Article Text

Abstract
Objectives We examined trends of diagnosis-specific work disability before and after ischaemic heart disease (IHD).
Design Participants were followed 4 years before and 4 years after an IHD event for diagnosis-specific work disability (sickness absence and disability pension).
Setting and participants A Swedish population-based cohort study using register data on all individuals aged 25–60 years, living in Sweden, and who suffered their first IHD event in 2006–2008 (n=23 971) was conducted.
Results Before the event, the most common diagnoses of work disability were musculoskeletal disorders (21 annual days for men and 44 for women) and mental disorders (19 men and 31 for women). After multivariable adjustments, we observed a fivefold increase (from 12 to 60 days) in work disability due to diseases of the circulatory system in the first postevent year compared with the last pre-event year among men. Among women, the corresponding increase was fourfold (from 14 to 62 days). By the second postevent year, the number of work disability days decreased significantly compared with the first postevent year among both sexes (to 19 days among men and 23 days among women). Among women, mean days of work disability due to diseases of the circulatory system remained at a higher level than among men during the postevent years. Work disability risk after versus before an IHD event was slightly higher among men (rate ratio (RR) 2.49; 95% CI 2.36 to 2.62) than among women (RR 2.29, 95% CI 2.12 to 2.49). When pre-event long-term work disability was excluded, diseases of the circulatory system were the most prevalent diagnosis for work disability after an IHD event among both men and women.
Conclusions An IHD event was strongly associated with an increase in work disability due to diseases of the circulatory system, especially among men and particularly in the first postevent year.
- comorbidity
- disability pension
- sex differences
- sick leave
- sickness absence
- trajectories
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first nationwide population-based study on diagnoses of work disability (sickness absence and disability pension) before and after ischaemic heart disease (IHD) event.
Data were from reliable register-based measurements of high coverage and specificity, and no loss to follow-up.
Monitoring the sickness absence patterns and trajectories of patients after their IHD event may help to prevent permanent exit from the labour market.
While we could include many confounders related to sociodemographic characteristics and treatment procedures, register data also have their limitations; we had no information on traditional cardiovascular risk factors, psychosocial work environment, nor information on quality and outcome of postevent care.
Introduction
The risk of ischaemic heart disease (IHD) increases from the age of 45 among men and 55 among women.1 2 Thus, the onset of IHD is often at working age, and it has been linked with a high risk of work disability (sickness absence and disability pension).3–7 In Sweden, the estimated productivity losses and indirect costs of myocardial infarction were estimated to be 25 days, corresponding to indirect costs of €3465 per event during the year following the event.6 In addition to productivity losses, the direct medical costs of IHD are substantial.8 9
Comorbid conditions pose an additional risk to work ability: people with IHD and comorbid diabetes, mental disorders or musculoskeletal disorders are at a higher risk of work disability than those without these comorbid conditions.10–13 Alternatively, it is possible that other diseases, particularly depression and other common mental disorders, are more likely to occur after an IHD event than if no such event has occurred.14 15 This would, in turn, increase mental disorder-related work disability after an IHD event. These findings highlight the important role of comorbidity in relation to work disability among people with IHD. However, the causes of work disability before and after an IHD event remain unknown. Knowledge about the trends of diagnosis-specific work disability among people with IHD can be beneficial when planning specific interventions to promote the resumption of economic activity.
IHD manifests differently among women than among men, including clinical presentation, importance of particular risk factors, pathophysiology of disease and treatments/outcomes.16 17 While women are more at risk of work disability after an IHD event,10–12 18 coronary heart disease is generally more common and more fatal among working-aged men.19 Previous research has also suggested that sickness absence due to circulatory diseases may be a stronger predictor of death among men than among women.20 Thus, our aim was to investigate the trends of diagnosis-specific work disability, as indicated by sickness absence and disability pension, 4 years before and 4 years after an IHD event among men and women living in Sweden.
