Article Text

Abstract
Objectives Investigate the effectiveness of a complex intervention aimed at improving the appropriateness of medication in older patients with multimorbidity in general practice.
Design Pragmatic, cluster randomised controlled trial with general practice as unit of randomisation.
Setting 72 general practices in Hesse, Germany.
Participants 505 randomly sampled, cognitively intact patients (≥60 years, ≥3 chronic conditions under pharmacological treatment, ≥5 long-term drug prescriptions with systemic effects); 465 patients and 71 practices completed the study.
Interventions Intervention group (IG): The healthcare assistant conducted a checklist-based interview with patients on medication-related problems and reconciled their medications. Assisted by a computerised decision support system, the general practitioner optimised medication, discussed it with patients and adjusted it accordingly. The control group (CG) continued with usual care.
Outcome measures The primary outcome was a modified Medication Appropriateness Index (MAI, excluding item 10 on cost-effectiveness), assessed in blinded medication reviews and calculated as the difference between baseline and after 6 months; secondary outcomes after 6 and 9 months’ follow-up: quality of life, functioning, medication adherence, and so on.
Results At baseline, a high proportion of patients had appropriate to mildly inappropriate prescriptions (MAI 0–5 points: n=350 patients). Randomisation revealed balanced groups (IG: 36 practices/252 patients; CG: 36/253). Intervention had no significant effect on primary outcome: mean MAI sum scores decreased by 0.3 points in IG and 0.8 points in CG, resulting in a non-significant adjusted mean difference of 0.7 (95% CI −0.2 to 1.6) points in favour of CG. Secondary outcomes showed non-significant changes (quality of life slightly improved in IG but continued to decline in CG) or remained stable (functioning, medication adherence).
Conclusions The intervention had no significant effects. Many patients already received appropriate prescriptions and enjoyed good quality of life and functional status. We can therefore conclude that in our study, there was not enough scope for improvement.
Trial registration number ISRCTN99526053. NCT01171339; Results.
- multimorbidity
- multiple chronic conditions
- polypharmacy
- medication reconciliation
- computer-assisted drug therapy
- Medication Appropriateness Index
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- multimorbidity
- multiple chronic conditions
- polypharmacy
- medication reconciliation
- computer-assisted drug therapy
- Medication Appropriateness Index
Strengths and limitations of this study
The Prioritising Multimedication in Multimorbidity (PRIMUM) intervention was developed and piloted in accordance with the latest Medical Research Council guidance on complex interventions.
The effectiveness of the PRIMUM intervention was evaluated in a rigorously conducted cluster randomised trial that involved random sampling of patients, disclosure of treatment allocation after baseline completion and adherence to the protocol.
To evaluate the generic patient-centred strategy of applying PRIMUM, we used the commonly used Medication Appropriateness Index (MAI), as this implicit measure allows individualised assessments.
We blinded both the assessment of the primary outcome MAI and the statistical analyses.
Key limitations were that the baseline values of MAI and the secondary outcomes did not provide enough scope for improvement, and that medication underuse in polypharmacy was not sufficiently reflected in our outcome measures.
Introduction
The prevalence of multimorbidity, that is, the co-occurrence of multiple chronic or acute diseases and medical conditions in one person,1 increases with age, and most primary care consultations currently involve patients with multiple conditions.2–4 Multiple disorders in patients are likely to result in multiple drug prescriptions. This increases the risk of drug–drug and drug–disease interactions, inappropriate dosages or drug selection and non-adherence of patients. They may, however, also result in undertreatment.5–10 Inappropriate prescriptions may result in hospitalisations, falls and related injuries, decreased quality of life, cognitive and physical dysfunction, loss of autonomy and increased mortality, particularly in the elderly.6–8 11–14 Negative health outcomes caused by inappropriate polypharmacy are responsible for high outlays for hospital treatment, home care and nursing homes.15–17 Much morbidity and many costs may be preventable—for instance, 20%–50% of medication-related hospitalisations on internal wards have been estimated to be avoidable.13 16 18–20 Recently, Dreischulte and coresearchers observed a reduction in hospital admission rates for gastrointestinal ulcers or bleeding in their trial evaluating a complex intervention addressing nine specific high-risk prescribing patterns such as non-steroidal anti-inflammatory drugs in renal failure, or in combination with oral anticoagulants.21 Further trials also evaluated interventions addressing safety indicators and achieved a reduction in high-risk prescribing through adherence to explicit criteria that are relevant to public health.22 23 However, ‘the range of reported effect sizes was modest, and it is unclear whether such interventions can result in clinically significant improvements in patient outcomes.’24
