12 months using the consistency model.
Network meta-analysis results in ≥15 letters gained (lower part) and lost (upper part) at 12 months
In terms of the proportions of patients gaining ≥15 letters at 12 months, aflibercept (RR 3.08, 95% CrI 0.99 to 8.85), bevacizumab (RR 3.26, 95% CrI 0.56 to 17.47), dexamethasone (RR 1.40, 95% CrI 0.32 to 6.14), ranibizumab (RR 2.08, 95% CrI 0.45 to 10.09) and triamcinolone (RR 5.21, 95% CrI 0.91 to 31.67) are more likely to have a positive effect in the treatment of CRVO than sham/placebo treatment at 12 months; however, the differences were not significantly different. Table 6 shows the rank probabilities of these drugs for the treatment of CRVO according to the proportions of patients gaining ≥15 letters at 12 months, while table 7 shows the rank probabilities of the proportions of patients losing ≥15 letters at 12 months.
Ranking based on simulations for gaining ≥15 letters at 12 months
Ranking based on simulations for losing ≥15 letters at 12 months
Efficacy of interventions on the mean changes in BCVA from baseline at 6 months
Table 8 shows the mean changes and 95% CrI of BCVA improvement for all possible comparisons by the network meta-analysis using the consistency model. Patients treated with aflibercept (RR 17.88, 95% CrI 7.59 to 29.11), bevacizumab (RR 19.32, 95% CrI 5.17 to 33.11) and ranibizumab (RR 13.78, 95% CrI 1.58 to 24.91) showed greater improvements in BCVA than those treated with sham/placebo group at 6 months, and the differences were significant. Triamcinolone (RR 7.48, 95% CrI −6.05 to 20.78) was also superior to sham injection, but the difference was not significant. Overall, patients treated with anti-VEGF agents (aflibercept, ranibizumab or bevacizumab) had a higher probability of improvement in BCVA than those treated with corticosteroid agents (triamcinolone or dexamethasone).
Network meta-analysis results in BCVA changes (lower part) and CRT changes (upper part) at 6 months
Table 9 shows the rank probability of these drugs for the treatment of CRVO according to the BCVA improvement at 6 months.
Ranking based on simulations for BCVA changes from baseline at 6 months
Efficacy of interventions on mean changes in CRT from baseline at 6 months
The CRT represents anatomic changes in the fovea after treatment. As certain studies did not report CRT changes after treatment, the evaluation of CRT only involved ranibizumab, dexamethasone and sham injections. Intravitreal ranibizumab injections showed greater reduction in CRT than both sham injection (RR −156.80, 95% CrI −452.68 to 144.63) and dexamethasone (RR −205.30, 95% CrI −470.88 to 64.62). Table 10 shows the rank probability of these three drugs for the treatment of CRVO according to CRT reductions at 6 months.
Ranking based on simulations for CRT changes from baseline at 6 months
Adverse events
Many AEs were reported after drug treatment in the 11 studies, which comprised 2060 patients (table 11). The most common ocular AE reported in more than two studies that could be compared by network meta-analysis were increased IOP, cataracts, VH and retinal tear.
Main adverse events after drug treatment reported according to the included studies
Consistency analysis of network model
Based on direct versus indirect evidence, we compared the effect estimate twice using node-splitting, considering that direct and indirect evidences existed together. The first was the comparison of ranibizumab, dexamethasone and sham/placebo, while the second was bevacizumab, triamcinolone and sham/placebo. Table 12 shows the comparisons of the estimated quantiles for the direct and indirect evidence, as well as the combined evidence. No inconsistencies were observed (p>0.05). These data suggest that our model is relatively robust.
Node-splitting meta-analysis of two comparison
Benefit–risk analysis between anti-VEGF agents and dexamethasone
For the purpose of the proposed methods, benefit–risk analysis is defined as the quantitative synthesis of drug efficacy (or effectiveness) and AE profile.83 Based on the existing data from the included studies, benefit–risk analysis could be performed if efficacy outcomes and safety outcomes were both reported at the same time. When considering gaining ≥15 letters at 6 months as a benefit index and increased IOP as a risk index, aflibercept and ranibizumab were superior to dexamethasone in the treatment of ME secondary to CRVO (figure 4). When considering gaining ≥15 letters at 6 months as a benefit index and cataracts as a risk index, ranibizumab exhibited a greater benefit of visual improvement as well as a higher risk of cataracts than dexamethasone (figure 5).