Material and methods
This cohort study was based on Insurance Medicine All Sweden research database, which is an individual-level register-linkage data covering about 12 million people over several decades nationwide. The population of Sweden in 2006–2008 was about 9.1–9.2 million, of whom 61% were aged 18–64 (in 2010) corresponding to about 5.5 million people.21 The study cohort consisted of all people living in Sweden, who at the event date in 2006, 2007 or 2008 were aged 25–60 years, had been living in Sweden for 5 years before the event and had no indication of IHD between 2001 and the event date. First event dates were included for all cases, except for cases in which death occurred within 30 days of the event, resulting in a sample of 23 971 cases. Thus, our study cohort with new-onset IHD in 2006–2008 represents roughly 0.5% of the same-aged population of Sweden.
An IHD event was based on hospitalisation or specialised outpatient care for myocardial infarction or other IHD, excluding angina pectoris (ie, codes I21‒I25 were included). The follow-up begun from the event date (T0) and continued for 4 years (T1 to T4). Before-event data were gathered 4 years prior to the event date (T−4 to T−1). The participants had to have survived until the event and 30 days after the event, but not necessarily thereafter. A total of 1184 deaths (5%) were observed during the four postevent years.
Data were obtained from several nationwide registers and linked with personal identity numbers. The following registers were used:
Statistics Sweden: Longitudinal Integration Database for Health Insurance and Labour Market Studies regarding sex, age, education, family situation, place of birth, type of living area and labour market activity.
National Board of Health and Welfare: Patient register: diagnosis-specific data on hospitalisations and specialised outpatient care (coded according to the International Classification of Diseases, 10th revision (ICD-10, WHO, 1994); medical treatment procedures; cancer register; date of death.
National Social Insurance Agency: information on sickness absence and disability pension benefits.
Outcome: diagnosis-specific work disability
Work disability was defined as days of annual sickness absence or disability pension, as indicated by sick leave and disability pension benefits. In Sweden, all people with income from work or unemployment benefits with reduced work capacity due to disease or injury are entitled to sick leave benefit. The treating physician evaluates whether the patient has a disease or injury and whether this condition impairs work capacity to the extent that the person is unable to work. In most cases, the first 14 days of sick leave are covered by the employer and thus not registered by the Social Insurance Agency. All individuals, including those with no previous income, can be granted disability pension if their work capacity is permanently reduced owing to the disease or injury.
We examined the following ICD-10 diagnostic groups: neoplasms (C00–D48); diabetes (E10–E14); other endocrine, nutritional and metabolic diseases (E00–E09, E15–E90); mental disorders (F00–F99); diseases of the nervous system (G00–G99); diseases of the circulatory system (I00–I99); diseases of the respiratory system (J00–J99); diseases of the digestive system (K00–K93); diseases of the skin and subcutaneous tissue (L00–L99); musculoskeletal disorders (M00–M99) and injuries (S00–T35, T66–T78, T79). Diagnostic groups of A, B, H, N, O, P, Q, R, V, Y, Z and U were not studied due to their infrequency in our cohort.
Confounding factors
Known risk factors for sickness absence and disability pension, that is, older age (continuous variable), lower education (‘low’ <10 years; ‘intermediate’ 10–12 years (high school); ‘high’ >12 years (college/university)), economic activity (‘in paid work’; ‘not in paid work’: unemployed, student, on parental leave, etc), not being married (family situation: ‘married/cohabitant’; ‘not married/cohabitant, no children’ (single); ‘not married/cohabitant with children’ (single parent)), living in smaller towns (large city’; ‘medium-sized town’; ‘small town/village’), and being born outside Sweden (‘Sweden’; ‘Other’) were treated as possible confounders. All confounders were measured at the event.