Furthermore, considering there are more than 10 000 known diseases, the number of possible interactions between diseases and treatments in patients with multimorbidity is vast, and patients may not be able to cope with the treatment burden.25 Generic patient-centred strategies to assess potential interactions and to prioritise and individualise management in accordance with patients’ preferences and shared treatment goals have been recommended for patients with multimorbidity and polypharmacy.26–32 In these patients, evidence of interventions with proven effectiveness on clinical outcomes remains scarce. However, recent Cochrane reviews have identified strategies that appear to be beneficial in terms of reducing inappropriate prescribing.33 34 Based on promising strategies to combat inappropriate polypharmacy and in accordance with guiding principles to manage patients with multimorbidity, we developed and piloted a complex intervention.35 As the prevalence of multimorbidity and polypharmacy in older people is high, they made up the target population. To reduce the workload on the general practitioner (GP), the intervention also involved a healthcare assistant (HCA) from the practice.35 In Germany, HCAs receive less training than nurses and are comparable to certified medical assistants in the USA. In usual care, HCAs work as receptionists, assist GPs (eg, in diagnostic procedures or wound management) and conduct, for instance, dietary counselling. On many occasions, HCAs have successfully participated in chronic care interventions where they have, for example, surveyed patients by following protocols with fixed interview questions for conditions such as osteoarthritis, major depression and chronic heart failure, under the supervision of GPs.36–40
In accordance with the Medical Research Council (MRC) guidance on developing and evaluating complex interventions, we tested the feasibility of the complex intervention in a pilot study.35 On the basis of overall feasibility findings, we improved the intervention and trial design. To compare the effectiveness of the complex Prioritising Multimedication in Multimorbidity (PRIMUM) intervention with usual care in older patients with multimorbidity and polypharmacy in general practice, we used the Medication Appropriateness Index (MAI) as primary outcome. This implicit (non-criteria-based) measure allows an individualised assessment of medication appropriateness.41–43 We investigated whether the appropriateness of drug prescriptions changed after 6 months’ follow-up measured as a difference in the MAI score 6 months from baseline minus baseline (MAI T1−T0).
Methods
Study design
The study was a pragmatic, cluster randomised controlled trial (RCT) with the general practice as the unit of randomisation. To further reduce contamination of the control group and unlike the pilot study, detailed information on the intervention treatment was only provided to the intervention group.35 Primary and secondary outcomes were measured at patient level (figure 1 44–69 and online supplementary appendix 1: study protocol).
Supplementary file 1

PaT Plot70 of the Prioritising Multimedication in Multimorbidity (PRIMUM) trial. †Structured symptoms of side effects: dizziness, dyspnoea, tachycardia/palpitations, nausea/vomiting, abdominal pain, bleeding diathesis, difficulties urinating, ankle oedema—frequency expressed as occurrence on 1 day/several days/almost every day during the past 2 weeks. CDSS, computerised decision support system.
Setting and participants
General practices in the German state of Hesse were eligible if they provided primary care under the German statutory health insurance system, and if at least one of the HCA staff members was able to access the internet in the practice. Practices specialising in unconventional treatments or in special indications (eg, HIV) were excluded. To recruit practices, we sent letters to about 1600 practice addresses provided by the Association of Statutory Health Insurance Physicians of Hesse—addressees were not exclusively active GPs. We checked inclusion and exclusion criteria for those who were interested by phone and agreed upon a time for investigator training (figure 1: icon ‘1’). In both groups, GPs and HCAs received a lump sum of €300 in recompense for the work involved in documenting results. In the intervention group, GPs and HCAs received an additional €150 for the extra work that the intervention entailed.
GPs who did not respond to the original letter received a reminder phone call. We phoned a random 10% sample of those who did not respond to either the letter or the reminder up to three times in order to collect data on inclusion and exclusion criteria, practice characteristics and reasons for non-participation.
Patients: A random sample of seven patients per practice were included (figure 1, patient recruitment, icons ‘c’ to ‘e’). Patients were required to be ≥60 years old, have ≥3 chronic conditions under pharmacological treatment, ≥5 long-term prescriptions of drugs with systemic effects (the medication regimen may have included drugs with local effects but these did not fulfil the inclusion criterion), have made ≥1 practice visit during the past quarter and be able to fill in questionnaires and participate in telephone interviews. To include a greater number of patients at risk of (manageable) interactions than in the pilot study,35 patients had to have diseases affecting at least two different organ systems operationalised as two different chapters of the International Classification of Diseases, 10th Revision. The chapters ‘H’ (diseases of the eyes and ears) and ‘E00’ to ‘E04’ (diseases of the thyroid gland without hyperthyroidism) were not counted because their potential for systemic interactions was considered to be low. We excluded patients with dementia and cognitive impairment (Mini-Mental Status Examination <26),47 because we designed our intervention for cognitively intact patients and did not target caregivers. Further exclusion criteria were a life expectancy ≤12 months, alcohol and drug abuse (based on the GP’s assessment) or participation in another clinical trial 30 days prior to inclusion.
