Article Text

Abstract
Objective To model the long-term cost-effectiveness of consuming milk powder fortified with potassium to decrease systolic blood pressure (SBP) and prevent cardiovascular events.
Design A best case scenario analysis using a Markov model was conducted.
Participants 8.67% of 50–79 year olds who regularly consume milk in China, including individuals with and without a prior diagnosis of hypertension.
Intervention The model simulated the potential impact of a daily intake of two servings of milk powder fortified with potassium (+700 mg/day) vs the consumption of a milk powder without potassium fortification, assuming a market price equal to 0.99 international dollars (intl$; the consumption of a milk powder without potassium fortification, assuming a market price equal to intl$0.99 for the latter and to intl$1.12 for the first (+13.13%). Both deterministic and probabilistic sensitivity analyses were conducted to test the robustness of the results.
Main outcome measures Estimates of the incidence of cardiovascular events and subsequent mortality in China were derived from the literature as well as the effect of increasing potassium intake on blood pressure. The incremental cost-effectiveness ratio (ICER) was used to determine the cost-effectiveness of a milk powder fortified with potassium taking into consideration the direct medical costs associated with the cardiovascular events, loss of working days and health utilities impact.
Results With an ICER equal to int$4711.56 per QALY (quality-adjusted life year) in the best case scenario and assuming 100% compliance, the daily consumption of a milk powder fortified with potassium shown to be a cost-effective approach to decrease SBP and reduce cardiovascular events in China. Healthcare savings due to prevention would amount to intl$8.41 billion. Sensitivity analyses showed the robustness of the results.
Conclusion Together with other preventive interventions, the consumption of a milk powder fortified with potassium could represent a cost-effective strategy to attenuate the rapid rise in cardiovascular burden among the 50–79 year olds who regularly consume milk in China.
- cost-effectiveness
- potassium
- fortification
- cardiovascular
- china
- markov model
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to evaluate the cost-effectiveness of a food fortified with potassium to prevent cardiovascular diseases in China.
A conservative approach was adopted, including only stroke and myocardial infarction among the possible cardiovascular events.
This analysis was based on data reported in the literature rather than data from real cases.
In order to extend our results to a national level, we assumed that the incidence and costs related to cardiovascular events were the same across China.
Introduction
Cardiovascular diseases (CVD) are the leading cause of premature death and disability worldwide: more people die annually from CVD than from any other cause.1 2
China is not unique in that respect and has a very high burden from CVD.3 4 Among the individual modifiable risk factors, the most important in China is high blood pressure.5 Hypertension is a serious health issue which has significantly increased over the past few decades. In 2010, the prevalence of hypertension was estimated at 34% of the adult population (35% in men and 32% in women)4 with no signs of decline.6 The excessive dietary salt consumption (eg, in rural China, salt intake can be as high as 12–15 g/day)7 is one of the major causes of hypertension and could partly explain why, among other reasons (eg, obesity, smoking and air pollution), the Chinese population has a higher overall stroke incidence compared with Caucasians.8–10 In China, 20%–41% of deaths are due to cardiovascular episodes2 11 and this percentage is likely to increase resulting in 21.3 million additional cardiovascular events and 7.7 million deaths from 2010 to 2030, based on population ageing and growth alone.12 13
The financial burden from CVD is substantial to both patients and the healthcare system. In 2011 alone, almost 13 million patients in China were hospitalised for CVD, with total hospitalisation expenditures equalling ¥40 billion (international dollar (intl$) 11.36 billion at a conversion rate of intl$1.00=3.52 ¥),14 which corresponded to 1.64% of the national health expenditures.11 The total amount of the annual direct costs are estimated to be more than US$40 billion, the equivalent of 4% of China’s gross national income, with indirect costs more than doubling the direct costs.15
In order to decrease systolic blood pressure (SBP), the WHO guidelines recommend to decrease sodium intake to less than 2000 mg/day and increase potassium intake to at least 90 mmol or 3510 mg/day.16 Many studies have shown that reducing sodium intake in China would be an effective strategy,17 and recent studies have shown that increased potassium intake can benefit endothelial function,18 which is correlated with future cardiovascular events.19
This study aims to specifically evaluate the cost-effectiveness of increasing potassium intake (+700 mg/day) to lower SBP, and, consequently, the risk of CVD among the 50–79 year olds who regularly consume milk in China via the consumption of a milk powder product fortified with potassium.