Having undergone an IHD-related medical treatment procedure was considered a proxy for a more severe event, and was also treated as a possible confounder. Medical treatment procedures were coded according to Nordic Medico-Statistical Committee Classification of Surgical Procedures.22 Procedures were registered during the year before the event (T−1) or the year after the event (T1), and included coronary artery bypass graft (FNA–FNE, FNH 20), percutaneous coronary intervention (FNG 02, FNG 05) and other coronary surgeries (FNF, FNG 00, FNG 10, FNG 20, FGN 22, FNG 30, FNG 96). Individuals with at least one such procedure were coded as ‘yes’ and those without as ‘no’.
Statistical analysis
Differences between men and women were tested using χ2 tests except for continuous variable age, for which one-way analysis of variance was used. We used the repeated measures negative binomial regression procedure and the generalised estimating equations method to produce least square means and rate ratios (RRs) and their 95% CIs to estimate trends and risk of diagnosis-specific work disability before and after an IHD event, except for work disability due to diseases of the circulatory system (I00–I99), where the estimates were produced using Poisson distribution due to conversion problems with negative binomial distribution. This method considers the intraindividual correlation between measurements.
To demonstrate the absolute levels of diagnosis-specific work disability, annual means of work disability were calculated for each diagnostic group for 4 years before and 4 years after the IHD event. As a supplementary analysis—to express the difference in the shape of the trajectory of work disability—we calculated the RRs per 4 years in work disability separately for the pre-event (years −4 to −1) and postevent (years 1–4) periods. RRs above 1 suggest an increasing trend, and RRs below 1 suggest a decreasing trend. These estimates (shown in online supplementary table 1) help to confirm whether changes in mean annual work disability days are statistically significant.
Supplemental material
To express the relative risk of work disability in the main diagnostic groups (circulatory, musculoskeletal, mental and diabetes) during the years after the IHD diagnosis in relation to the years before the diagnosis, we calculated RR and their 95% CI by contrasting the 4-year window after diagnosis (years 1–4) with the 4-year window before the diagnosis (years –4 to –1) adjusting for age, sex, education, type of living area, family situation, birth country, economic activity and medical treatment procedures at diagnosis. Moreover, we examined whether sex modified the risk of work disability in time by entering interaction term (sex×year) into the adjusted regression models. Year was entered as a categorical variable in the analyses. These analyses produced least square means. Their exponential functions were used to obtain adjusted annual means to demonstrate the adjusted absolute levels of work disability. The SAS V.9.4 was used for all analysis (SAS Institute).
If a person is permanently work disabled due to, for example, musculoskeletal disorders before the IHD event, this person remains on disability pension due to musculoskeletal disorders also after an IHD event. To control for these competing risks, and the fact that one person cannot be granted disability benefits for two different diseases simultaneously, we performed additional sensitivity analyses among a subcohort from which those on disability pension or long-term sickness absence (>730 consecutive days) before the event were excluded. We excluded 2411 women and 3910 men. Thus, 41% of women and 22% of men were permanently disabled from work before the IHD event. These results are presented in online supplementary figures 1 and 2.
Results
Of the study population with the first registered IHD diagnosis in 2006, 2007 or 2008 (n=23 971), 75% were men and 25% were women (table 1). Single parenting was more prevalent among women, and being married or single without children was more common among men. More men were more often born elsewhere than in Sweden while more women were economically inactive. Of the medical procedures, more men than women had had coronary artery bypass graft.