Randomisation, allocation concealment and blinding
The first patient from each practice served as the basis for randomisation (figure 1, icon ‘i’). Patients registered thereafter were treated according to practice status (control or intervention), which was assigned in an allocation ratio of 1:1 using a block randomisation of variable block length. At the study centre, an external researcher generated the allocation sequence using the random number generator of Microsoft EXCEL. Treatment allocation was disclosed to the practice after baseline completion. Owing to the nature of the intervention, it was not possible to blind GPs, HCAs, patients and the study team. Treatment allocation was blinded to the clinical pharmacologist conducting medication reviews for the primary outcome (MAI) and to the statistician.
Intervention and control groups
Intervention group
The PaT Plot70 (figure 1, icons ‘j’ and ‘3’ to ‘5’) shows the four elements of the complex intervention. It consists of (1) a brown bag review and (2) a checklist-based preconsultation interview with the patient that is conducted by the HCA (online supplementary appendix 2), (3) a computerised decision support system (CDSS)-assisted medication review carried out by the GP, and (4) a GP–patient consultation to optimise and prioritise medication. GPs had the option to use the CDSS to help prepare the medication review with the patient, and during the consultation itself. Trained HCAs and GPs (figure 1, item ‘2’) implemented the intervention on a single occasion, which took the GP and the HCA a per-patient average of 35 and 45 min, respectively.35 The practice team for the intervention group received the GP guidelines for ambulatory geriatric care prepared by the Hesse Guideline Group (figure 1, item ‘k’). Recommendations in the guideline focus on primary and secondary prevention (eg, physical exercise, fall assessment and prevention).46
Supplementary file 2
Outcomes
The primary outcome was the difference in MAI sum score41 71 at 6 months minus the corresponding baseline score (MAI T1−T0). The MAI is commonly used in RCTs42 43 and consists of 10 items: indication, effectiveness, correctness of dosage, correctness of direction, practicality of direction, drug–drug interactions, drug–disease interactions, unnecessary drug duplications, correctness of treatment duration and costs. The MAI item on cost was omitted because variable discount contracts between pharmaceutical companies and statutory health insurers preclude cost comparisons in Germany. The medication reviews were conducted by the same clinical pharmacologist (SH) who performed the pilot study. He rated nine items per prescription from ‘1’ (appropriate) to ‘3’ (inappropriate) where ‘2’ represents a middle rating of uncertain appropriateness in a blinded chart review. In line with the piloted procedures,35 he coded the MAI according to the GP’s prescriptions, renal function, electrolytes, multimorbidity (diagnoses, Cumulative Illness Rating Scale)44 45 (figure 1, icon ‘f’) and symptoms of adverse drug reactions (ADR) (figure 1, icon ‘h’). Phytopharmaceutical, homeopathic and other complementary medicine products were excluded from the rating. MAI sum scores for the entire medication regimen were calculated on the basis of these ratings. Based on the intrarater reliability of the MAI ratings in the pilot study (B statistics: the intrarater reliability for the nine MAI items ranged from 0.90 to 0.99 and was slightly better than inter-rater reliability),35 we did not perform a duplicate MAI rating. MAI ratings were transformed by subtracting 1 from the original rating, resulting in values ranging from ‘0’ (best rating) to ‘2’ (worst rating), and summed to give an MAI score per prescription (theoretically ranging from 0 to 18) and across the entire medication regimen of the patient. Lower MAI sum scores denoted better prescribing appropriateness. A negative difference in MAI sum scores (MAI T1−T0) therefore reflected an improvement in prescribing quality.
Secondary outcomes (6 vs 9 months): we measured the change in the MAI score after 9 months (MAI T2−T0). On the assumption, improved medication appropriateness would result in improved health-related quality of life and functional status, we measured the differences in the EuroQol five dimensions (EQ-5D) index score,48 49 changes in perceived future life expectancy (a quality of life-related concept indicating well-being and positive life evaluation measured in years of expected and desired lifetime duration),52 53 functional status (differences in Vulnerable Elderly Survey-13 items),50 all-cause hospitalisation and severity of chronic pain (von Korff Index)51 after 6 and 9 months (T1−T0 and T2−T0).