Methods
The cost-effectiveness of a milk powder product fortified with potassium was estimated using TreeAge Pro 2015. We hypothesised that an additional potassium intake of 700 mg/day would reduce the burden of disease related to CVD events due to the lowering effect of potassium intake on SBP.
Baseline potassium intake
Data from the 2009 China Health and Nutrition Survey (CHNS)20 were used to assess the baseline distribution of potassium intake among adults in nine provinces. Since individual-level data are distributed free of charge via the web, no agreement was required. Crème Nutrition,21 a scientific, cloud-based software service designed to analyse dietary intakes of foods and nutrients, was used to estimate the baseline potassium dietary intake. In their unpublished report, final outcome of a consultancy for Nestlé, the baseline potassium intake of the Chinese population aged over 45 years was 1781 (±9.95) mg/day (figure 1). No permission to publish was needed.

Baseline daily potassium intakes (mg/day) from the total diet in the Chinese population aged over 45 years. Mean is the average of intake values for all individuals within the target population; P25, P50, P75 and P95 are percentiles and represent the values of intake below which the 25%, 50%, 75% and 95% of the analysed population, respectively, falls. WHO guidelines recommend a potassium intake to at least 90 mmol or 3510 mg/day for adults. Source: Creme Global.
Potassium effect on the SBP
We relied on the literature to estimate the effect of increasing potassium intake on SBP. Potassium supplementation is associated with a reduction of blood pressure and the effect size may vary depending on different factors.22–26 For our model, we relied on one human intervention study conducted in China on a heterogeneous population (normotensive, prehypertensive and hypertensive), where the subjects were given 60 mmol/day via potassium chloride tablets.27Compliance among subjects, measured using 24 hours urine samples and assuming 80% recovery, indicated a dietary intake of about 26 mmol/day, corresponding to about 1 g of potassium. The reduction of SBP after 6 and 12 weeks was −6.38 and −3.68 mmHg, respectively. To be conservative, we used the value of SBP reduction at the end of the intervention (−3.68 mmHg) to represent the average decrease in SBP for individuals in China. To account for the different potassium amounts (1 g in the Gu study vs 700 mg in our model), and the non-linear relationship between potassium intake and blood pressure,23 we evaluated the impact at different levels (% effectiveness) by downgrading 3.68 mmHg to 2.76 mmHg (75%), 1.84 mmHg (50%) and 0.92 mmHg (25%).
Markov model
Finally, we built a Markov model (figure 2), based on the structure of Li et al,28 in TreeAge Pro 2015 to compare the long-term cost-effectiveness, from a societal perspective, of an additional potassium intake (+700 mg/day), given through a milk powder product, against consumption of the same product without potassium fortification. The cost of the potassium fortification in the milk powder was modelled as a 13.13% increase (intl$0.99 vs intl$1.12). Both arms (milk powder with potassium fortification and milk powder without fortification) have the same structure, but different probabilities of CVD events.

Decision tree representation of the Markov model structure for each arm.63 Circles indicate chance events and triangles indicate terminal nodes. The ‘well” and ‘chronic CVD’ state represent people without or with prior AMI or stroke, respectively. For the initial population, we assigned 3.83% to start in ‘chronic CVD’ state, consistent with the prevalence of CVD in China among 50–79 years old. The remaining 96.17% start from the ‘well’ state. People in the ‘well’ state can remain in their state or passing to ‘chronic CVD’ in case of first AMI or stroke. In each cycle, people in Well and the chronic CVD states may experience a MI or stroke and have the same chances to survive as the other people in their state, regardless of their personal story. ‘Other death’ accounts for all people who die for causes different from CVD. AMI, acute myocardial infarction; CVD, cardiovascular disease; MI, myocardial infarction.
