Article Text

Abstract
Objective Evaluate the urinary, bowel and sexual function as well as stress symptoms and depression in a sample of the Swedish population.
Design A random sample of Swedish men and women in age groups from 30 to 89 years, a total of 3000 individuals, were contacted and after receiving informed consent, a questionnaire was sent.
Main outcome measures Measures of urinary, bowel, sexual function and quality of life.
Results The questionnaire was sent to 2094 individuals who gave informed consent. The questionnaire was answered by 1078 individuals. Quality of life, stress symptoms and depressed mood were relatively constant across age groups for both men and women. Urinary function differed significantly across gender and age groups, but bowel function was relatively unaffected by age. Overall bowel dysfunction was slightly more prevalent among women compared with men. For both men and women, the frequency of intercourse or other sexual activities decreased with age, whereas sexually associated distress increased by age in men, but decreased among women.
Conclusions In a general population, the urinary function varied across age and sex. Overall bowel dysfunction was slightly more prevalent among women compared with men. Sexually associated distress increased by age for men, but decreased for women.
Trial registration number NCT02392923; Results.
- general population
- urinary incontinences
- urogenital function
- quality of life
- epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
A population based sample including both sexes and different age groups enabling an assessment of differences across age groups and sex.
Validated questionnaire on urogenital function.
A high rate of non-responders is a limitation.
Introduction
Several conditions such as various forms of cancer in the urinary and gastrointestinal tract as well as their treatment may cause complications such as urinary incontinence, faecal incontinence, sexual dysfunction, stress symptoms and depression. The prevalence and severity of such types of dysfunctions have been addressed for patients with rectal cancer1 and those with prostate cancer,2 respectively. Bowel dysfunction, prevalent among up to 60% of patients with rectal cancer,3 consisting of incontinence for flatus and/or faeces, urgency, constipation, fragmentation and frequent bowel movements is referred to as the low anterior resection syndrome (LARS).4
Some of these complications are specific as a consequence of treatment such as stoma-related symptoms. Many symptoms, such as incontinence and sexual dysfunction, are however also present in a general population, where prevalence and severity may vary with gender and age. In order to assess to what extent the prevalence and severity of these symptoms are related to the disease, it is relevant to assess the symptoms in a general population.
For established generic instruments such as SF 36, EQ5D as well as cancer-specific instruments, such as EORTC QLQ, results from reference populations are available.5–7 However, for specific instruments, such as the LARS score,4 8 validated and constructed for certain groups of patients, corresponding results from reference populations are rarely available.
The aim of this study was to evaluate urinary, bowel and sexual function, stress symptoms, quality of life and depressed mood in a sample of the Swedish population.
Methods
Study design
A random sample of the Swedish population born during the years 1924–1983, a total of 3000 individuals, was retrieved from the Swedish Inland Revenue (Skatteverket). Each individual was identified by their personal identity number. The postal address for each individual was found using the population registry. Telephone numbers are not in the registry, but were retrieved from various search engine websites. People with unlisted numbers could not be contacted by telephone. The random sampling was stratified with regard to age groups (30–39, 40–49, 50–59, 60–69, 70–79, 80–89 years) and sex aiming at 250 individuals in each decade and sex, rendering a total of 3000 individuals, to make the sample representative of the general Swedish population. Each individual in the sample received a unique study ID number. The individuals were contacted by mail with information about the study followed by telephone contact, if possible. Individuals were included after giving informed consent and received a questionnaire, as well as a prepaid return envelope. For individuals who could not be reached by phone, an information letter and the questionnaire were sent together with the informed consent form and a prepaid return envelope. A ‘Thank you’/reminder letter was sent 2 weeks later. Subject enrolment started in June 2014 and the study was completed in November 2015. The trial was approved by the Board of Ethical Approval in Gothenburg, Sweden (registration number 608-13).