To explain intervention effects, we also measured changes in satisfaction with shared decision-making (Man-Son-Hing Scale)54 55 and medication adherence after 6 and 9 months (T1−T0 and T2−T0). We investigated (A) self-reported adherence in accordance with Morisky (low scores indicating good adherence)62; (B) ‘observed adherence’ measured in terms of discrepancies between medicines actually taken (reported during patient interviews) and medicines prescribed (reported by GP), as expressed in the three scores developed by Barat et al.72 The scores were based on ratios calculated as follows:
The drug score representing the ratio of the number of drugs reported by the patients to the number of drugs reported by the GP.
The dose score (DoS=d1(a1)+d2(a2)+d3(a3)+…/n), where di is the drug used by the patients (value 0 or 1), n is the number of drugs in the GP’s report, and ai is the dose-deviation ratio calculated by dividing the patient’s reported daily dose by the daily dose prescribed by the GP.
The regimen score (RS=d1(b1)+d2(b2)+d3(b3)+…/n), where bi is the regimen-deviation ratio and calculated by dividing the patient’s reported daily intake frequency (once daily, twice daily, and so on) by the corresponding frequency prescribed by the GP.72
Scores outside an interval of 0.8–1.2 were considered to be divergent.
Further adherence-related measures assessed the complexity of the medication (total number of prescriptions, number of single doses/day and Medication Regimen Complexity Index),73 patients’ beliefs and attitudes towards medication (Beliefs about Medicine Questionnaire),56 57 cognitive function (verbal fluency test, VFT)59 and depressive symptoms (Geriatric Depression Scale, GDS).60 61 GDS and VFT will be reported elsewhere.
Sample size
Based on the results obtained in previous studies,35 74 a difference in the change values (MAI T1−T0) of at least 2 units between the treatment groups was considered clinically relevant. Based on the pilot study, an SD of 6 units was expected, resulting in a Cohen’s effect size d of 0.3 and representing a small effect size.75 Assuming an intracluster correlation coefficient (ICC) of 0.03 at practice level76 and an average cluster size of seven patients, a total of 62 practices and 434 patients (31 practices and 217 patients per treatment arm) were required to detect such an effect with 80% power using a two-sample t-test at a two-sided significance level of α=0.05. The sample size calculation was performed using NCSS Statistical Software ’PASS 2008'TM (inequality tests for two means in a cluster randomised trial). On the basis of an assumed drop-out rate of approximately 10%, the sample size was adjusted to a total of 70 practices and 490 patients (35 practices and 245 patients in each treatment group).
Statistical analysis
We performed descriptive analyses of the primary endpoint, the secondary endpoints, and all patient and practice characteristics (separately for patients in both groups) and calculated mean and SD for continuous variables, and relative and absolute frequencies for categorical data.
In the primary analysis and using a two-sided significance level of α=0.05, we tested the null hypothesis H0: μ1=μ2 (the mean difference MAI T1−T0 is the same in both groups) against the alternative hypothesis H1: μ1≠μ2 (the mean MAI T1−T0 differs). Because of cluster randomisation, we used a multilevel regression approach with patients at level 1 and practices at level 2. The primary model included treatment group and MAI baseline as fixed factors and practice as a random factor. In a mixed model, estimates are adjusted for the correlation of observations on the same level, where a specific structure has to be chosen. We applied the compound symmetry correlation structure on the assumption that a correlation exists between patients from the same practice and that a specific numerical value can be attached to this correlation. We assumed the value was 0 for the correlation with patients from other practices. The results are presented as the adjusted mean between-group difference in MAI T1−T0 with the corresponding 95% CI. In addition, the practice-related ICC was estimated. The primary analysis was performed in accordance with the intention-to-treat (ITT) principle,77 and additional sensitivity analyses were conducted on a per-protocol analysis set. In the multilevel approach, we made use of the missing at random assumption that the baseline or the treatment variable can explain missing data in the response. No additional imputation of missing data was conducted. In a sensitivity analysis, we replaced missing values for the primary endpoint using the baseline observation carried forward (BOCF) approach. The statistical analyses of the secondary endpoints used the same multilevel approach as the primary analysis. A linear, binary or Poisson mixed model was fitted in accordance with the scaling of the considered endpoint. The obtained P values in the secondary analyses are only interpreted exploratively. All evaluations were carried out using software package R (V.2.15.0 and higher),78 in combination with the R packages xtable,79 nlme,80 lme4,81 multilevel82 and psychometric.83
Results
Participant flow and non-responders
Of the 1662 practice addresses we sent letters to (1332 of them also received a phone call reminder), 1325 did not reply at all, 102 answered but were not interested in further information and 235 general practices asked for further details and were assessed for eligibility. Of those, 153 practices finally declined to participate, 3 did not meet inclusion criteria and 7 were not able to create screening lists using their practice computer. Of the 72 included practices, 3478 IDs for potentially eligible patients were provided, from which a random sample of 1346 IDs was drawn at the study centre and sent to the practices. In total, 505 patients were consecutively included from the random sample and 465 completed the study (intervention group 238/252, control group 227/253) (flow chart: online supplementary appendix 3).