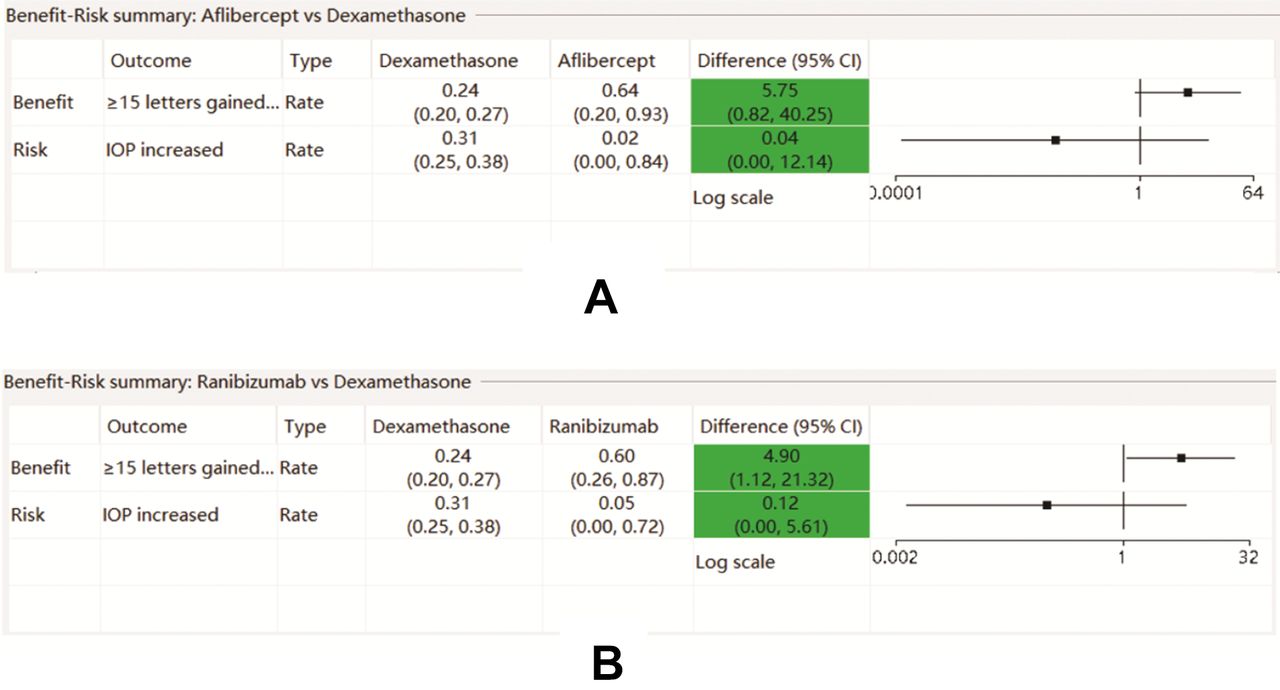
Benefit–risk analysis of aflibercept and ranibizumab versus dexamethasone considering gaining ≥15 letters and increased intraocular pressure (IOP): (A) aflibercept versus dexamethasone; (B) ranibizumab versus dexamethasone. Key benefit–risk summary with embedded relative effect forest plot. The colour in the ‘difference’ column indicates whether the point estimate favours dexamethasone (red) or aflibercept/ranibizumab (green). The symbol in the forest plot indicates whether the logarithmic (square) scale is used.

Benefit–risk analysis of ranibizumab versus dexamethasone considering gaining ≥15 letters and cataracts. Key benefit–risk summary table with embedded relative effect forest plot. The colour in the ‘difference’ column indicates whether the point estimate favours dexamethasone (red) or ranibizumab (green). The symbol in the forest plot indicates whether the logarithmic (square) scale is used.