In order to populate the model, we relied on several data sources including published literature, expert opinion, national statistics and tariff lists. The stroke and MI incidence and mortality for the milk powder without potassium fortification arm (control group), and the risk reduction applied to estimate the probabilities for the other arm (intervention group) are reported in table 1. Given the linear relationship between SBP and CVD risk reduction, we extrapolated the impact of a 3.68 mmHg reduction in SBP on CVD risk by dividing the referenced impact of a 10 mmHg reduction by 2.71.29–32
Stroke and MI incidence, mortality and risk reduction
Costs and utilities associated with a cardiovascular event are reported in table 2. The cost of inpatient care due to a stroke was calculated as a weighted average of 25% cerebral haemorrhage and 75% cerebral infarction. The early outpatient drug cost for treating hypertension was obtained from a Chinese publication, where only two geographical areas (Beijing City and Jiangsu Province) were surveyed.33 In order to calculate a national cost, we first calculated the average of these two provinces. Given that the outpatient drug costs were collected only in Tier 1 hospitals, we then calculated the costs in the Tier 2 and Tier 3 hospitals (which are more expensive). We obtained the total number of outpatient visits for Tier 1, Tier 2 and Tier 3 hospitals in China and average outpatient drug costs (ie, general costs, not only for hypertensive) at each tier from the China Health and Family Planning Statistical Yearbook 2015.34 We used these data to estimate the amounts Tier 1 and Tier 2 hospitals spend as compared with Tier 1. In this way, we obtained the average outpatient drug cost per capita for hypertensive patients in all Tier hospitals in 2014. When necessary, the appropriate inflation rate was applied to convert the costs from previous years to 2014 prices. In order to estimate the societal loss due to CVD among the population of 50–79 year olds, we multiplied the average daily salary for the number of days of work lost after a stroke or a MI. This was valid even for retired people, on the assumption that their time still has a value (eg, they may be involved in socially useful activities such as looking after grandchildren). All costs are expressed in international dollars.14
Costs and utilities
Utilities were obtained from the literature and were expressed in quality-adjusted life years (QALY). The utilities for MI and stroke referred to acute states (moment of the event).
Taking into account the minimum age of the population of interest (50 years old) and the average life expectancy in the Chinese population (76 years),35 we considered a time horizon of 30 years. A discount rate of 3% per annum was applied for both costs and utilities.36 37 The findings were presented as incremental cost-effectiveness ratio (ICER), which measures the incremental cost per QALY. We performed both deterministic and probabilistic sensitivity analyses to assess the impact of the uncertainty of the key variables in the model on the base case estimates. This study did not involve human subjects and thereby was exempt from institutional review board approval.
Results
Cost-Effectiveness
With an ICER equal to intl$4711.56 per QALY gained, the intervention can be classified as very cost-effective according to the conventional WHO threshold which accounts for a country’s annual gross domestic product (GDP) per capita (very cost-effective if <1 GDP per capita; cost-effective if equal to 1–3 GDP per capita; no cost-effective is >3 GDP per capita).38 Moreover, we evaluated the impact on the base case estimates of an increase in potassium intake (+700 mg/day) at different level of effectiveness (75%, 50% and 25%) on SBP. The consumption of milk powder fortified with potassium was the preferred strategy compared with the milk powder without fortification, ceteris paribus, up to an effectiveness of potassium on SBP equal to the 50% (table 3).
Base case results
Sensitivity analyses
We performed both deterministic and probabilistic sensitivity analysis evaluating the impact on the base case estimates of an increase in potassium intake (+700 mg/day) at different level of effectiveness (75%, 50% and 25%) on SBP.