Supplementary file 3
Of the 1325 practices that did not reply, we called 132 randomly selected practices. Six practices did not answer the phone, 51 were willing to answer all questions and 75 provided partial information. Sixty-one interviewed practices (48%) were not eligible (7 were not active GPs, 51 had no internet access and 3 declined to say). Practice characteristics and reasons for not responding are provided in online supplementary appendix 3.
Baseline characteristics of participants
Most practices were single handed (57%), medium sized (64%) and located in small to mid-sized towns (57%). Slightly more male GPs (57%) participated; they were either specialists in general practice (83%) or in internal medicine. On average, they were 51 years of age, had more than 23 years of clinical experience and had worked in private practice for about 15 years. With one exception, HCAs were female. They averaged about 40 years of age, had about 17 years of clinical experience and had worked in the practice at various employment levels (49% less than full time) for an average of 10 years. About three-quarters were qualified HCAs. Patients were slightly more often female (52%), had a median age of 72 years and averaged eight prescriptions in nine single doses per day. Almost all patients were covered by statutory health insurance (96%), and looked after themselves (94%). Fifty-eight per cent participated in one of the national disease management programmes (DMP). Overall, baseline characteristics were well balanced in both groups (table 1).
Baseline characteristics of practices and patients
Outcomes
Our study found the intervention to have no significant effect. The mean MAI sum scores had decreased minimally in both groups 6 months after baseline—by 0.3 points in the intervention group and 0.8 points in the control group—revealing a non-significant adjusted mean difference of 0.7 (95% CI −0.2 to 1.6) points in favour of the control group (ITT, per-protocol analysis and BOCF approach did not differ). To control for the effects of oversampled patients registered in a DMP, we compared DMP participants with non-participants, which revealed no effects on MAI. Furthermore, sociodemographic factors did not have an influence (table 2).
Intention-to-treat analysis of primary and secondary outcomes and sensitivity analyses
To explore our results, we conducted additional, non-prespecified analyses. As the sample size was not sufficiently large to perform subgroup analyses, we calculated multilevel models, which revealed strong effects of the baseline values of MAI sum scores on the primary outcome MAI T1−T0 (P<0.001) (figure 2A). The figure also shows the low proportion of patients with high inappropriateness at baseline, and the size and direction of the MAI changes in both groups after 6 months. To explain the relationship between the number of prescriptions and MAI values, we conducted exploratory regression analysis, which approximately revealed a square function (figure 2A).

Distribution and changes in the MAI using baseline values and number of prescriptions. (A) Changes in MAI scores in intervention and control groups 6 months after baseline compared with baseline values (absolute numbers of study participants and boxes and whiskers per subgroup are provided). (B) MAI scores at baseline in terms of the number of prescriptions (higher diameters of drops represent higher numbers of study participants).