Characteristics of the study participants at the year of the ischaemic heart disease event
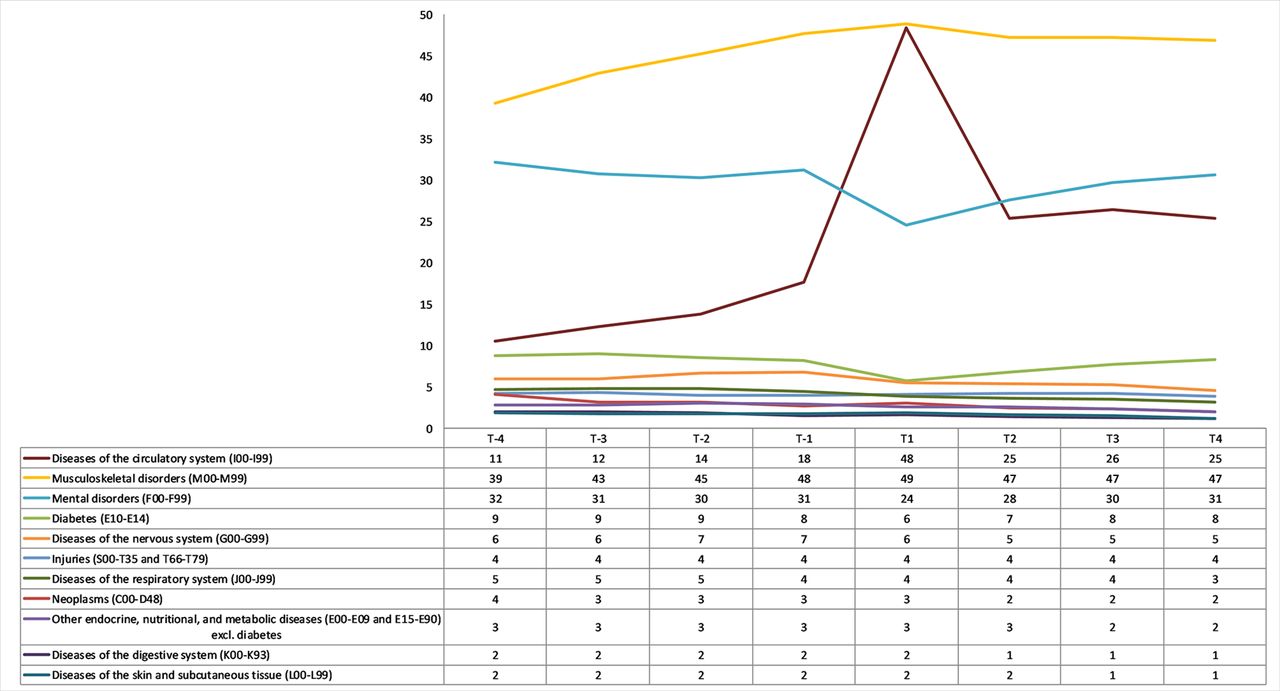
Figure 1 shows the observed (unadjusted) trends in work disability 4 years before and 4 years after the event among men with an IHD event. Before the event, the most common reasons for work disability were mental and musculoskeletal disorders (about 20 annual absence days). Work disability due to diseases of the circulatory system strongly increased (from 15 to 49 days; 3.3-fold increase) the year after the event from the year before, diseases of the circulatory system being the most common reason for work disability in the first postevent year. The average number of work disability days due to diseases of the circulatory system decreased from the first postevent year to the second postevent year (from 49 days to 21 days; being only 0.42 times the level observed in the first postevent year). From the second postevent year onwards, work disability due to diseases of the circulatory system and musculoskeletal disorders was on the same level (about 20 annual work disability days), and circulatory system and musculoskeletal disorders were the two most common reasons for work disability, followed by mental disorders (15–18 annual absence days).

Mean annual number of days of work disability before and after an ischaemic heart disease event among men (n=18 020) by the International Classification of Diseases, 10th revision diagnostic category. T-4 to T4 refer to four years before and four years after the ischeamic heart disease event.
Figure 2 shows the corresponding trends for women. As for men, before the event, the two most common reasons for work disability among women were mental (about 30 annual absence days) and musculoskeletal (about 40 annual absence days) disorders. While there was also a sharp increase in work disability due to diseases of the circulatory system among women in the first postevent year (from 18 to 48 days; 2.7-fold increase) from the year before, musculoskeletal disorders remained the most common reason for work disability during the whole follow-up, with 39–49 annual absence days. In the first postevent year, diseases of the circulatory system (48 days) were as prevalent diagnoses for work disability as musculoskeletal disorders (49 days), but musculoskeletal (47 days) and mental (about 30 days) disorders were the leading diagnoses for work disability during the years after this. Among women, the average number of work disability days due to diseases of the circulatory system decreased from the first to the second postevent year by 23 days (being only 0.52 times the level observed in the first postevent year), and remained at the same level until the end of follow-up.

