Article Text

Abstract
Objectives We systematically reviewed the literature to identify evidence-informed recommendations regarding the detection of drug-induced pancreatitis (DIP) and, secondarily, to describe clinical processes for the diagnosis of DIP.
Design Systematic review.
Data sources Ovid MEDLINE, including Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Embase Classic+Embase, the Cochrane Library.
Eligibility criteria We included clinical practice guidelines, systematic reviews, narrative reviews and observational studies with a focus of establishing incidence, prevalence or diagnostic approaches for DIP. Clinical trials that diagnosed DIP as an outcome were also included.
Data extraction and synthesis Two reviewers screened citations and performed data extraction. A narrative synthesis of the evidence was prepared.
Results Fifty-nine studies were included. Early published evidence suggested serial pancreatic ultrasound could detect subclinical pancreatitis; however, subsequent studies demonstrated no utility of serial ultrasound or serial monitoring of pancreatic enzymes in the early detection of DIP. Two small studies conducted in patients with a high baseline risk of acute pancreatitis concluded serial monitoring of pancreatic enzymes may be useful to guide early discontinuation of medications with known associations with pancreatitis. Early discontinuation of medication was not advised for lower-risk patients because some medications cause transient elevations of pancreatic enzymes that do not progress to acute pancreatitis. Eight of 52 studies (15%) reporting a clinical diagnostic process for DIP reported using currently accepted criteria for the diagnosis of acute pancreatitis. A variety of methods were used to assess drug-related causality.
Conclusions There is minimal evidence to support the use of serial monitoring by ultrasound or pancreatic enzymes to detect cases of DIP. Serial monitoring may be useful to guide early discontinuation of DIP-associated drugs in high-risk patients, but not in lower-risk patients. Greater uptake of standardised diagnostic and causality criteria for DIP is needed.
Trial registration number CRD42017060473
- pancreatitis
- drug reaction
- detection
- diagnosis
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We present the findings of a review of a previously unreviewed research question.
Our review followed robust and established systematic review methods, including development and registration of an a priori protocol.
Our search strategies were broad and encompassed all of the key databases in this area.
Primary studies that may have used a drug-induced pancreatitis (DIP) diagnostic process but that were not indexed in databases using vocabulary related to DIP would not have been captured by our search.
We attempted to limit confirmation bias through inclusion of the entire review team and clinical experts in data synthesis, as well as transparent reporting of quotes from references.
Introduction
Acute pancreatitis (AP) is the most common single gastrointestinal cause of hospitalisation in the USA,1 with an annual incidence of emergency department or ambulatory care visits ranging from 106 to 320 per 100 000 population,2 3 at an inpatient cost of approximately 2.6 billion US$ annually.1 With an associated overall mortality ranging from 1% to 30%,2 4 5 AP can result in considerable patient harm. Most cases are attributed to obstructive gallstones or alcohol use6 however, approximately 0.1% to 2.0% of AP cases have a medication-related cause,6 with over a hundred medications associated with AP in the literature.7
The list of medications potentially associated with AP will continue to expand as new drugs are marketed. Given its rare occurrence, AP risk is difficult to assess in clinical trials unless very large sample sizes are enrolled. To reduce the risk of approval of drugs that ultimately demonstrate an association with AP postmarket, a greater understanding is needed of methods to detect drug-induced pancreatitis (DIP) in clinical trials conducted as part of the premarket regulatory process. The diagnosis of DIP first requires a confirmed diagnosis of AP and, second, establishment of a drug-related cause through causality assessment. Detection of DIP differs from diagnosis in that it incorporates serial monitoring of all patients receiving a drug of interest to identify all cases of AP. There is uncertainty regarding the optimal means by which drug trialists and manufacturers should be required to detect DIP. The objective of this review was to systematically review clinical practice guidelines, reviews and observational studies to identify evidence-informed recommendations regarding the detection of DIP. Secondarily, we identified processes to diagnose DIP.
Methods
Established systematic review methods were used, and a review protocol was developed a priori and registered with PROSPERO (online supplementary appendix 1). The reported work was part of a series of systematic reviews on DIP.
Supplemental material
Research question
We addressed the following research question: ‘What are the current evidence-informed recommendations regarding detection of drug-induced pancreatitis?’ A secondary review objective was to describe processes of diagnosis of DIP reported in the literature.
Study eligibility criteria
Eligible studies were identified using a priori selection criteria, established according to the population-intervention-comparator-outcomes-study design framework:
Population: Human subjects only, with no restrictions on patient age or other demographics.
Intervention and comparator: No restrictions.
Outcomes: Primary studies that identified the diagnosis of DIP a priori as a primary or secondary outcome were included. Those in which AP occurred only as an unanticipated/unmonitored adverse event were excluded.