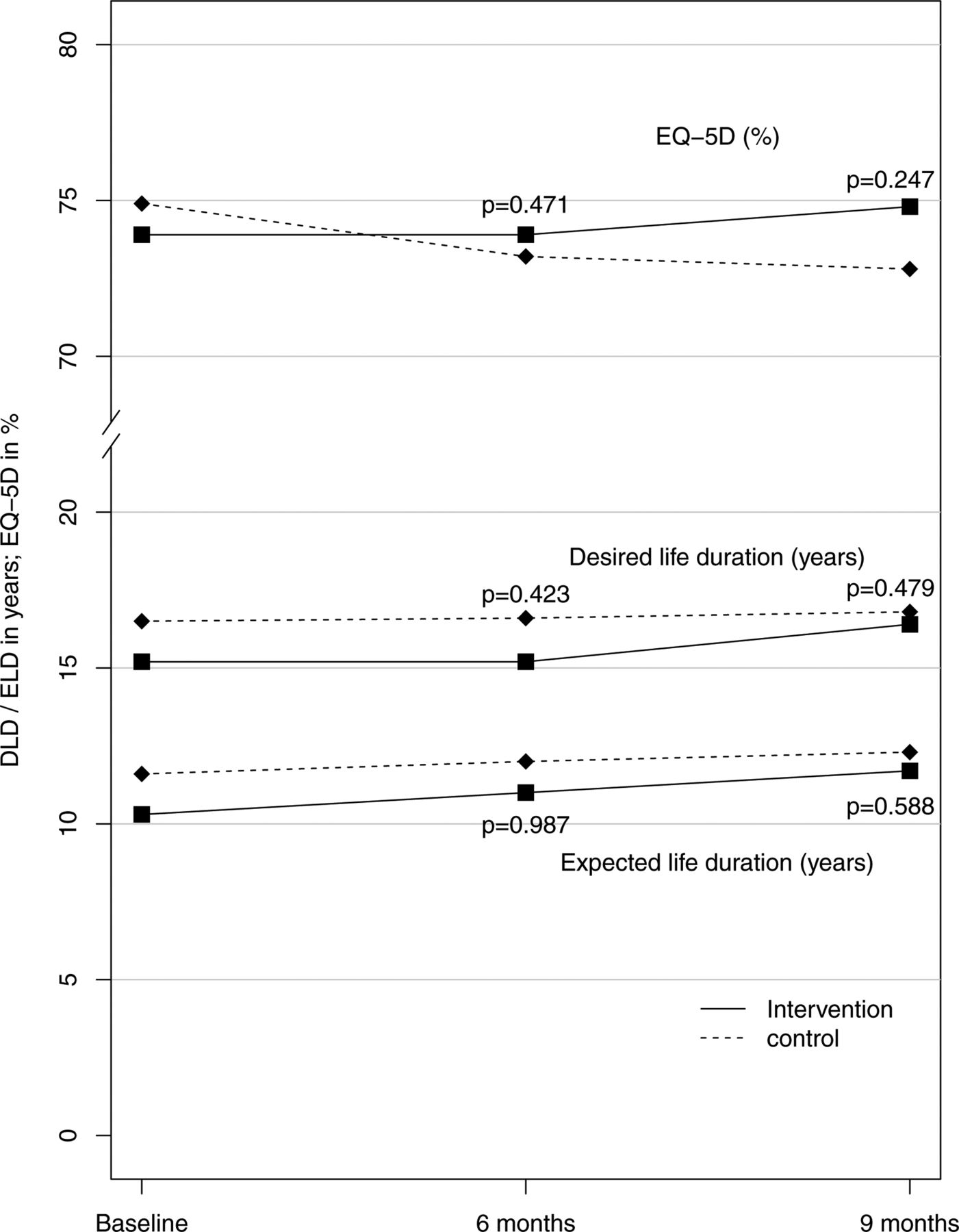
Secondary outcomes showed small, non-significant changes. In the intervention group, patients’ self-reported quality of life improved minimally (about 2.3% in EQ-5D, 0.5 years in both expected and desired lifetime) after 6 and 9 months, whereas it continued to decline in the control group (figure 3). Additionally, in the intervention group the mean number of hospital stays decreased and the mean number of days spent in hospital had dropped by half after 6 months, but in both groups the event rate was too small to show significant differences (ITT analyses of the primary and secondary outcomes: table 2, descriptive analysis of symptoms for potential ADRs: online supplementary appendix 4).
Supplementary file 4

{kind=link}
{kind=link}
{kind=link}
Secondary outcomes related to patients’ self-reported quality of life measures. DLD, desired life duration; ELD, expected life duration; EQ-5D, EuroQol five dimensions.
Discussion
Key findings of the study
This study found the complex PRIMUM intervention to have no significant effects in older patients with multimorbidity and polypharmacy in general practice. At baseline, many patients already received appropriate prescriptions and enjoyed good quality of life and functional status. We can therefore conclude that in our study, there was not enough scope for improvement.
Strengths and limitations of study
The systematic development and stepwise evaluation of the PRIMUM intervention in accordance with MRC guidance on complex interventions84 was a strength as demonstrated by refinements in the design of the main trial, based on the results of pilot testing.35 Recruitment to target, random sampling of patients, minimal attrition (we lost one cluster to follow-up because the GP moved to another town) and adherence to the protocol are additional strengths when compared with previous studies.85 86 However, our study also had several limitations.