Questionnaire development
The questionnaire was constructed according to the approach proposed by Steineck et al 9 as a means for symptom assessment in cancer survivors. In this approach, rather than summarising items into a single score, one symptom at a time is considered and its nature, occurrence, intensity, duration and associated distress are documented. This approach was used for constructing questionnaires used in patients with prostate cancer10 and rectal cancer.1 11 The validation process involved content validation, that is, verifying that the questionnaire and the included items are relevant for the purpose, followed by an assessment of face validity, that is, the researcher sits face-to-face with patients in order to assess their comprehension and ability to relate to the items. One feature of this approach is the provision of a sufficient number of response categories for the subject to relate to. In the subsequent analyses, response categories can be combined as needed. In the construction of the questionnaire, items considered relevant for a general population were chosen from aforementioned questionnaires and thereafter validated (content and face). A selection of the items is presented in the online supplementary file 1.
Supplemental material
The LARS score questionnaire4 8 was not included in this study. However, based on items similar to the five items in the LARS questionnaire, a scoring similar to the LARS score was used to classify individuals as having no, minor or major bowel dysfunction (see the online supplementary file 1).
The questionnaire also included questions on socioeconomics (marital status, education, occupation and origin), comorbidity, physical activity (4-level Saltin-Grimby Physical Activity Level Scale12), alcohol consumption (AUDIT-C),13 14 smoking habits,15 health-related quality of life (EQ-5D-3L)16 as well as questions on intrusive thoughts17 and the 29-item Sense of Coherence scale (SOC-29).18 19
Data analysis
To enable 80% power to detect a 10% prevalence difference between each of the six 10-year age groups, the study aimed at 350 evaluable individuals in each of the groups. Assuming a dropout rate of 30%, the required number in each of the age groups was 500 with a total of 3000 individuals. Due to a higher drop-out rate than anticipated, age was categorised into 20-year groups.
Men and women who scored ≥5 and ≥4 points on AUDIT-C, respectively, were classified as hazardous drinkers.20
If at most 25% of the 29 items were missing prior to the calculation of the SOC-29 total sum score, the missing values were replaced by the median score for the remaining answered items. If >25% of items had missing values, the total score was defined as missing.
For group comparisons a χ2 test was used for categorical data and a Kruskal-Wallis test for continuous variables. Men and women were analysed separately. No imputation technique was used for handling missing data.
Patient and public involvement
The target population was the general Swedish population. Individuals included in the study were Swedish inhabitants from age 30 to 89. No specific patient group was included in the study.