In the deterministic sensitivity analysis (Tornado diagrams, figure 3), we applied±20% variations to all costs and the appropriate ranges (table 2) to the inpatient days of MI and stroke. Hospitalisation after a stroke had the largest impact whereas a hypertension visit had the least impact on final costs.

Deterministic sensitivity analysis—Tornado diagrams. The bars represent the relative importance of the variables on the expected value (EV), the incremental cost-effectiveness ratio: the larger the bar, the higher the impact of that cost voice. In this case the cost of the hypertensive drugs is the one affecting the final cost the most, the hypertension visit the less. CVD, cardiovascular disease; MI, myocardial infarction.
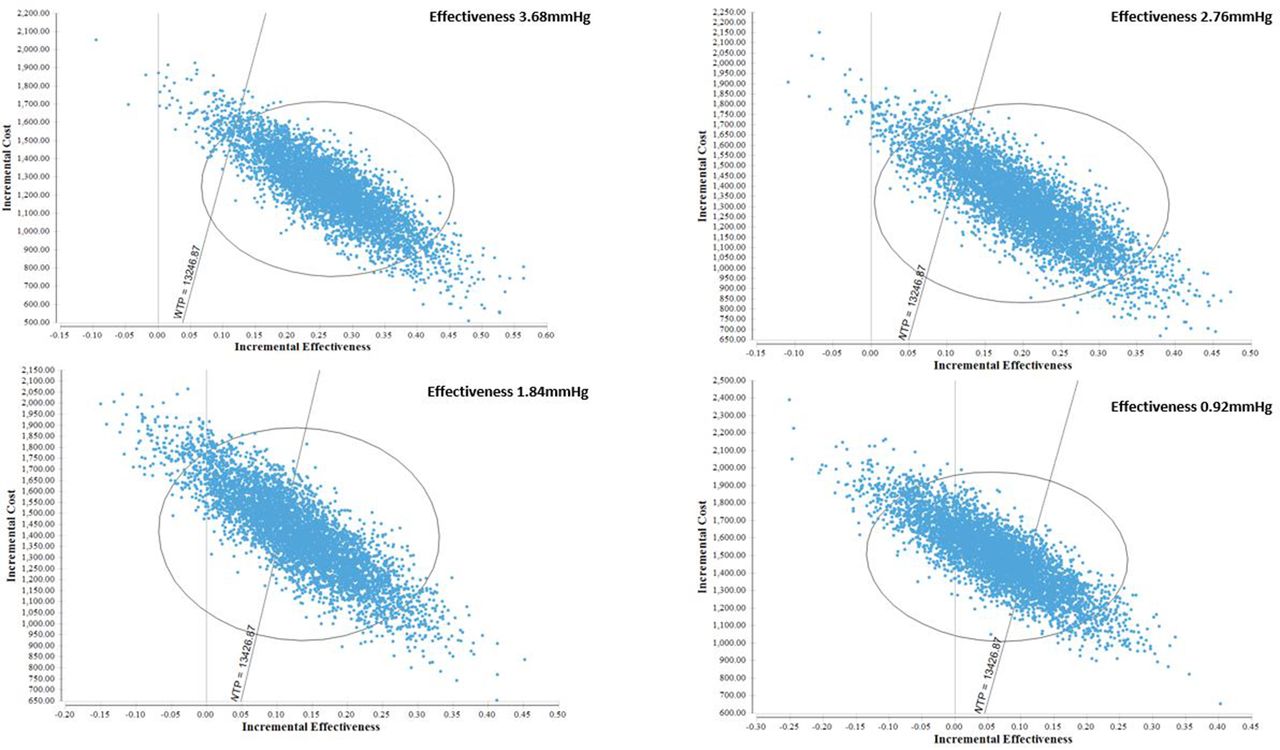
In the probabilistic sensitivity analysis (Monte Carlo simulations, figure 4), all costs and resources used were modelled using a gamma distribution, while probabilities and utilities using a beta distribution.39 The consumption of milk powder fortified with potassium was the preferred strategy compared with the milk powder without fortification, ceteris paribus, up to an effectiveness of potassium on SBP equal to −1.83 mmHg (49.72%). The results were overall robust.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Probabilistic sensitivity analysis—Monte Carlo simulations. The x and y axes, respectively, represent the incremental effectiveness and cost. The dots represent the incremental cost-effectiveness ratio values outcome of 5000 simulations carried out to take into consideration the uncertainty around both cost and effectiveness. The ellipse represents 95% of all data points. The line from the origin is the willingness to pay (WTP), corresponding to the gross domestic product per capita. Points below right of the WTP line recommend the fortified milk powder as preferred strategy and are 96.32% for 3.68 mmHg (100% effectiveness), 86.24% for 2.76 mmHg (75% effectiveness), 61.34% for 1.84 mmHg (50% effectiveness) and 30.72% for 0.92 mmHg (25% effectiveness).