First, there is no agreed definition of polypharmacy and patient inclusion at the numerical threshold of ≥5 prescriptions was somewhat arbitrary,87 88 but using a higher threshold would have meant losing patients whose medication was highly inappropriate (figure 2B). Moreover, the association between the number of prescriptions and health outcomes is not linear: Payne and coauthors found only the most extreme levels of polypharmacy to be associated with increased admission rates in patients with multimorbidity,89 while Gnjidic and her coresearchers identified the best discriminating threshold to be between 4.5 and 6.5 medicines for associations with frailty, disability, mortality and falls.90
Second, our study population may limit the generalisability of the results. Our study was population based and involved no preselection, and the response rate of practices was low. We cannot rule out that relatively ambitious GPs volunteered more frequently. As far as the choice of patients is concerned, we took a random sample within each practice and our selection criteria aimed at including a broad range of diseases involving as many organ systems as possible. We applied the cognition test during recruitment and after consent. As our ultimate aim was to promote regular practice consultations, we excluded patients with dementia. The study required that patients who were unable to fill in questionnaires or to answer telephone calls should not attend (eg, some nursing home residents and migrants). These groups may therefore have been under-represented. To enable random sampling, we applied a systematic case finding using prescription costs as a proxy but oversampled DMP participants. However, German DMPs do not address multimorbidity or polypharmacy and we did not find any DMP impact on outcomes in our study.
Third, our outcome measures were slightly insensitive. In the intervention group, the increase in the average number of prescriptions indicates that GPs had more often begun to prescribe patients a new medicine. If undertreatment had been a key problem in our study, having the MAI as the main outcome variable would have led us to underestimate its impact, because it does not reliably detect underuse.42 It is noteworthy that the number of medicines used in intervention and control groups had diverged after 6 and 9 months, with the adjusted mean number of drugs being 1.0 higher in the intervention group (table 2). Figure 2B shows that the more drugs a physician prescribes, the greater the chance that the MAI score will increase. The intervention may have induced increased prescribing of medicines (eg, in case of otherwise undetected underuse), which may explain the trend towards smaller reductions of the MAI scores in the intervention group.
Fourth, our efforts to reduce contamination of controls by using a cluster randomised design and withholding intervention details may have been substantially offset by a potentially important Hawthorne effect, as has been noted in other studies.85 91 GPs and HCAs collected extensive data on medication, diseases and laboratory parameters (see icon ‘f’ in figure 1) at each study visit. It can be assumed that data collection will have had the same effect as the structured medication reviews: we also observed improvements in MAI mean values in the control group at the first follow-up (figure 2A), and a slight decrease in the average numbers of prescriptions. The net effect was that the decrease in MAI scores in the control group was slightly larger than in the intervention group where it had been partly offset by an increase in the number of prescriptions (and higher MAI scores) resulting from identified underuse. However, the differences were very small.
Comparison with other studies
Most primary care studies have investigated pharmacist-led interventions, and have shown inconclusive results in various outcomes.33 92–96 However, pharmacist-led interventions may be difficult to implement in healthcare contexts in which pharmacists have no access to clinical information (eg, patients’ diagnoses, laboratory tests), patients often visit many different pharmacies and interprofessional relationships between GPs and pharmacists are not well established, as in Germany.85 86 In this context in particular, information technology systems have been identified by European GPs as supporting safer prescribing.97–99 Further factors that have been addressed include support from other healthcare professionals such as nurses, systematic medication reviews and greater involvement of the patient.97–99 However, the efficacy of these measures is inconclusive: Olsson and coinvestigators found that a physician-led medication review had no effect on indicators of high-risk prescribing in older patients with polypharmacy.100 In contrast, a large-scale cluster RCT achieved reductions in unintentional drug duplications, drug–drug interactions and new prescriptions of potentially inappropriate medications, but failed to show an impact on the discontinuation of inappropriate medicines.101
No evidence yet exists that polypharmacy interventions lead to decrease in mortality and hospitalisations,94 functional decline and falls102 103 and health-related quality of life.85 86 100 104–107 A recent meta-analysis revealed a modest reduction in the number of drugs (on average −0.2 in the intervention group vs +0.2 in controls) but the results of the included studies differed widely94 and, considering the frequency and potential impact of medication underuse,6–8 a reduction in net prescription numbers is an ambiguous study endpoint.
Possible explanations and implications of the study
Our study showed the intervention to have no significant effect. We cannot rule out that there was not enough scope for improvement in our study (figure 2A: the MAI of the patients included in the left two box plots in both groups could not improve). Additionally, there was a relevant Hawthorne effect (figure 2A: the patients included in the four box plots of the control group on the right hand side also improved). The patients depicted in the four box plots of the intervention group on the right hand side (figure 2A) improved less than corresponding patients in the control group, which probably reflects the small numbers of patients and the lack of an intervention effect. In addition, given the MAI’s inability to detect changes in inappropriate underuse, it may have not been sensitive enough for the purpose of our study. As any newly prescribed drug worsens the MAI score, unless it is completely appropriate, this may at least partially explain the difference. Ongoing process evaluation concerning medication changes may provide further explanations of the outcomes and information on the implications of the study.