Mean annual number of days of work disability before and after an ischaemic heart disease event among women (n=5951) by the International Classification of Diseases, 10th revision diagnostic category.
Online supplementary figures 1 and 2 show that when prior permanent work disability was excluded, diseases of the circulatory system were the most prevalent diagnosis of work disability after an IHD event among both men and women (men: T1: 47 days, T2–T4: 12–13 days; women T1: 53 days; T2–T4: 17–18 days). Postevent trend in work disability due to circulatory disease was rather similar in these sensitivity analyses than in the main analyses.
Online supplementary table 1 shows the statistical significance of annual trends in work disability before and after an IHD event stratified by sex in each diagnostic category. The trend in work disability among both men and women was increasing before the event due to diseases of the circulatory system (men: RR 2.09; 95% CI 1.93 to 2.25; women: RR 1.99; 95% CI 1.77 to 2.23), mental (men: RR 1.43; 95% CI 1.35 to 1.51; women: RR 1.35; 95% CI 1.25 to 1.45) and musculoskeletal (men: RR 1.38; 95% CI 1.32, 1.45; women RR 1.30, 95% CI 1.23 to 1.36) disorders. After the event, the trend was decreasing regarding diseases of the circulatory system (men RR 0.33; 95% CI 0.31 to 0.35; women RR 0.42; 95% CI 0.39 to 0.47) and musculoskeletal disorders (men RR 0.92; 95% CI 0.89 to 0.96; women RR 0.95; 95% CI 0.91 to 0.99).
Figure 3 shows the mean annual number of work disability days in the four most common diagnostic groups before and after an IHD event adjusted for confounding by demographic and socioeconomic factors and medical treatment procedures among men and women. In figure 3A, work disability due to diseases of the circulatory system increased even more sharply 1-year postevent among both sexes after adjustments. Among men, adjusted work disability days due to circulatory diseases increased from 12 to 60; a 5.2-fold increase in the last pre-event year compared with first postevent year. The corresponding increase was 4.4-fold among women (from 14 to 62 days). The decrease from the first to second postevent year was 3.2-fold (from 60 to 19 days) among men and 2.7-fold (from 62 to 23 days) among women. Among women, mean days of work disability due to diseases of the circulatory system remained at a higher level than those among men during the postevent years (postevent difference between women and men was about 4 days). As for the other diagnostic groups of musculoskeletal and mental disorders and diabetes (figure 3B–D), the trends were moderately increasing throughout the follow-up, with women consistently having more work disability days than men. IHD event did not impact the trend in other diagnostic groups.

{kind=link}
{kind=link}
{kind=link}
Adjusted mean annual number of days of work disability in the four most common diagnostic groups before and after an ischaemic heart disease (IHD) event among men and women. Error bars indicate 95% CIs. Models are adjusted for age, education, type of living area, family situation, birth country, economic activity and medical treatment procedures for IHD. Women are marked with dashed line, men with red line. Grey lines mark work disability trends in other diagnostic group. Arrow indicates the event time.
Table 2 demonstrates comparisons of the postevent period to the pre-event period as regard the risk of diagnosis-specific work disability among men and women. The risk of work disability increased after the event for disability due to diseases of the circulatory system, musculoskeletal disorders, mental disorders and diabetes among both sexes. We observed a statistically significant interaction of sex and year regarding work disability due to diseases of the circulatory system. Thus, while the absolute mean number of work disability days due to diseases of the circulatory system was higher among women than men during the postevent years, the relative increase in the risk of work disability was slightly higher among men than among women. This is due to a sharper increase in the first postevent year among men, illustrated in figure 3.