Discussion
Principal findings
To the best of our knowledge, this study is the first to show the cost-effectiveness of increasing potassium intake, via a milk powder product fortified with potassium (+700 mg/day), to reduce blood pressure and prevent cardiovascular diseases in China. This model capitalises on the substantial evidence already existing on the association between increased potassium intake and the reduction of blood pressure.23 40 The daily potassium intake we used as baseline, 1.785 g/day, is consistent with the values reported in the literature: 1.7 g/day and 1.8 g/day.41 42 It is worth to mention that, in their subgroup analyses, Aburto et al showed that, regardless of baseline potassium intake, there is a comparable reduction in blood pressure when potassium intake is increased.23
We estimated that an increase in potassium intake (+700 mg/day), would result in an average reduction in SBP of 3.68 mmHg in the Chinese adult population. This value was based on an intervention study conducted in Chinese adults (mean age: 56.9±7.4 in the intervention group)27 with an overall low risk of bias,43 which has been included in several recent systematic reviews and meta-analyses.23 40 The baseline SBP was 130–159 mmHg, which is consistent with other reported figures from the literature for a similar age range.44 In that specific study, the difference in 24 hours urinary excretion of potassium between intervention and control group was 20.6 mmol, hence corresponding to an estimated intake of 1.0 g of potassium (close to our own case), assuming a recovery of 80% of dietary potassium in the urine. This value is in agreement with the reduction in SBP reported in the Aburto meta-analysis of 3.49 mmHg (95% CI: 1.82 to 5.15) on average for the overall population.23 Moreover, when the difference in achieved potassium intake between the intervention and the control group was less than 30 mmol/day (1.17 g/day), a reduction of 4.89 mmHg in SBP (95% CI: 2.20 to 7.59) was observed.23 It is well acknowledged that BP status at baseline as well as age influence the reduction in the blood pressure triggered by potassium intake, with much larger effects observed in hypertensive compared with non-hypertensive individuals,23 and in older compared with younger individuals.26 Also, blood pressure may be significantly lowered in normotensive subjects with a low dietary intake of potassium,45 or with sodium sensitivity, an independent risk factor for cardiovascular disease.46 We are therefore confident that both normotensive and hypertensive would equally benefit from a potassium supplementation.
Unfortunately, no other study has been conducted with such a small amount of potassium like ours (+700 g/day), therefore we could not model the provincial level variation impact. Acknowledging these limitations, we took uncertainty into consideration through an extended sensitivity analysis, to model which would be the effect at different level of effectiveness on SBP (100%, 75%, 50%, 25% and 10%).