Further research is needed to identify patients who stand to benefit significantly from an intervention that aims to support the care of complex patients with multimorbidity and high treatment burden.108 109 Future studies may also benefit from considering a refined choice of outcome measures that adequately takes underuse into account.
Conclusion
We did not find the intervention to have significant effects. Many patients already received appropriate prescriptions and enjoyed good quality of life and functional status. We can therefore conclude that in our study, there was not enough scope for improvement. Further research should seek to identify groups of patients who are most likely to benefit from such resource-intensive interventions. Outcome measures should be patient relevant and detect changes in underuse.
Acknowledgments
The authors thank all participating patients and all general practice investigators and their teams. The authors are grateful to our dedicated research team Petra Lödige, Zeycan Albay, Mareike Leifermann, Anja Paesel and Natalie Aksamit, as well as to the team who was involved in developing and programming the study version of the CDSS, namely Kristina Zint, Diana Witticke, Jens Kaltschmidt and Michael Metzner. The authors also thank our practice advisory board Joachim Fessler, Joachim Seffrin, Karola Mergenthal and Vera Müller. This study was only possible thanks to their extraordinary engagement. The authors thank Cornelia Mahler for the provision of the German version of the BMQ and Roman Kaspar for his advice on quality of life measures in gerontology. The authors also thank Professor Paul Glasziou from CREBP, Bond University, QLD, Australia, for his comments on a former version of the manuscript.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
Footnotes
Contributors CM drafted the manuscript, coordinated the study and contributed to the conception, design, data collection and data analyses. SH contributed to the conception and design, and conducted the MAI ratings. FMG was the guarantor of the study. JR and LU contributed to the conception and design, and conducted the data analyses. WEH contributed to the conception and design, and provided the study version of CDSS. CG, MB, FO, RP, MvdA, JAK, JMV and FMG provided specific advice on the conception, methods and coordination of the study. All authors critically revised and agreed on the final version of the manuscript.
Funding Funding has been provided by the German Federal Ministry of Education and Research, BMBF (grant number 01GK0702).
Competing interests CM, FMG, CG, MB, SH, WEH, JR and LU report receiving grants from the German Federal Ministry of Education and Research, BMBF, grant number 01GK0702, during the course of the study. WEH reports other grants from Dosing, Heidelberg, during the course of the study; he received personal fees, non-financial support and other from Aqua Institute Göttingen; personal fees, non-financial support and other from Aspen Europe; personal fees and other from Diaplan; grants, personal fees, non-financial support and other from Actelion; personal fees and other from GSK GER/UK/Slovakia/France; personal fees from Thieme Verlag; personal fees and other from Daiichi Sankyo; personal fees and other from Bristol-Myers Squibb; personal fees and other from MSD Sharp & Dohme; personal fees and other from AstraZenica; personal fees and other from Boehringer; personal fees and other from Grünenthal; personal fees and other from KWHC; personal fees and other from Novartis; personal fees and other from Berlin-Chemie; grants, personal fees and other from Landesapothekerkammer BW; grants and other from BMBF (DZIF, ESTHER); grants, personal fees, non-financial support and other from BayerPharma; grants from CHIESI; personal fees and other from Doctrina Med; personal fees and other from GSK France, UK, Germany, Slovakai; personal fees, non-financial support and other from Pfizer; grants from Smooth ClinicalTrials; grants from Sumaya Biotec; grants from Klaus Tschira Stiftung; other from University Frankfurt; grants from Vaximm, outside the submitted work. FO, MvdA, JMV, RP and JAK have nothing to disclose.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.
Presented at Oral presentations and posters: Muth C, Uhlmann L, Haefeli WE, Rochon J, van den Akker M, Beyer M, Perera R, Knottnerus A, Gerlach FM, Harder S (2014). PRIorisierung von MUltimedikation bei Multimorbidität (PRIMUM)* Cluster-RCT in Hausarztpraxen zeigte keine Effekte auf die Angemessenheit der Verschreibung. 48. Kongress der DEGAM, 18; 20 September 2014, Hamburg; Abstractband V3c | 3, S. 88. Muth C, Rochon J, Namyst A, Fullerton B, Harder S, van den Akker M, Perera-Salazar R, Gerlach FM, Beyer M. Anwendung der MRC Guidance in der allgemeinmedizinischen Forschung: Ergebnisse aus der PRIMUM-Studie (PRIorisierung von MUltimedikation bei Multimorbidität). Vortrag auf 13. Jahrestagung des Deutschen Netzwerks Evidenzbasierte Medizin, Hamburg, 15; 17 March 2012, Abstractband IV/1a.