Results
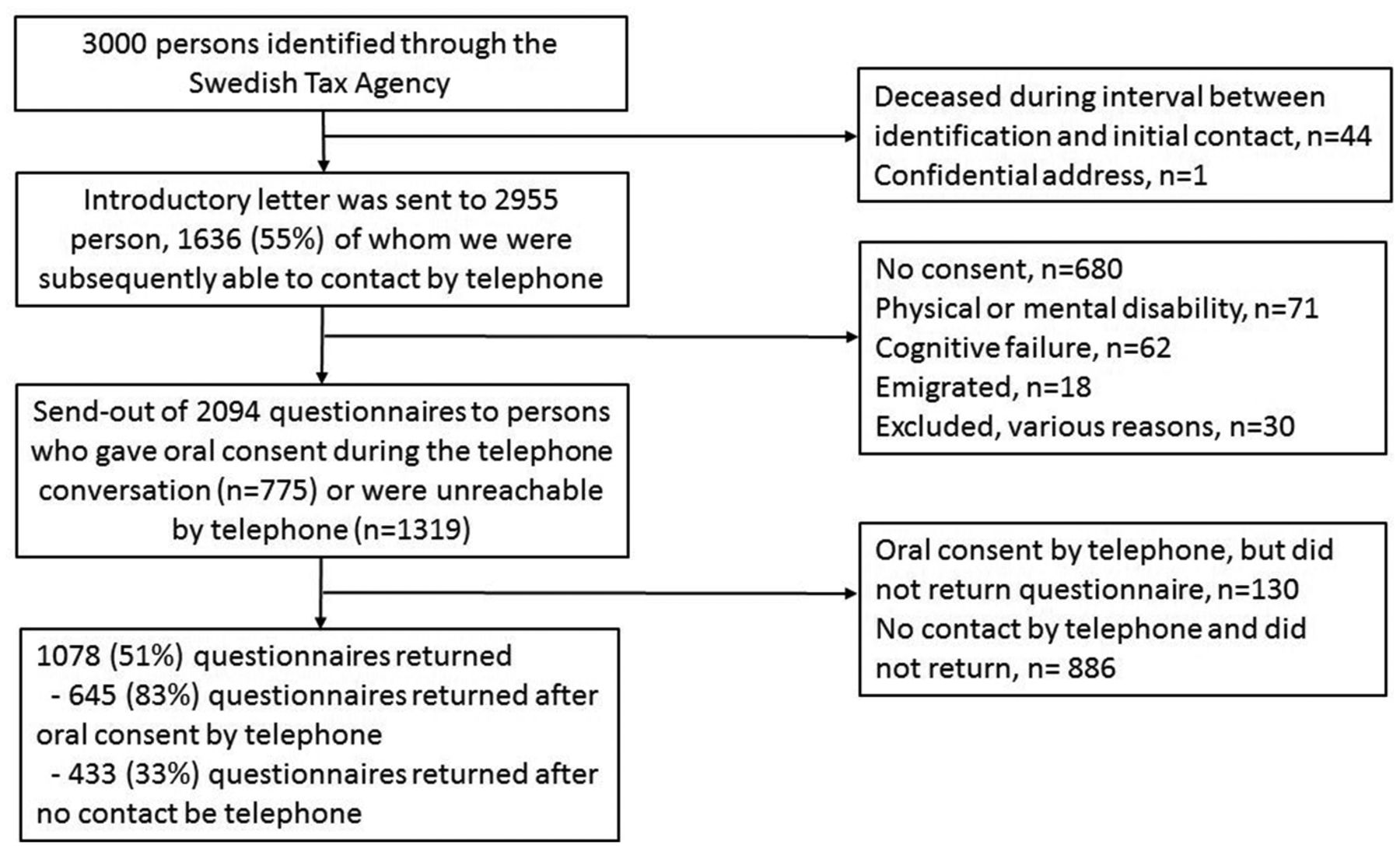
Of the 3000 individuals identified through the Swedish Inland Revenue, questionnaires were sent out to 2094 individuals. The questionnaire was answered by 1078 individuals rendering a response rate of 51% (figure 1).
{kind=link}
Flow chart of individuals included in the population sample.
Demographics are shown in table 1. There was equal distribution between sexes. A majority of the individuals were >60 years of age and half were retired. Seventy-seven per cent were in a relationship. Sixty per cent rated themselves as lightly physically active, 13% as current smokers and 28% of the men and 26% of the women had a hazardous drinking behaviour. Additional tables are presented in the online supplementary file 2 (see table 2).
Supplemental material
Demography and subject characteristics
List of tables presented in the online supplementary file 2
Quality of life, stress symptoms and depressed mood
Quality of life, stress symptoms and depressed mood were relatively constant across age groups for both men and women (online supplementary table S1a and S1b). Negative intrusive thoughts at least once per week were more common among women than men in the age group of 30–39 years with a prevalence of 38% and 21%, respectively. Sense of coherence was positively correlated with global health-related quality of life (Spearman correlation 0.52).
Urinary and bowel function
Among both sexes, urinary function differed significantly across age groups, with a prevalence of weakened urine flow, difficulties emptying the bladder and use of protective measures against urinary leakage increasing with age. Urinary leakage, measured as use of protective continence products as well as frequency of leakage, was more common among women than men. Daytime leakage was more common than night time leakage (online supplementary table S2).
Bowel function was relatively unaffected by age among both men and women. Dysfunction was slightly more prevalent among women compared with men. Faecal incontinence increased with age among both men and women, but differed only between sexes in the age group of ≥80 years . The frequency of emptying the bowel was higher among men. (online supplementary table S3).
Sexual function
Among both sexes, the frequency of intercourse or other sexual activity decreased with age. At higher age groups, sexual activity was more common among men than women. Satisfaction with sexuality was relatively stable among women, but decreased at higher age among men (online supplementary table S4a). The proportion of men experiencing a deterioration of sexual function increased with age. The prevalence of the associated distress also increased (online supplementary table S4b). Among women, the frequency of occasions with sexual arousal decreased with age. A majority of women did not experience sexual problems. The proportion of women who regarded their sexual problems as bothersome decreased with age (online supplementary table S4c).