Study design: Clinical practice guidelines, systematic reviews and observational studies (both prospective and retrospective cohort studies and case series that diagnosed DIP either as part of inclusion criteria or as a primary or secondary outcome) with a focus of establishing incidence, prevalence or diagnostic approaches for DIP were included. Given the low yield of these designs of interest following initial screening, we amended the protocol to include narrative reviews and clinical trials that diagnosed DIP as a primary or secondary outcome. Studies of all designs were only included if a sufficient description of a clinical process to detect or diagnose DIP was reported, including patient history, signs and symptoms and laboratory and/or imaging criteria, plus methods to determine drug causality.
Searching the literature
An experienced information specialist (BS) developed and tested the search strategy using an iterative process in consultation with the review team. A second information specialist peer reviewed the strategy prior to execution using the Peer Review of Electronic Search Strategies checklist.8 Using the Ovid platform, we searched Ovid MEDLINE, including Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Embase Classic+Embase. We also searched the Cochrane Library on Wiley. We performed separate searches for primary studies and systematic reviews. We incorporated controlled vocabulary (eg, ‘Pancreatitis/ci (chemically induced),’ ‘Drug-Related Side Effects and Adverse Reactions,’ ‘Diagnostic Techniques, Digestive System’) and keywords (eg, ‘drug-induced pancreatitis,’ ‘adverse effect,’ ‘detection’) into the searches. We adjusted vocabulary and syntax across the databases. No date or language limits were applied, but we removed animal-only and opinion pieces, where possible. Specific details regarding the strategies appear in online supplementary appendix 2.
All database searches were performed on 31 January 2017 from inception. A grey literature search of clinical practice guideline registries, the TRIP (Turning Research Into Practice) database and Google Scholar was undertaken on 9 March 2017 to 10 March 2017. We also manually searched the references of the final included studies for additional potentially relevant titles.
Study selection
Titles and abstracts were screened for relevance independently by two reviewers, with agreement of two reviewers required for exclusion, and inclusion requiring assessment by only one reviewer. Potentially relevant full texts were screened by two reviewers, with agreement of both reviewers required for both inclusion and exclusion. Screening was conducted in the online platform DistillerSR (Evidence Partners Inc, Ottawa, Canada). Screening forms were piloted to ensure similar understanding of the eligibility criteria among reviewers. Conflicts were resolved by consensus or consultation with a third independent reviewer. Study selection was summarised using a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.9
Data extraction and risk of bias assessment
Two independent reviewers extracted data, with a third reviewer to establish consensus as needed. A data collection form was developed in Microsoft Excel and piloted on a small number of studies. The pilot data were discussed among the review team to refine the form. The following data were extracted: publication characteristics (year of publication, journal, authorship, country); study design (eg, clinical practice guideline, systematic review, narrative review or primary study); details of the reported approach to detect or diagnose DIP, including patient history, symptoms, use of laboratory testing, use of imaging, causality assessment and other factors (including patient characteristics and drug implicated, if relevant) and literature cited for the detection method or diagnostic process (if reported). Given that the objective of this review focused on study methods/recommendations and not findings, risk of bias assessment was not conducted.
Summarising the evidence
Publication characteristics and study design were synthesised descriptively. Studies were classified according to whether they reported a process to detect or diagnose DIP. We prepared a narrative summary of the recommendations for and against serial monitoring for DIP detection and described detection methods used in the literature, summarised by decade of publication.
A separate narrative synthesis of DIP diagnostic processes was conducted, focusing on (1) adherence to the currently accepted AP diagnostic criteria published following international consensus as part of the Atlanta classification of AP10 and (2) the reported methods to assess causality. By international consensus, AP diagnosis requires two of the following three features to be present10 : (i) typical clinical symptoms (eg, epigastric pain, nausea, vomiting); (ii) serum amylase or lipase elevated at least three times the upper limit of normal (ULN); (iii) characteristic imaging findings of AP on contrast-enhanced computed tomography or, less commonly, on MRI or transabdominal ultrasonography.
Reporting of review findings
Manuscript development was guided by the PRISMA Statement,9 and a PRISMA checklist was completed (online supplementary appendix 3).