Benefit– risk analysis of aflibercept versus ranibizumab
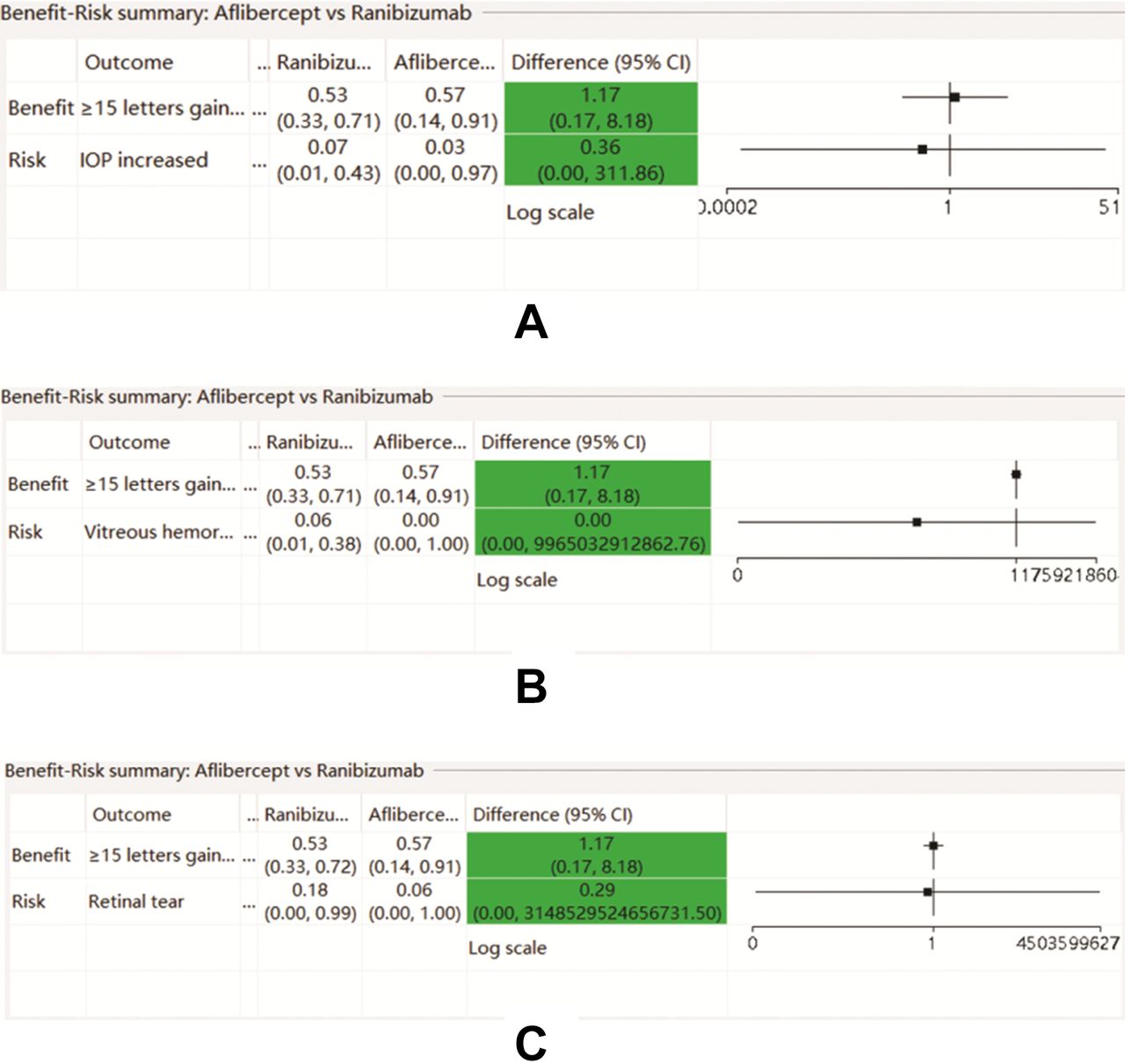
Aflibercept and ranibizumab are the two most widely used anti-VEGF agents in the treatment of CRVO worldwide. However, there are few head-to-head RCTs comparing the efficacy and safety of aflibercept and ranibizumab directly. Gaining ≥15 letters at 6 months was considered a benefit index; and increased IOP, vitreous haemorrhage, and retinal tear were considered risk indexs. Thus, aflibercept exhibited slightly better visual improvement and a lower risk of the latter three AE than ranibizumab (figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Benefit–risk analysis of aflibercept versus ranibizumab considering gaining ≥15 letters at 6 months and the three main adverse events: (A) increased intraocular pressure (IOP); (B) vitreous haemorrhage; (C) retinal tear. Key benefit–risk summary table with embedded relative effect forest plot. The colour in the ‘difference’ column indicates whether the point estimate favours ranibizumab (red) or aflibercept (green). The symbol in the forest plot indicates whether the logarithmic (square) scale is used.
Discussion
Intravitreal corticosteroids12 (triamcinolone or dexamethasone) and intravitreal anti-VEGF drugs84 85 are both therapeutic options for CRVO patients despite their limitations. It is important that comparisons of the efficacy and safety of intravitreal anti-VEGF injection and intravitreal corticosteroids are needed in patients with ME secondary to CRVO.