RRs with 95% CIs comparing risk of work disability after an IHD event to before in men and women
Discussion
This longitudinal study of all working-age individuals in Sweden who suffered their first IHD event in 2006‒2008 provided novel information on work disability diagnoses before and after an IHD event. We showed that before an IHD event, mental and musculoskeletal disorders were the most prevalent diagnoses, corresponding to those observed among the general population.23 The high prevalence of musculoskeletal disorder-related work disability after an IHD event, particularly among women, was explained by permanent work disability (disability pension) before the event. A total of 41% of women who had an IHD event were already permanently disabled from work prior to the IHD event. The corresponding figure for men was 22%. These percentages correspond to those previously reported in Finland24 and Sweden.12 After we excluded those who were permanently disabled from work prior to the event, diseases of the circulatory system were the most prevalent diagnosis of work disability after an IHD event, followed by mental and musculoskeletal disorders among both men and women. This corresponds to two previous studies on diagnoses for disability pensions after coronary interventions in Finland.7 25
Work disability due to diseases of the circulatory system increased considerably a year after an IHD event among both sexes, but this increase was slightly stronger among men. Work disability due to diseases of the circulatory system decreased to one-third from the first to the second postevent year. The end of work disability compensation can be viewed as a return to economic activity. In previous studies, 86% of patients with acute myocardial infarction returned to work in 1 year,26 65% of patients with acute coronary syndrome were working 5 years after diagnosis11 and 32% were on disability pension 5 years after a coronary revascularisation procedure.12 The trend in work disability among general population was stable during roughly the same time period.27
Our findings correspond to previous research on IHD comorbidity and the risk of work disability, which has linked musculoskeletal-related, mental-related and diabetes-related comorbidity to a higher risk of work disability among people with IHD.10–13 18 28 Our results do not indicate that comorbidity-related work disability increases due to an IHD event, but rather that pre-existing musculoskeletal and mental comorbidity may contribute to work disability after the event, as also suggested by recent case–control study.29 While the risk of mental-related and musculoskeletal-related work disability was higher after than before the event, the increase in work disability due to these diagnoses was rather stable throughout the follow-up, without an increase at the time of an IHD event as noted regarding the diagnostic group of diseases of the circulatory system.
We observed high levels of work disability due to musculoskeletal disorders before an IHD event, especially among women. Of musculoskeletal disorders, previous research has established a link between rheumatoid arthritis and a higher risk of IHD-related morbidity and mortality.30–32 Chronic inflammation may be the mechanism linking musculoskeletal disorders in general to IHD. The link between musculoskeletal disorders and IHD could also be due to uncontrolled confounding: the traditional risk factors of IHD, namely high body mass index, smoking, high alcohol consumption and lack of physical activity, may be over-represented among people with musculoskeletal disorders, and may be reasons for why they suffer more from IHD.33 34 This, however, warrants more research, as our register data did not include lifestyle-related information.
Mental comorbidity was also rather prevalent both before and after the IHD event, and was the third most common diagnostic group. Mental disorders combined with IHD may cause poor medication adherence,35 36 which may worsen the prognosis of IHD and future work capacity. The most prevalent mental diagnosis, depression, has also been associated with a higher risk of cardiovascular events, which corresponds to our findings regarding high levels of mental disorder-related work disability before the IHD event.37–39 Some evidence exists that IHD might predispose people to depression and other common mental disorders later in life,14 15 and depressed mood measured after admission has been linked to slower return to work after acute coronary syndrome.40
People with diabetes have a worse prognosis after revascularisation than people without diabetes,41 42 and diabetes itself also increases the risk of work disability.43 44 However, the most common diagnoses of work disability among people with diabetes are mental, musculoskeletal and cardiovascular,45 suggesting that diabetes combined with IHD is reflected in work disability due to diseases of the circulatory system rather than IHD being associated with worse prognosis of diabetes and diabetes-related work disability.