Results
Extent of available evidence
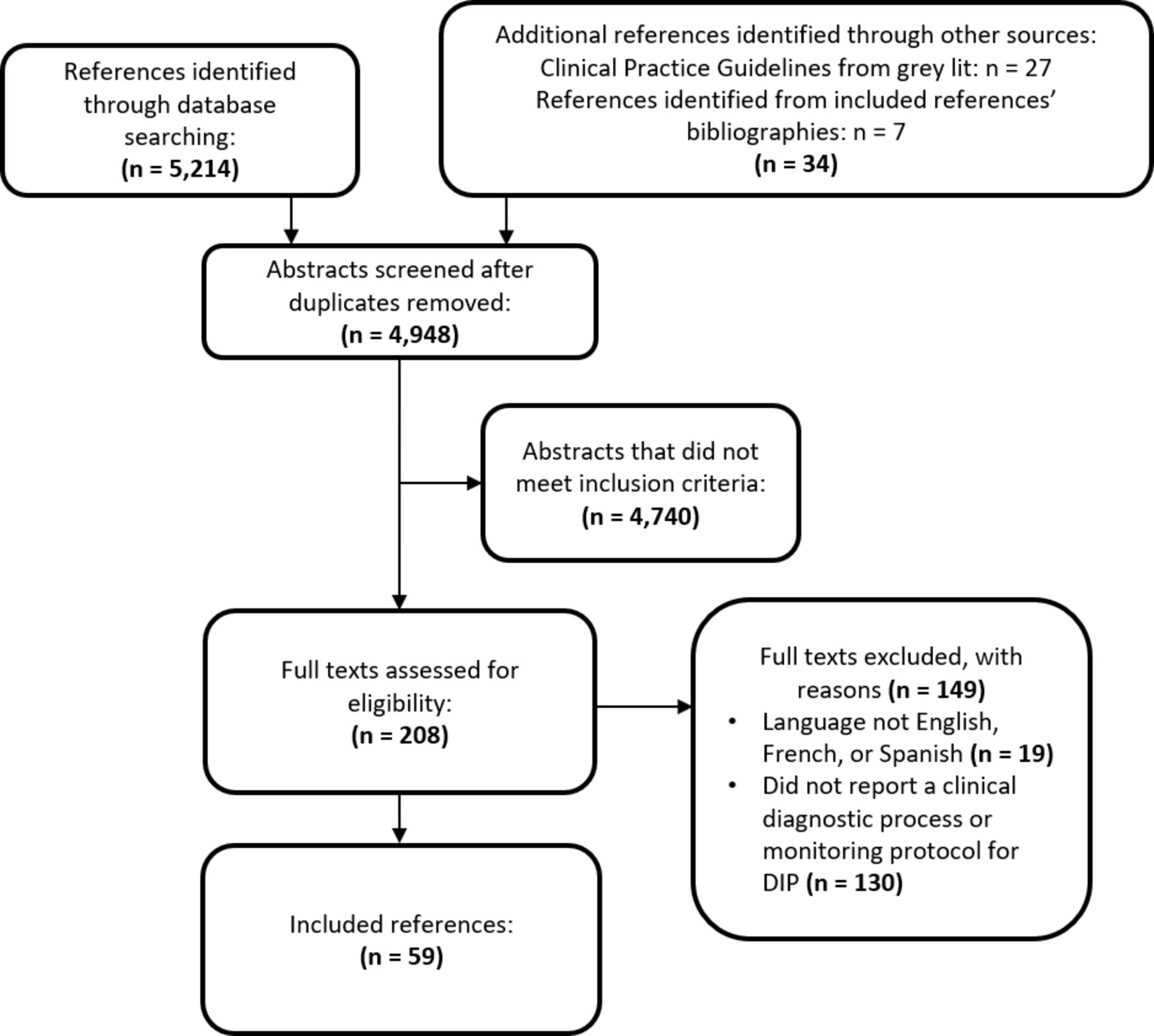
A PRISMA flow diagram summarises the process of study selection (figure 1). Out of 4948 references screened, 59 eligible studies were identified (table 1) — 14 reported on DIP detection,6 11–23 with seven of those also reporting a DIP diagnostic process, while 45 reported only a DIP diagnostic process.24–68 Forty per cent (n=23) of the studies were published between 2010 and 2016, 29% between 2000 and 2009 and 32% prior to 2000. Three countries published over half of the relevant studies: USA (36%), France (14%) and Italy (9%). A list of excluded studies has been provided in online supplementary appendix 4.
Characteristics of the 59 included studies
{kind=link}
Flow diagram describing the study selection process.
DIP detection methods and recommendations
Eleven primary studies and three narrative reviews reported data on DIP detection methods and/or recommendations (table 2). The studies focused on detection methods for patients taking PEG-asparaginase,17 19 22 23 L-asparaginase,11 15 valproic acid,12–14 didanosine,16 azathioprine18 and drugs in general.6 20 21 These studies have been summarised below by decade of publication.