In terms of the proportions of patients gaining ≥15 letters at 6 months, our results showed that only aflibercept and ranibizumab had a significantly better efficacy than the sham/placebo group. Between the four main anti-VEGF agents and the two corticosteroids, our results showed no evidence of differences in effectiveness at both 6 and 12 months. According to the rank probability of the existing data, aflibercept, bevacizumab and triamcinolone are the best three drugs, with no statistical significance, in gaining ≥15 letters at 6 and 12 months. However, bevacizumab and triamcinolone were used off-label and lacked safety data. Therefore, aflibercept would be considered the first choice to improve VA in the treatment of ME secondary to CRVO. Aflibercept targets a wider range of cytokines and may have a stronger binding affinity,86 which could explain the greater efficacy in visual improvement, than ranibizumab, bevacizumab and pegaptanib. Unlike corticosteroids, anti-VEGF could decrease the vitreal levels of VEGF. Aflibercept and ranibizumab exhibited significantly better efficacy at 6 months but not at 12 months, indicating that the effects of aflibercept and ranibizumab were less obvious than the effects of the sham/placebo group as the follow-up time progressed.
In terms of the proportion of patients that lost ≥15 letters at 6 or 12 months, the pooled result showed that only ranibizumab was superior to dexamethasone, with a significant difference at 6 months. Although no significant difference was found among the other drug treatment groups, anti-VEGF agents showed a tendency toward better efficacy in visual improvement than corticosteroids did. Among the anti-VEGF agents, ranibizumab had the lowest risk of patients losing ≥15 letters.
Apart from the ≥15 letters gained or lost, BCVA changes from baseline could reflect visual recovery. At 6 months, aflibercept, bevacizumab and ranibizumab showed a greater improvement in BCVA than the sham/placebo group, with a statistically significant difference. The results support the efficacy of anti-VEGF agents for VA improvement to some extent, which is consistent with the aforementioned results of ≥15 letters gained or lost. In the case of visual improvement, anti-VEGF agents, especially ranibizumab and aflibercept, were better than corticosteroids.
CRT, an anatomical index reflecting macular, was also considered as an important outcome to estimate the efficacy of these drugs. Only three RCTs reported a CRT reduction. According to the outcomes reported, ranibizumab afforded more reduction in CRT at 6 months than dexamethasone, and bevacizumab afforded more reduction than triamcinolone. As for intravitreal anti-VEGF injections, the resolution of exudative fluid and retinal oedema is important for the favourable treatment of BCVA.87
A low incidence of AEs should also be considered besides the better efficacy of different drug treatments. In this network meta-analysis, increased IOP, cataracts, VH and retinal tear are the four most frequently reported AEs from the included studies. More reported data can lead to more accurate analyses. As shown in table 11, dexamethasone has a higher risk of increased IOP compared with that of aflibercept and ranibizumab. In contrast, ranibizumab was associated with a higher probability of cataracts than dexamethasone. Cataracts are associated with injection frequency, and dexamethasone needs fewer injections than anti-VEGF agents. Gu et al reported that the advantages of dexamethasone are fewer number of injections and long-term efficacy, while the advantages of ranibizumab include lower incidence of increased IOP,88 which is similar to the results of our pooled data. A head-to-head trial called comparison of ranibizumab PRN versus single-dose dexamethasone for branch retinal vein occlusion (COMRADE-B) demonstrated that elevated IOP occurred more frequently with dexamethasone than with ranibizumab treatment, similar to Branch Retinal Vein Occlusion (BRVO).89 In addition, aflibercept showed lower incidence of VH and ranibizumab showed lower incidence of retinal tear. AEs mainly arise from the disease process itself or as a result of the side effects during the course of treatment. Intravitreal anti-VEGF or corticosteroid injections and traumatic procedures sometimes cause AEs such as endophthalmitis. Safety is as important as efficacy after treatment, and both must be considered comprehensively in the selection of drugs for CRVO.
When comparing ranibizumab, dexamethasone and sham/placebo, as well as bevacizumab, triamcinolone and sham/placebo, node-splitting and pairwise meta-analysis could be used to estimate the efficacy based on direct versus indirect evidence. If direct and indirect evidence existed together, the consistencies could be tested. Since no inconsistencies were observed in this network meta-analysis, we performed sensitivity analysis of the comparison of random and fixed effects models, which was more accurate.34 The unchanged outcome suggests that our model was robust according to known data, and therefore, the results of this network meta-analysis would be useful in clinical practice.