Strengths and weaknesses of the study
The main strength of this study was the conservative approach adopted. The cost-effectiveness model only included stroke and MI among the possible cardiovascular events, focused only on medical costs and partially on indirect costs (days of work lost), and did not include other cost types such as travelling costs, mortality costs or intangible costs. An additional strength was the extensive sensitivity analysis conducted on the effectiveness of a potassium supplementation to decrease SBP which evaluated several scenarios given that limited clinical evidence is available in this population. To the best of our knowledge, interventions have not been conducted using relatively small amounts (700 mg/day) of potassium, but given that potassium fortification may also make foods bitter, this is the maximum amount consumers showed to tolerate during consumers tastes. An additional amount would mean to risk to have a negative impact on the compliance and, as a consequence, on the effectiveness, of such an intervention.
The first limitation of this study was the use of multiple sources of data for the model parameter values.
Unfortunately, no data exist about CVD risk or burden of the Chinese 50–79 year olds who regularly drink milk compared with those who do not. Moreover, given the lack of detailed information about some provinces and ethnic groups, we assumed that incidences, costs and baseline BP and potassium intakes were the same across China in order to extend our results to a national level. For the same reason, we assumed people who never had a CVD event to be fully healthy and do not face any cost to treat hypertension. Finally, we did not consider the current sodium intake nor any effect of fortified milk consumption on sodium consumption. The sodium to potassium ratio regulates blood pressure and Chinese population consume excessive amounts of sodium and not enough potassium. Therefore, increasing potassium intake would be indeed more effective in preventing cardiovascular diseases if combined with a reduction in the salt consumption.
Comparison with other studies
Multiple cardiovascular risk factors are common among the Chinese population, including smoking or overweight, and often both are present in the same individual.3 47 A large body of literature exists on interventions aiming to reduce blood pressure,48 49 the most important individual risk factor for CVD, with some studies assessing the effectiveness and cost-effectiveness of the interventions.50 51 One study from He et al, targeted to families of the Chinese schoolchildren in the Changzhi urban area, evaluated an education programme to lower-salt intake,17 while a study from Wang et al simulated which would be the effect of promoting the replacement of the cooking salt with a substitute, currently available, containing 25% potassium and 10% magnesium in the Chinese diet.44 Both studies analyse the impact of a culturally tailored intervention: differently from North American and European population, who take the most of their salt intake from packaged processed food, Chinese population primary salt intake is food consumed at home, therefore home-cooked foods is what public policies should target.44 Another study from Gu et al simulated the effect of a hypertension treatment of essential medicines in Chinese adults and evaluated different healthcare scenarios.36 Similar to the He et al study,17 the present analysis evaluated the effectiveness of a SBP reduction through food, and similar to Gu and Wang study,36 44 it was based on a simulation model and not a real intervention. Simulations allow generalising the results to the whole country, but are less precise than a real intervention. All studies, however, had a positive outcome and showed the effectiveness and/or cost-effectiveness of the interventions. Together with our findings, these results suggest that in China different interventions (less sodium, more potassium and appropriate medicines) could be implemented to decrease blood pressure and lower the risk of CVD.
While consistent evidence exists in China, studies evaluating the effect of fortifying food to decrease the risk of CVD have had mixed findings in Europe. In a study from Germany, an enriched margarine with plant sterols has been shown to be a cost-effective method to decrease the risk of coronary heart disease (CHD) in a representative sample of the 30–79 year olds population; assuming a health insurer’s perspective and calculating the transition probabilities for CHD and CHD-related death on the basis of the Framingham risk equations.52 In a study from the Netherlands, they evaluated the cost-effectiveness of functional foods containing phytosterols/phytostanols, in addition to statins, to prevent cardiovascular diseases among the population of 35–75 year old eligible for use according to their 10-year absolute risk of fatal cardiovascular disease (SCORE risk).53 The results, differently from the German study,52 showed that this strategy was not- cost-effective.
A lack of consistency in the findings between China and Europe could be due to differences in the type of intervention (margarine and functional food containing phytosterols/phytostanols vs potassium/sodium), the health outcomes (cholesterol vs SBP), the healthcare systems and the health status of the populations.