Summary of recommendations from studies reporting DIP detection methods
DIP detection recommendations from the 1970s
One study was published in the 1970s.11 Samuels et al. (1976) conducted serial monitoring of 19 children receiving L-asparaginase treatment for hematological malignancies. Monitoring consisted of serial testing of serum amylase and lipase, and ultrasonography prior to treatment, then weekly thereafter. Not all patients were studied systematically — some were evaluated retrospectively and some prospectively; some did not receive extensive testing or only received ultrasounds after the development of clinical signs or elevated serum pancreatic enzymes. The authors reported that ultrasonic diagnosis of pancreatitis ‘agreed with laboratory data in 18 of 19 patients’; however, a diagnostic definition of pancreatitis was not provided, making interpretation of their data difficult. Ultrasound was positive before pancreatic enzymes rose in two patients that developed AP; several other patients appear to have had an enlarged pancreas on ultrasound without developing pancreatitis, with false-positive leukaemic infiltration of the pancreas and peripancreatic lymphadenopathies occurring in some patients. The authors commented that some children presented no abnormal laboratory findings or clinical symptoms until immediately before death due to AP; however, they concluded that serial ultrasound was capable of depicting the natural development of AP. They summarise by stating that ultrasound permitted the diagnosis of subclinical AP, allowing for withdrawal of L-asparaginase prior to serious injury.
DIP detection recommendations from the 1980s
Four studies with DIP detection data were published in the 1980s.12–15 Torelli et al 13 evaluated the serum amylase of 27 patients about to start valproic acid (VPA) therapy, of which 18 had a second sample after 1 month, and nine had a third sample after 6 months of treatment. Serum amylase increased significantly after 1 month and remained high at 6 months; however, the values were considered within normal limits. No patients developed AP. The authors recommended that serial amylase testing could not be justified in VPA patients, given the expected slight increases in amylase, the lack of an accumulating metabolite, the rapidity of onset of AP and the rarity of cases in the literature.
Bale et al 12 monitored the serum amylase of 61 patients monthly during VPA therapy. Elevated serum amylase was identified in 20% of patients (n=12); however, serum amylase values did not correlate with dose or serum level of VPA. All 12 patients continued to receive VPA and serum amylase returned to normal spontaneously. The authors advised that serum amylase may be transiently elevated with VPA therapy, without predicting AP; thus, serial monitoring in asymptomatic patients may not be warranted.
Wyllie et al 14 reported a case series of four patients with AP associated with VPA. Serial monitoring was not conducted in any of the patients; however, the authors commented that transient hyperamylasaemia does not correlate with clinical AP in asymptomatic patients, citing Bale et al.12 They recommended that VPA be withdrawn if symptomatic AP appears but that serial monitoring of serum amylase in asymptomatic patients is not necessary.
Nguyen et al 15 conducted serial serum amylase testing and pancreatic ultrasonography in 92 children with lymphoproliferative diseases that were treated with L-asparaginase. Studies were conducted at baseline, partway through treatment, and at the end of treatment, although a strict protocol was not followed. Eleven patients (12%) developed at least one abnormal parameter that was suggestive of pancreatitis, and six patients (7%) developed AP. If it appeared, ultrasonographic evidence of early/subclinical AP occurred after clinical and/or laboratory abnormalities were present (n=2), and in two other patients that developed AP, the mid-treatment ultrasound was normal. No correct decisions to alter treatment were based solely on ultrasonographic findings. The authors advised that serial ultrasounds are not useful in the early detection of AP in L-asparaginase patients.
DIP detection recommendations from the 1990s
Two studies reported on DIP detection methods in the 1990s.16 17 Maxson et al 16 conducted a retrospective analysis of data from a prospective clinical trial of 51 AIDS patients treated with didanosine (ddI). Clinical and laboratory testing were performed at least every 3 to 4 weeks, with a mean follow-up of 8.2 months. Twelve patients (24%) developed AP, and two of these patients demonstrated asymptomatic elevations of pancreatic enzymes that progressed to pancreatitis within 2 weeks. Twenty other patients (39%) demonstrated asymptomatic elevations of pancreatic enzymes that did not progress to AP. We calculated the sensitivity (17%) and specificity (49%) of early elevated serum amylase as a test for later development of AP. Despite these low values, the authors stated that serial monitoring of pancreatic function and early identification of risk factors in AIDS patients on ddI may be essential to avoid AP.
Chambon et al 17 reported on two cases of AP associated with PEG-asparaginase therapy, neither of which received serial monitoring. They challenged the findings of Samuels et al (1976),11 pointing out the weaknesses of ultrasound in that study (weekly ultrasounds in PEG-asparaginase patients were prone to false-positives due to adenopathies and leukaemic infiltration and false-negatives due to gas-filled bowel obfuscating the pancreas). The authors instead recommended that all PEG-asparaginase patients with suspected AP undergo further examination for the following signs of pancreatic necrosis within 24 hours, and asparaginase discontinued if present: (1) lactate dehydrogenase >270 IU/L, (2) C-reactive protein >100 mg/L, (3) alpha-2 macroglobulin <1.3 g/L and (4) contrast CT of the pancreas.