Discussion
The results from our study show that quality of life, stress symptoms and depressed mood are relatively constant across age groups for both men and women. In a general population, the urinary function varied across age and sex. Urinary leakage was more common among women compared with men. Overall bowel dysfunction was slightly more prevalent among women compared with men. For both men and women, the frequency of intercourse or other sexual activities decreased with age. Whereas the sexually associated distress increased by age for men, it decreased for women.
Thirteen per cent rated themselves as smokers which is above the average rate of 9% in Sweden.21 The prevalence of hazardous drinking of 28% for men and 26% for women was similar to what was observed in the Swedish National Survey of Public Health from 200622 but higher (with regard to AUDIT-C mean score) than a survey from 200123.
Both sense of coherence score and global health-related quality of life levels were similar to previous observations.19 24 25
The attitudes to the factors addressed here have changed a lot during the 20th century, with more openness and less taboo, especially with regard to sexuality. In Beckman et al’s 26 study, the quantity and quality of sexual activity among Swedish 70 year olds was seen to be improved and increased over a 30-year period. Our findings confirm their results that intercourse is more common among men than women, but found no differences regarding sexual satisfaction. It is interesting that historically the satisfaction has increased for women, but decreased for men.26 However, when addressing functional aspects in general and during sexual arousal, it was common among elderly women to respond ‘Don’t know’ and ‘Not applicable’, respectively. A more thorough assessment of this group would be desirable.
The results from this study may serve as a benchmark for comparison with the prevalence and severity of symptoms in patient populations. Besides differences across populations, prevalence estimates based on patient reports also depend on several other aspects such as what scales were used (symptom severity scales or functional symptom criteria), definitions of outcomes and how the questionnaire is constructed and administered. The approach for symptom assessment used here may differ in various ways from other scales. In the systematic review by Sharma et al 27 based on the ROME II criteria for faecal incontinence,28 the overall prevalence range was 4.2%–7.6%. This is similar to our results, although the frequency increased much more with age in our study. The prevalence of constipation and faecal incontinence was otherwise similar to the levels observed in previous studies, see refs 29 and 30.
In Bedretdinova et al,31 using the Incontinence Questionnaire UI short form,32 the estimated prevalence of urinary incontinence among women in France was 17%. In another study,33 incontinence as defined by as self-reported involuntary loss of urine in the past 12 months was estimated to be prevalent among 2.7% and 13.9% men and women, respectively. Urinary incontinence as assessed among 382 Swedish women aged 20–59 years by the question ‘Do you suffer from involuntary loss of urine?’ rendered a prevalence of 24% at baseline and in 28% at follow-up.34 In the current study, incontinence as measured by use of protective measures and change of pad during 24 hours was present in 10%–14% among women in this age group.
Strengths of this study include a population-based sample including both sexes and different age groups, thereby enabling an assessment of differences across age groups and sex. The questions on urogenital function has been validated and used in studies of groups of patients. Limitations include the high dropout rate. One reason for this was the difficulty in identifying telephone numbers for a high proportion of the individuals. The response rate was 83% and 33% among individuals who were reached and unreachable by phone, respectively. This is in line with previous research35 and shows that pre-contact has a positive effect on response rate. Differences in response rate between individuals precontacted by telephone compared with by post have not been established. In our previous studies of patient populations using the same kind of questionnaire, the dropout rate is usually as low as 10%. The explanation may be that patients can relate to the content of the questionnaire more easily than individuals in a general population and that they are more supportive of this kind of research.
Acknowledgments
The authors gratefully acknowledge the participants, members of the steering committee and the personnel at the trial secretariat for their provision of study material and administrative support.
References
Footnotes
Contributors Research area and study design: EH, EA, EG and JH; data acquisition: EH; data analysis and interpretation: DB and EH; statistical analysis: DB; supervision and mentorship: EH. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved. DB takes responsibility that this study has been reported honestly, accurately and transparently; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Funding This work was supported by the Region Västra Götaland, Sahlgrenska University Hospital ALF grant ALFGBG-4307771.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The trial was approved by the Board of Ethical Approval in Gothenburg, Sweden (registration number 608-13).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Statistical programming code and datasets can be available upon request.