As mentioned above, both dexamethasone and ranibizumab have their own advantages and disadvantages.88 Broadly speaking, each drug has benefits and risks; therefore, estimating benefits and risks consistently is necessary. Although anti-VEGF agents can avoid the increased IOP caused by dexamethasone, the high risk of developing cataracts after anti-VEGF treatment, especially ranibizumab, cannot be ignored.
Aflibercept and ranibizumab are the two, on-label maximum dosage drugs recently approved in Europe and America. According to the data of benefit–risk analysis between the two drugs from the included studies, aflibercept had a slight advantage over ranibizumab. However, this does not mean that aflibercept is effective for all patients. Patients need to choose medications according to their actual situation. During our clinical practice, some patients were not responsive to anti-VEGF agents, but instead responded to dexamethasone.
Considering that intravitreal anti-VEGF agents are expensive, intravitreal corticosteroids should be considered to reduce the overall treatment cost. However, care should be taken when using these treatments because elevated IOP is seen more frequently with corticosteroid therapy than with anti-VEGF therapy, as demonstrated by our network meta-analysis. Regardless of the treatment administered, all patients with CRVO should be closely monitored for IOP changes and VA.
This is the second network meta-analysis providing an indirect comparison of drugs to treat ME secondary to CRVO, and our study possesses several strengths when compared with previous systematic reviews.24 First, our meta-analysis included the most recent reports, analysing studies published as late as 1 May 2017. Second, we performed a comprehensive comparison of aflibercept, ranibizumab, bevacizumab, pegaptanib, dexamethasone and triamcinolone treatment using strict inclusion and exclusion criteria. Third, the 12-month follow-up time point was also considered in addition to 6 months, because the outcome at 12 months could better show the duration of efficacy after treatment.
Although the results of this work may be important for clinical treatment, there are certain limitations that need to be considered. First, our data contained some biases, which may have influenced our results. Second, more detailed data at long-term follow-up time points (eg, 24 months) are required to improve the accuracy and robustness of our findings for clinical applications. Third, the details of AEs were not always reported in each study, and the data available can only indicate the relative safety of every intervention for CRVO. To assess the efficacy of these treatments more accurately, additional high-quality RCTs with comprehensive safety data will be necessary.
Head-to-head trials comparing ranibizumab, aflibercept, bevacizumab, pegaptanib, dexamethasone and triamcinolone are needed. Further long-term, prospective studies are needed to examine and compare the safety and efficacy of CRVO-associated ME treatment strategies. Including data from future studies in subsequent meta-analyses will improve conclusion accuracy and robustness and provide better clinical guidance. In addition, as patients can be concerned about the cost of treatment, clinicians may prefer aflibercept because it requires fewer injections.24
Conclusion
Our analysis confirms that anti-VEGF agents have more advantages than corticosteroids in the treatment of ME secondary to CRVO. A higher proportion of the patients who received intravitreal anti-VEGF injections gained ≥15 letters than those treated with corticosteroids at both 6 and 12 months. Among these anti-VEGF agents, aflibercept and ranibizumab were the best drugs for BCVA improvement and CRT reduction. In terms of AE, the results of network meta-analysis showed that (1) dexamethasone was associated with a higher risk of increased IOP than aflibercept and ranibizumab, (2) ranibizumab had a higher probability of cataract formation than dexamethasone, (3) aflibercept exhibited superiority in terms of low incidence of VH and (4) ranibizumab exhibited superiority in terms of low incidence of retinal tear. Aflibercept was shown to have a slight advantage over ranibizumab by benefit–risk analysis, but with no statistical difference. More high-quality RCTs will be necessary as the results of this study provide only a reference for clinicians. Each patient must be evaluated individually for the appropriate treatment regimen.
Acknowledgments
The authors thank the researchers whose studies were included in this network meta-analysis and provided useful data to us.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
Footnotes
Contributors TQ: study conception, study design, data collection, data analysis, manuscript writing and final manuscript approval; MZ: study design, data collection and critical manuscript revision; YW: statistical analysis; MXL: statistical analysis; XX: study conception, study design, critical manuscript revision and final manuscript approval.
Funding This study was funded by the National Natural Science Foundation of China (Grant No. 81800878) and Interdisciplinary Program of Shanghai Jiao Tong University (Grant No.YG2017QN24).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Extra data can be accessed via the Dryad data repository at http://datadryad.org/withthedoi:10.5061/dryad.p1qq2r1.