DIP detection recommendations from the 2000s
Five studies commented on DIP detection methods in the 2000s.6 18–21 Castiglione et al 18 conducted a retrospective review of 30 Crohn’s disease patients that had received azathioprine (AZA). All patients underwent monthly serum amylase and transaminase assays for the first 3 months of treatment, with pancreatic isoenzyme evaluated in all cases of hyperamylasaemia. Three patients developed moderate AP; however, no comment was made regarding the results of serial testing. Additionally, prospective testing was performed in 46 Crohn’s disease patients on AZA, each receiving weekly serum amylase evaluation for the first 8 weeks of treatment. Hyperamylasaemia was detected in three cases, resulting in discontinuation of AZA; however, there was no clinical or ultrasound evidence of AP in these cases, and no other cases of AP developed. The authors commented that serial amylase testing during the first 2 months of AZA therapy in Crohn’s patients could prevent the development of AP, allowing early withdrawal of treatment.
Laugel et al (2005)19 did not conduct serial monitoring in their study of clinical aspects of asparaginase-induced AP in children. However, citing two references,69 70 they advise that serial monitoring of serum amylase is a ‘late and imperfect means of detecting AP’ because at the time of first clinical signs, serum amylase and lipase may still be normal or only moderately increased. They suggest that serial monitoring is not useful except perhaps to establish a baseline on which laboratory results can be compared, should clinical signs develop.
Three narrative reviews made comments regarding serial monitoring to detect DIP.6 20 21 Dhir et al. (2007)20 cited Maxson et al (1992) and Nguyen et al (1987)15 16 in concluding that although patients should be carefully monitored for clinical AP, the use of serial serum pancreatic enzyme testing is not advocated, even for drugs associated with a high incidence of AP, and that drug withdrawal based on asymptomatic amylase elevations should not be universally applied. The second narrative review by Balani and Grendell6 cited the above review,20 while also pointing out the rarity of DIP in their recommendation against routine monitoring of asymptomatic patients. Instead of serial monitoring, they suggested that prevention of DIP should be grounded on recognition of high-risk medications and patients, maintenance of a high index of suspicion and immediate withdrawal of medication once AP is suspected. The third review21 cited Balani and Grendell in advising against serial monitoring.
DIP detection recommendations from the 2010s
Two studies by Raja et al (2015, 2017)22 23 conducted weekly serial monitoring for DIP in children on PEG-asparaginase. In the first study,22 pancreatic ultrasound was conducted weekly for 10 weeks on 19 children, then every 2 or 6 weeks, depending on the patient’s randomised treatment schedule. Three cases of AP developed in the first 10 weeks, all with signs of AP on ultrasound at the time of diagnosis; however, none demonstrated ultrasonographic evidence of AP prior to diagnosis, with the last ultrasounds conducted at 10, 11 and 16 days prior, respectively. The authors concluded that oedema does not develop gradually in asparaginase-induced AP (ie, asparaginase-induced AP develops acutely) and, thus, serial ultrasound is not useful to monitor for the development of AP or to identify patients at risk of experiencing AP prior to the event.
In the second study,23 pancreatic enzymes and lipid profiles were monitored weekly for 10 weeks in 31 children, then every 2 or 3 weeks, depending on the patient’s treatment schedule. Seven patients developed AP; however, although pancreatic enzyme levels may elevate during therapy, they did not gradually increase during treatment, but instead were suddenly significantly elevated at the time AP developed. It was concluded that early detection of asparaginase-induced AP was not possible by serial monitoring of pancreatic enzymes or triglycerides, and that persistent enzyme elevations above three times the ULN may be incorrectly diagnosed as AP, if the patient were to develop stomach pains for other reasons.
Summary of recommendations for DIP detection
Early evidence suggested that serial pancreatic ultrasound could detect subclinical pancreatitis in patients receiving medications associated with AP, allowing the discontinuation of medication prior to development of clinical disease.11 However, subsequent studies have disputed this claim,15 17 22 23 and have demonstrated no utility of serial ultrasound in early AP detection. The two studies in which serial monitoring of pancreatic enzymes was useful were conducted on patient populations with an increased risk of AP due to their underlying condition (ie, AIDS and Crohn’s disease).16 18 Other studies have recommended against serial monitoring of pancreatic enzymes to detect DIP. Other than the study of Crohn’s disease patients taking AZA,18 no study advised to discontinue medication based on asymptomatic pancreatic enzyme elevation.