Public health implications
In China, and like many other developing countries, the rapid rise of non-communicable diseases imposes major challenges to the healthcare system and targeting high blood pressure is a public policy priority.54 Adults in China consume excessive amounts of sodium and not enough potassium. Both are key minerals involved in the regulation of blood pressure; therefore, increasing potassium intake, in combination with other public health interventions, may help in decreasing blood pressure and preventing cardiovascular diseases.23 42
According to our findings, the consumption of milk powder fortified with potassium was cost-effective, if compared with the milk powder without fortification, for the 8.67% of 50–79 year olds who regularly consume milk,20 21 and could have a beneficial impact without increasing the total caloric intake. Healthcare savings due to CVD prevention would amount to intl$267.54 per consumer. Given a total population of 362.74 million in that age range,55 the consumption of milk powder fortified with potassium could allow medical cost savings equal to intl$8.41 billion. In addition, out-of-pocket expenditures are well known to be a substantial portion of the healthcare costs and a large portion of the population in China is not covered by insurance. In 2003, approximately 56% of CVD patients did not have health insurance and on average, 76% of outpatient costs per visit and 65% of inpatient costs were paid out-of-pocket.56 Indeed, individuals experiencing severe CVD are likely to face catastrophic health spending (CHS), defined as health expenditures higher than 30%–40% of the total household budget.57 58 In a 2009 survey involving 62 hospitals in China, more than the 71% of poststroke patients reported CHS, which results in impoverishment for individuals and their families.59 Recent healthcare reforms are aimed towards improving this situation and reducing inequalities, but further strategies are still needed for patients with cardiovascular disease; especially for those living in rural areas or belonging to lower income groups.60–62
Unanswered questions and future research
Further research is needed to assess the cost-effectiveness of reducing CVD risk with other types of foods and new clinical trials are encouraged to evaluate the effectiveness of small increases in potassium intake on the SBP.
Conclusion
Together with other preventive interventions, the consumption of a milk powder fortified with potassium could represent a cost-effective strategy to attenuate the rapid rise in cardiovascular burden among the 50–79 year olds in China. This strategy could be especially easy to implement in those already having regular dairy consumption, and even encouraged in those with low dairy product intake.
Acknowledgments
We thank Dr Dantong Wang (Nestlé Research Center, Lausanne, Switzerland) for the help provided in translating and interpreting some of the Chinese literature analysed and Dr Kevin Mathias (Nestlé Research Center, Lausanne, Switzerland) for the language revision of the final manuscript. Finally, since this research used data from CHNS, we thank the National Institute for Nutrition and Health, China Center for Disease Control and Prevention, Carolina Population Center (P2C HD050924 and T32 HD007168), the University of North Carolina at Chapel Hill, the National Institutes of Health (NIH) (R01-HD30880, DK056350, R24 HD050924 and R01-HD38700) and the NIH Fogarty International Center (D43 TW009077, D43 TW007709) for financial support for the CHNS data collection and analysis files from 1989 to 2015 and future surveys, and the China–Japan Friendship Hospital, Ministry of Health for support for CHNS 2009, Chinese National Human Genome Center at Shanghai since 2009 and Beijing Municipal Center for Disease Prevention and Control since 2011.
Acknowledgments
None
References
Footnotes
Contributors PD conceived the study. LD built the model and drafted the paper. HF and TX updated the economic model with demographic, cost and utilities and helped in running the model; YW and ML contributed with epidemiological data and estimates; both HF and YW oversaw and supervised the empirical work. DZ supervised and contributed to everything (data, effectiveness, writing) related to the potassium effectiveness on systolic blood pressure and consequent risk reduction. All authors contributed with their comments to the manuscript and revised the final version of the paper.
Funding This work was funded by the Nestlé Research Center of Beijing (China) and the Nestlé Research Center of Lausanne (Switzerland).
Competing interests HF and YW were paid as consultants by Nestlé.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Requests for access to data should be made to the corresponding author at patrick.detzel@rdls.nestle.com.