After an IHD event, work disability was more prevalent among women than among men, an observation also reported previously.18 26 We extended the previous research by examining the diagnoses for work disability, and found a consistent gender gradient across cardiovascular-related, musculoskeletal-related, mental-related and diabetes-related diagnoses. However, no diagnosis-specific sex difference was observed. Higher mortality and worse cardiovascular outcomes are observed in women with IHD than among men, especially among younger patients (<65 years and particularly <55 years). This is partially attributed to the incomplete use of secondary prevention treatment regimens,16 but may also related to physician who tend to underestimate cardiovascular risk in women, which may delay the diagnosis.17 Compared with men, women are at increased risk of adverse outcomes after coronary artery bypass graft and percutaneous coronary interventions.17 They are also at increased risk of bleeding from medical therapies used in acute coronary syndrome and the use of femoral access for percutaneous coronary intervention.16 In this study, the sex difference was not explained by the sociodemographic characteristics or treatment procedures investigated.
Strengths and limitations
The major strength of this study was the large population-based cohort data with reliable register-based measurements of high coverage and specificity,46 and no loss to follow-up. While there are no studies about the quality of register-based sickness absence data in Sweden, Danish registers have proven a valid measure.47 Generally, register-based data on sickness absence can be viewed as a golden standard compared with self-report data. However, it should be noted that the first 14 days of sick leave spells were not recorded in our data. These short-term sickness absences are most likely due to respiratory diseases, gastroenteritis and headache/migraine,48 and less likely due to circulatory diseases, mental or musculoskeletal disorders, which were the main diagnostic groups among people with IHD. We extended previous research by examining the diagnosis of work disability before and after an IHD event.
While we could include many confounders related to sociodemographic characteristics and treatment procedures, some residual confounding remained. We had no information on traditional cardiovascular risk factors or psychosocial work environment factors, which may possibly have explained the observed gender difference in work disability. Patients without hypertension had a higher likelihood of return to work than patients with hypertension.26 However, smoking, obesity, social support or financial strain have not been found to be significant predictors of return to work after acute myocardial infarction.26 Coronary artery bypass graft, percutaneous coronary intervention or other coronary surgeries associated with the IHD event were treated as a proxy for event severity. However, patients with most severe presentations are often treated conservatively because they are frail, have several impeditive comorbidities or have a severe coronary artery disease not amenable to revascularisation. Thus, more research on the impact of event severity is needed to make definite conclusions. Moreover, we had no information on quality and outcome of postevent care. In a previous German study, men were more likely to enrol in disease management programme than women after IHD event.49 Finally, it is possible that people have moved their place of residence or changed their marital status after the IHD event. However, we see this having minor impact on the results and subsequent conclusions.
Conclusions
We found that an IHD event was related to a sharp increase in work disability due to circulatory diseases, especially among men and particularly in the first postevent year. Women had more IHD-related and comorbidity-related work disability after the event than men. Occupational healthcare and other healthcare professionals, who monitor sickness absence, may benefit from such knowledge.
References
Footnotes
Contributors JE, TL, MV, EM-R and KA contributed to conception and design. JE analysed the data and drafted the manuscript. MV, TL, EF, EM-R, EL and KA contributed to interpretation of the results and critically revised the manuscript. All gave final approval and agree to be accountable for all aspects ensuring integrity and accuracy.
Funding This work was supported by Forskningsrådet om Hälsa, Arbetsliv och Välfärd (The Swedish Research Council for Health, Working Life and Welfare). JE, MV and TL were supported by Suomen Akatemia (Academy of Finland), project numbers 258598, 292824, 287488, 294096.
Competing interests None declared.
Patient consent Not required.
Ethics approval The project was approved by the Regional Ethical Review Board, Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.