DIP diagnostic processes
Fifty-two studies reported a DIP clinical diagnostic process (table 1)—one clinical practice guideline,36 16 narrative reviews6 20 21 24 26 27 29 33 35 40 42 48 62 64 67 68 and 35 primary studies.14 16 17 19 25 28 30–32 34 37–39 41 43–47 49–61 63 65 66 The single clinical practice guideline was published following a consensus conference in France on AP and provided a chapter on DIP causality assessment.36 Thirteen of the 16 narrative reviews focused solely on DIP, while the remaining three were more general reviews of AP. One primary study16 diagnosed DIP as an a priori specified outcome, while all others diagnosed DIP as part of patient inclusion criteria. Nine studies focused solely on paediatric patients.19 35 37 39 50 55–57 63
Several studies presented algorithms for the diagnosis of DIP that generally followed the same format: (1) confirm the diagnosis of AP and (2) determine the cause of AP.20 24 34 36 48
Diagnosis of AP
Thirty-seven studies reported AP diagnostic criteria, with only eight (22% of 37 studies) using the criteria established by international consensus (see Methods section).6 21 47 49 51 55 61 65 The international consensus process was begun in 2007 and published in 2012. First evidence of reported use of these criteria in our included studies was in a narrative review in 2008.6 Thirty-one per cent of studies published after 2007 (8 of 26) and 18% of studies published after 2012 (2 of 11) used the international consensus AP diagnostic criteria. Twenty-nine studies reported diverse and sometimes incomplete AP diagnostic criteria (see online supplementary Appendix 5). Sixteen studies (31%) reported no AP diagnostic criteria and only described causality assessment.17 19 20 27 29 31 36 40 45 53 56 59 62 66–68
Determination of a drug-related cause
Determination of a drug-related cause was achieved through two general methods: (1) the use of DIP-specific causality criteria cited from the literature or (2) the use of generic adverse drug reaction causality criteria cited from the literature.
DIP-specific causality criteria
Several studies presented DIP-specific causality algorithms.20 24 34 36 48 67 68 Mallory and Kern (1980)68 initially conducted a review of DIP case reports and classified the implicated drugs as having definite, probable or possible associations with AP according to presence of the following criteria:
Presence of a valid temporal relationship.
AP develops during treatment with the drug.
Clinical and biochemical abnormalities rapidly resolve on drug withdrawal.
Pancreatitis usually recurs on re-challenge.
Exclusion of all other causes of AP.
These criteria have subsequently been used in other studies not only to classify drugs,20 29 31 42 52 53 but also to impute a drug-related cause in the diagnosis of individual cases of DIP.17 38 49 53
Delcenserie (1992 and refined in 2001)27 36 presented an in-depth algorithm to impute causality of DIP, using data from two assessments: (1) the temporal aspects of the disease, including latency (ie, the time from first drug administration until development of AP), disease pattern following drug discontinuation, and re-challenge and (2) clinical criteria, including evidence of highly suggestive disease patterns (eg, evidence of allergy, hypertriglyceridaemia, hypercalcaemia in patients on drugs known to be associated with these), exclusion of all other non-drug causes and elevation of serum drug levels. Using these data and cross-tabulation of tables, the likelihood of DIP causality can be estimated. Three of our included studies cited Delcenserie’s methods19 32 41
Flow charts were used by several authors to depict the steps of DIP causality assessment.20 24 34 48 67 These generally were visual depictions of Mallory and Kern’s (1980) criteria,68 with various refinements. Steinberg, 198524 presented a flow chart that included the initial exclusion of obvious non-drug causes, determination of whether the patient was taking a drug associated with AP, clinical course after drug discontinuation and effects of re-challenge. Eland et al, 199934 presented a similar graphical; however, only gallstones and alcoholism were excluded as non-drug aetiologies. Trivedi and Pitchumoni, 200567 presented an algorithm that considered malignancy as a non-drug cause initially, as well as alcoholism, gall stones, microlithiasis, hypertriglyceridaemia and hypercalcaemia. If none of these causes were apparent, DIP was considered if the patient was receiving one of the many drugs associated with DIP identified in their review of case reports. Other numerous causes of AP (see table 3) were to be ruled out if the patient was not receiving a listed drug or if the clinical course did not fit DIP following drug withdrawal. This algorithm was cited by two other included studies.49 51 Flow diagrams reported by Dhir et al, 200720 and Nitsche et al, 201048 were similar to that of Trivedi and Pitchumoni (2005), although Nitsche et al suggested integrating a generic adverse drug reaction causality assessment tool, not found in their graphic.71
Non-drug causes of AP that were excluded in the 44 studies that included exclusion of non-drug causes as part of the DIP diagnostic process
Temporal aspects related to latency, drug discontinuation and AP resolution and re-challenge were key components in the DIP-specific causality criteria reported above. Many of our included studies indicated that the shorter the latency, the more suggestive of DIP (assuming other conditions were met)25 27 42 60 61 66 however, other studies commented that DIP could occur several months to years after the start of medication,20 27 36 42 or after discontinuation of short-term medication.36 A typical latency (ie, consistent with the literature for the drug in question) has also been proposed as suggestive of causality,17 20 32 36 61 66 which takes into consideration the underlying pathophysiological mechanism. Regarding drug discontinuation, some studies suggested that there should be a rapid disappearance of symptoms,27 33 36 42 followed by a slower decrease in pancreatic enzymes.27 36 42 One study advised that resolution of symptoms may be coincidental with drug discontinuation, and thus, is not confirmatory of DIP.64 If AP did not recur after drug discontinuation, many felt the suspicion of a drug-related cause was heightened.17 27 32 33 38 44 52 Most studies considered a positive re-challenge to be confirmatory; however, patients with idiopathic pancreatitis or microlithiasis may have recurrent attacks of AP coincident with de-challenge and re-challenge.62 Re-challenge was considered unethical if a drug-related association was already suspected in the literature,14 27 33 36 39 44 49 63 but unintended re-challenge was known to occur.49 61 Others commented that re-challenge should only be attempted if the benefit of the medication outweighs the risk of another potentially severe episode of AP.21 29 48 67
In imputing a drug-related cause, several studies required identification of either previous AP cases associated with the drug in the literature or a previous determination of an association between the drug and AP. Beyond a literature search, reported sources of cases and associations included the American Gastroenterological Association Technical Bulletin on Acute Pancreatitis,72 the French database ‘Pancreatox’ (http://drugsoft.com/pancreatox.html) and articles by Trivedi and Pitchumoni,67 Andersen et al,73 Eland et al 34 and Lankisch et al.28
Exclusion of at least one important non-drug cause of AP was a key element of DIP-specific causality assessment in 44 studies. table 3 presents the nine most commonly excluded non-drug causes of AP reported. The non-drug causes were numerous, variable across studies and may have changed over time (eg, the first evidence of exclusion of autoimmune causes of AP in our sample was in 2001). Many studies (n=24) claimed to have ‘excluded all other causes’, without explicitly defining the other causes, precluding synthesis of these data. The most commonly excluded non-drug cause of AP was biliary disease, including gallstones, biliary sludge or crystal development. Algorithms of hierarchical testing74 75 have been reported that could rule out more common aetiologies of AP before embarking on more invasive or costly tests to evaluate less likely causes.40 The exclusion of other drugs as causative agents of DIP was considered in 14 studies.6 14 16 20 25 29 30 36 38 40 46–48 52 McArthur commented that it is difficult to evaluate the contributions of other drugs in the development of AP.29 Spanier et al, suggested classification of all drugs being administered at the time of AP onset using the Badalov system,7 while Delcenserie recommended measurement of serum levels of administered drugs with a known dose-dependent toxic mechanism for DIP.36 No studies discussed the potential for drug interactions that may potentiate DIP.
Generic adverse drug reaction causality criteria
Four tools to assess causality of potential adverse drug reactions generically (ie, not DIP specifically) were used by seven of the included studies,45 46 48 49 51 61 62 including The WHO Probability Scale,76 77 The Naranjo criteria,78 criteria developed by Karch and Lasagna71 and Hill’s criteria of causation.79 These tools were used in addition to considerations of temporal aspects of the case and exclusion of non-drug causes, to determine the likelihood of a suspected drug-related cause.
Discussion
The prevailing opinion of the included studies in this review is that serial monitoring to detect early cases of AP is unwarranted in patients receiving medications with the potential to cause DIP. Patients with a higher risk of AP due to an underlying disease (eg, those with Crohn’s or AIDS) may be the exception, and thus may benefit from serial monitoring, although the evidence for this is based on single studies and this hypothesis has not been tested in a randomised controlled trial. Several studies demonstrated that serial monitoring could not differentiate between patients in whom AP will or will not ultimately arise. As well, some drugs may induce significant and persistent elevations of serum amylase or lipase unrelated to AP, putting those patients at risk of misdiagnosis of AP should abdominal pain arise due to other causes. Cases of DIP occurred acutely, without a continuous gradual elevation of pancreatic enzymes or a gradual accumulation of pancreatic oedema on ultrasound. Thus, asymptomatic elevations of pancreatic enzymes could not predict AP, and evidence of AP on ultrasound generally did not appear until patients were symptomatic. As stated by Laugel et al,19 serial monitoring is a ‘late and imperfect means of detecting AP.’
Our review also identified that diagnosis of DIP is not standardised across the literature. Although AP diagnostic criteria have been generally accepted, the uptake of these criteria by researchers has been low, even in recent publications. Similarly, there were substantive differences across studies in the methods used to impute causality in DIP. Lack of standardisation in DIP diagnostic criteria can significantly influence the classification of drugs with respect to their association with AP. Current classification systems rely on synthesis of DIP case reports in the literature.7 However, accurate drug classification is only possible when DIP case reports correctly diagnose DIP using currently accepted AP diagnostic criteria and appropriate imputation of causality. Lack of use of standard diagnostic and causality criteria can lead to information bias resulting from (1) misdiagnosis of other gastrointestinal disease as AP and (2) incorrect attribution of cause to a drug when it is not. The numbers of published cases of DIP apparently associated with a drug can become inflated, potentially leading to a higher risk of pancreatitis being assigned than is warranted.
Similarly, a lower risk of pancreatitis may be assigned to newly approved drugs than what is warranted. Without an accurate method of detection of DIP during clinical trials required for the new drug approval process, cases of pancreatitis may be missed. For example, publicly available United States Food and Drug Administration (FDA) documentation demonstrates that in April 2014, a concern regarding an association between ceritinib (Zykadia, Novartis Pharmaceuticals Corporation, East Hanover, New Jersey) and pancreatitis was raised by FDA New Drug Application (NDA) reviewers.80 However, the available evidence from the submitted trial data did not substantiate an association because no clinical cases of confirmed pancreatitis had been found.80 Pancreatitis was identified as a potential serious adverse reaction of ceritinib based on clinically significant elevations in serum lipase that occurred during clinical trials and preclinical findings submitted as part of the approval process.81 One year later, a warning regarding pancreatitis was added to the Zykadia label by the FDA. The original NDA reviewers suggested that cases of pancreatitis may have been misclassified as general gastrointestinal (GI) toxicity during pre-approval trials due to the almost universal presence of GI symptoms among the patients.81 An accurate method of DIP detection or application of the currently accepted AP diagnostic criteria may have attributed some cases to pancreatitis and confirmed an association between ceritinib and DIP prior to approval.
No reviews of the literature have previously been published that have evaluated DIP detection or diagnostic processes reported in the literature, thus, we have no comparison for our findings. Our review had both strengths and weaknesses. We used robust systematic review methods, including development and registration of an a priori protocol. We elected to include both review papers and primary studies to encompass as wide an evidence base as possible. Our search strategies were designed to be broad enough to capture all relevant reviews of DIP; however, for primary studies, it is impossible to screen all trials of all drugs ever evaluated. Thus, our primary search strategy was designed to capture studies that contained vocabulary and key words related to diagnostic processes associated with DIP; trials that may have used a DIP diagnostic process but that were not indexed by vocabulary related to DIP would not have been captured, a source of potential selection bias. As well, given the non-quantitative approach to synthesis, a degree of confirmation bias may be inherent in the inferences drawn. We attempted to minimise confirmation bias through discussion of the data and the inferences drawn among all members of the review team as well as clinical experts. As well, to improve transparency of our inferences, in an appendix we have reported direct quotes from the included papers that illustrated key points and positions with respect to DIP detection (online supplementary appendix 5). Similarly, all raw data and syntheses have been provided in online supplementary appendix 6.
Supplemental material
The available evidence indicates that serial monitoring of pancreatic enzymes or ultrasound to detect cases of DIP is not warranted, even in patients receiving drugs with established associations with pancreatitis. Thus, detection of DIP in clinical trials remains elusive given its rare occurrence in the smaller sample sizes found in many trials, and given that more medically complex patients at higher risk of DIP are commonly excluded from clinical trials. For government drug regulatory bodies interested in identifying new drugs with high risk of AP prior to marketing approval, no recommendations could be made regarding serial monitoring methods to detect DIP in clinical trials. Future research efforts in identifying more specific biomarkers for earlier identification of pancreatitis or pharmacogenomic testing to identify a higher risk group of patients in whom a greater risk of pancreatitis could be predicted would be useful to clinicians, trialists and regulatory bodies. In the meantime, reliance on heightened clinical awareness, identification of high-risk patients and the use of standardised diagnostic and causality criteria remain key to DIP detection and diagnosis.
Acknowledgments
We would like to thank Raymond Daniel for assistance in reference management and acquisition of full texts. We acknowledge staff from the CIHR/DSEN Coordinating Office for coordination of activities related to the development of the funding application.
References
Footnotes
Twitter @dmoher
Contributors DW contributed to protocol development, study design, screening, data extraction, data synthesis and drafting of the manuscript and revisions. BH contributed to protocol development, study design, data synthesis and manuscript review. FY contributed to protocol development, study design, screening, data extraction, data synthesis and manuscript review. SK contributed to protocol development, study design, content expertise, data synthesis and manuscript review. BS developed search strategies and conducted literature searches. DM contributed to manuscript review.
Funding This work was supported by the Canadian Institutes of Health Research and the Drug Safety and Effectiveness Network. The funders had no role in the selection of study methods or formation of the conclusions drawn from this work.
Competing interests BH has previously received honoraria from Cornerstone Research Group for methodologic advice related to the conduct of systematic reviews and meta-analysis.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.